Transcription
“Practicing in the Grey Zone discussed the implications of working from a Dialogic OD mindset, along thecontinuum of diagnostic to dialogic methodologies used in the field. This sequel presents another casestudy in which working in the grey zone was successfully addressed to achieve positive outcomes.”Practicing in the Grey AreaBetween Dialogic and DiagnosticOrganization DevelopmentLessons from Another Healthcare Case StudyBy Yabome Gilpin-Jacksonwith Melissa CrumpIn 2013, the Practicing in the Grey Zonearticle was published outlining howOrganization Development’s third generation methodologies, that are anchored insocial constructivist thinking and respondto our current complex systems, usheredin the era of Dialogic OD. Since then, theliterature and exploration of Dialogic ODhas expanded, most notably with the bookDialogic Organization Development: TheTheory and Practice of TransformationalChange of which I was a contributingauthor. In that volume and in their otherwritings, Marshak and Bushe generallydefine Dialogic OD as a mindset and practice of Organization Development throughwhich practitioners design and facilitateinquiry-based processes that rely on sharedmeaning-making to result in transformational change. The transformationalchange unfolds due to the occurrence ofcore processes of disruptive emergence,generativity, and change in core narrative(s)underlying the dialogic processes (Bushe &Marshak, 2015).Practicing in the Grey Zone discussedthe implications of working from a Dialogic OD mindset, along the continuum ofdiagnostic to dialogic methodologies usedin the field. This sequel presents anothercase study in which working in the greyzone was successfully addressed to achievepositive outcomes. We (lead consultants,Melissa Crump and I), describe our navigating and balancing of practice in the greyzone via the Dialogic OD consulting stagesof initiating the inquiry, facilitating thejourney, and sustaining the transformation(Gilpin-Jackson, 2015).We start by reprinting an excerpt fromthe overview of the 2013 article, outliningthe evolution and maturity of OD methodologies, leading to the delineation of thegrey zone continuum. We then include asummary of the takeaways from the 2013article before introducing the current case.Overview, an Excerpt from the ODPArchives, V45(1)The field of Organization Development(OD) continues to buzz with the excitement of its third-generation methodologies. These methodologies represent ODpractices that are based on the premisethat an organization or system alreadyhas positive examples of what they wantmore of or what is needed for a desiredchange. The premise of third generationOD methodologies is, therefore, to searchout, highlight, or amplify what is alreadyworking in a system through genuineinquiry and conversation to understandvarying perspectives. Examples of thirdgeneration methodologies include Appreciative Inquiry and various whole systemengagement methodologies such as FutureSearch or Open Space conferences thatseek to unlock and amplify the generativepotential in organizations. Third generation methodologies are distinguished fromtheir first and second-generation precursors by the commitment to acknowledging and working with the subjectivity andmeaning-making of all involved. It is anapproach that upholds the social construction of human experience and embracesdialogue, inquiry and an emergent processPracticing in the Grey Area Between Dialogic and Diagnostic Organization Development: Lessons from Another Healthcare Case Study41
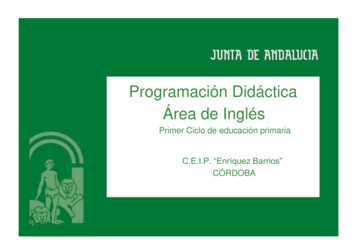
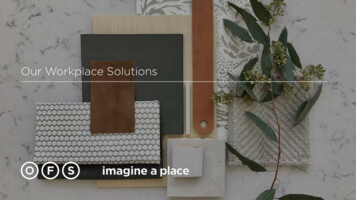
High42OD PRACTITIONER Vol. 50 No. 42018Dialogic ODreadinessand approach to change (Bouckenooghe,2010; Cameron, 2005).At the opposite end of the spectrum,first-generation OD methodologies assumethat change can be orchestrated by objectively identifying and quantifying problemswith a system or organization. Identifiedproblems are then corrected with prescribed solutions and recommendationsthat people in the system must adopt andimplement. Traditional action research isthe classic example of first-generation ODmethodologies, where objective data orvalid information is sought out and usedas the basis for diagnosing deficiencies ina system and recommending solutions.Second-generation methodologies are theset of approaches that bridge the first andthe third generations. They represent thedevelopmental methodologies that builton action research to action science andlearning organizations. The core tenetof second-generation methodologies isto work with observable data to identifydiscrepancies between desired and actualbehaviors and outcomes. It involves a commitment to reflection and public analysis ofattitudes, commitments and behaviors thatget in the way of desired outcomes, so thatsystem learning can occur (Raelin, 2006).OD practice has embraced its thirdgeneration methodologies. For example,there has been an explosion of wholesystem methodologies with features ofthird generation methodologies (Holman, Devane, & Cady, 2007). As with anymovement, however, new challenges andcomplexities tend to underscore emergentopportunities. Bushe and Marshak havenamed a bifurcation in the field, definedby the move to the practice of dialogic OD,which is characterized using third-generation OD methodologies. They explainthat the move to dialogic OD remainsunacknowledged in OD scholarship, as ODscholars continue to research and teachfrom the perspective of conventional, traditional diagnostic OD (Bushe, 2010; Bushe &Marshak, 2009)Diagnostic OD is traditional ODpractice in which a formal investigation isconducted so that objective data is collectedand analyzed to make a diagnosis andrecommendations for problem-solving—inDialogic ODBlended(Diagnostic/Dialogic OD)ModerateDiagnostic ODLowBlended(Diagnostic/Dialogic OD)ModerateHighc o m pl e x i t yReprinted from OD Practitioner 45(1)Figure 1. The Grey Zone Grid for Blended Diagnostic/Dialogic OD Practiceeffect, methodologies used in diagnosticpossibility that there is a grey area andOD are likely to be first-generation methodcontinuum in the space between diagologies. Second-generation methodologiesnostic OD and dialogic OD emerges.arguably represent diagnostic OD becauseWhile methodologies may be broadlyof their reliance on using valid data tocategorized as one form of OD or theuncover discrepancies between desired andother, it is the nature of the practiceactual behaviors and outcomes. However,and the intention behind the use ofsecond-generation methodologies couldthe methodology that would ultimatelyrepresent dialogic OD when identified gapsmake it diagnostic versus a dialogicare addressed using dialogic interventions.practice.For example, the practices associated with2. The art of mastering the grey zone indeveloping learning organizations oftenbetween diagnostic and dialogic ODrequire the use of valid or verifiable databecomes how well a practitioner canto engage in dialogue about discrepanciesmove along the continuum as approbetween espoused and actual behaviorpriate to the circumstance. The crucialin organizations (Argyris, 2005; Senge,element becomes practitioners’ ability1990).to understand the orientations, philosophical basis and intentions of the difLessons from the 2013 Case Studyferent forms of OD, such that they caneffectively move between and switchThe 2013 case focused on responding to thetheir own mental models to practicespecific question: can diagnostic and diaeffectively in either realm. This is notlogic OD co-exist and be used as complejust a question of acquiring diagnosticmentary forms of engagement in practice?or dialogic OD skills, but a matter of(Oswick, 2009). Through an analysis of amastery such that practitioners canmajor healthcare project that involved allsafely and effectively practice along thethe health authorities in the Lower Maincontinuum.land of British Columbia, Canada, the fol3. It is possible to blend and have diagnoslowing conclusions were presented:tic and dialogic methodologies co-exist.1. A dichotomous distinction between the 4. Two key questions must be answered togeneration of methodologies may notdetermine whether a situation requiresbe necessary, because: when a processa blended diagnostic/dialogic practicerather than a methodology-centeredin the grey zone. What is the level ofperspective is incorporated into ODcomplexity of the case? What is thepractice, the dichotomy betweenlevel of readiness of the organizationmethodologies diminishes and thefor dialogic practice? (See Figure 1.)
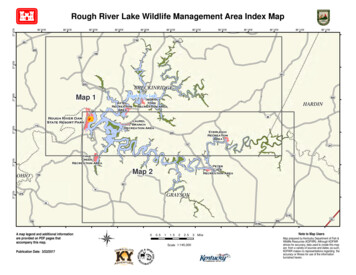
Table 1 was also presented to summarizethe grey zone continuum.A Recent CaseRoyal Columbian Hospital (RCH) is a 402bed tertiary care hospital in the Fraser Valley of British Columbia known for trauma,neurosurgery, cardiac, and neonatalcare (Royal Columbian Hospital, 2018).Currently, approximately 385 physicianswork at RCH comprised of approximately150 family physicians and 235 specialists(Royal Columbian Hospital ER, 2018).RCH participates in the National SurgicalQuality Improvement Program (NSQIP),a program created by surgeons for surgeons. This program is a risk adjusted,outcomes-based program to measureand improve the quality of surgical carethrough the generation of reports that helpto inform decisions (American College ofSurgeons, 2018).RCH has had a mature NSQIP program, existing for over ten years. However,within those years there had been nochange in the NSQIP data collected. TheTable 1. Practicing in the Grey Zone of the Diagnostic to Dialogic OD ContinuumConventional Diagnostic ODThe Grey ZoneConventional Dialogic ODType of ODMethodologies*First-generation ODmethodologies, e.g., actionresearch.First, second or third generationOD methodologies. Secondgeneration methodologies includefeatures of Diagnostic & DialogicOD.Third-generation ODmethodologies, e.g., AppreciativeInquiry.Goal of OD program,process, approach,or inquiry**Prescriptive diagnosis basedon a biological metaphor oforganizations. A focus on an idealidentified outcome.A blend of diagnosis and dialogueas needed at different stages ofthe change process. A focus oneffective change process to realizeidentified outcomes as well aspotential.Emergent self-organizing arounda shared vision created inconversation and interaction. Afocus on acting on opportunitiesand potential in the organizationsystem.Type of ODpractice***Methodology-centered wherediagnostic methods define the ODprogram.Holistic and adaptive practice thatis responsive to emergent needs.Methodology-centered wheredialogic methods define the ODprogram.Philosophicalorientation topracticeKnowledge can be objectivelydiscerned through research.Knowledge is co-created throughobjective data and emergentsubjective realities during theprocess.Knowledge is emergent andconstructed from real-time socialinteractions.Role of ODPractitionerExpert consultant.An expert, collaborator, projectmember, facilitator, trainer,mediator, and other roles assituations demand.Facilitator who recognizesthat their presence influencesknowledge creation.Source of ODInterventions****Interventions are recommended bythe OD practitioner.A blend of the practitioner’sexpert recommendations andself-organized solutions fromorganization members.Interventions are co-created by allinvolved and especially throughself-organizing.Practitionerinfluence onimplementationZero/limited influence wherepractitioners’ role is limited todiagnosis or maximum influencewhere contracted to implementrecommendations.High influence at early stageswhere the emphasis is ondiagnosis and zero to limitedinfluence as the focus shifts toDialogic OD.Zero/limited influence—interventions are implementedthrough self-organization ofparticipants.* OD methodologies are the set of methods, tools, techniques, or defined processes used to inquire and/or take actions to improve an organization’s effectiveness.**OD program is a full cycle of research and actions taken to improve organization effectiveness.***OD Practice is the professional exercise of organizational development using a variety of OD methodologies.****OD Interventions are the action(s) and methodologies within an OD program.Reprinted from OD Practitioner 45(1)Practicing in the Grey Area Between Dialogic and Diagnostic Organization Development: Lessons from Another Healthcare Case Study43
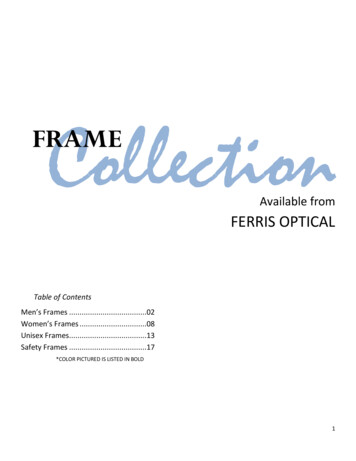
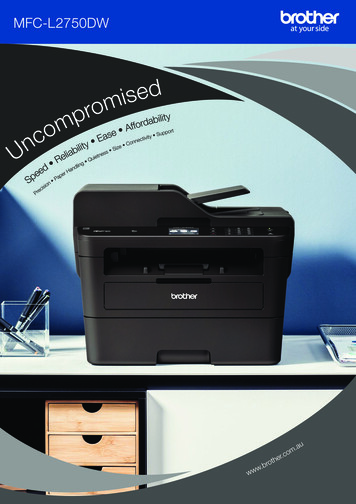
data showed that the majority of the surgical indicators were categorized as “needsimprovement,” which is highlighted in red.Organization Development wasapproached by the NSQIP surgical champion with these findings and the requestwas to partner with NSQIP to support theirgoal of getting RCH surgical staff involvedin quality improvement. However, priorto approaching Organization Development, RCH and NSQIP had a SurgicalQuality Improvement (QI) day plannedfor February 2016 to which they invitedindividuals from various surgical areas,as well as support staff. The agenda wastraditional and content heavy, as well ashaving many physician focused presentations. Despite this traditional approachalready being in place, Yabome GilpinJackson approved the request for supportand Melissa Crump as lead OrganizationDevelopment consultant facilitated oneportion of the day. The feedback receivedsurpassed all other presentations. It wasbased on this feedback that enabled theNSQIP surgical core team to decide thattheir traditional approach could benefitfrom a different approach to change.Initiating the InquiryAlthough Organization Development wasapproached to support the change thatwas desired from this group, the overallmindset was still one that was traditional.In other words, a diagnostic approach wasone that was familiar and used by thisgroup and expected by the NSQIP surgical core team to be utilized in this intervention. However, upon assessment andbecause the level of complexity was high,and the first conference had created somereadiness, a blended diagnostic/dialogicalmodel was required for any shifts to occur.More specifically a multilayer and facetedapproach was necessary for this intervention with RCH. Three levels of interventionwere focused on for the first phase of thechange intervention. Those layers includedthe senior leaders, the surgical core groupand the point of care staff. Point of carestaff was at this point expanded beyondphysicians to all point of care staff. Thisshift is paramount from the ideology that44OD PRACTITIONER Vol. 50 No. 42018Figure 2. Flipping from Typical Hierarchy to Positive Deviance HierarchyNSQIP was originally surgeon focused, toone that encapsulates all those individualsthat ‘touch’ the patient.Each intervention was specific toeach group, as well as carried out in a waythat achieved the desired outcomes, evenif the group was not aware of the intervention. The overarching methodologyused was the behavior science and socialchange approach called Positive Deviance(PD). The PD ideology is “based on theobservation that in every community thereare certain individuals or groups whoseuncommon behaviors and strategies enablethem to find better solutions to problemsthan their peers, while having access to thesame resources and facing similar or worstchallenges” (Positive Deviance Initiative,2017). PD relies on self-organizing in waysthat enables generativity and emergentsolutions for complex challenges. The selforganizing methodologies commonly usedwith PD are called Liberating Structures(LS) because they liberate all to participate.These methodologies meet all the criterion for dialogic OD methodologies. Thefocus in this phase was to introduce toolsand models found in LS to enable creativedestruction, as well as prepare the clientgroups by demystify some of the selflimiting behaviors and patterns that areinherent in the group.Positive Deviance was used at all threelevels of interventions. The first being withsenior leadership and surgical core group.A shift in their mindset and orientationto the work was essential to the successof staff. There was a need to move fromthe traditional hierarchical model to onethat flips it upside down and essentiallyinside out, where the role of leadership isto support the ideas that emerge from staffinstead of making decisions. Some may sayleaders need to make decisions and there isno disputing that, however when achievingsustainable long-term change to sociallyrooted behaviors, we must ask the controversial question: “How is that working forus?” There can be a balance where leaders provide the minimum specificationsneeded in a change, however successfulchange is one owned by those carrying itout. See Figure 2 adapted from Arvind Singhal (2017) presentation. As the literaturehas also confirmed, OD thrives to supportcomplex adaptive change when leadersmanage the process, but stake holdersdefine the changes required (Bushe, 2017).This new way of thinking was alsorequired for the staff to own this new wayof working towards quality improvement.While working with senior leadershipand the surgical core team, point of carestaff were invited twice a year to emersion workshops, and subsequently towhat became an annual conference. Theworkshops were emergent and co-createdby the Organization Development consultant and the NSQIP surgical core teamwith input from the staff. Each workshopbuilt upon the needs of the organization,site and staff, while enabling staff to learnabout Positive Deviance and utilize Liberating Structures to problem solve aroundtheir quality improvement challenges. Butmore importantly, it was a time for staff toconnect to the work and each other and seethings and each other in a different light.“Flipping” your thinking was the first PDideology taught. We were not only looking
at the possible verses the impossible, butwe are also looking at each other differentlyby creating connections and fanning similarities. When that mindset is encouragedstaff do not look at what is not available butwhat and who is available. This alone wasa huge achievement as many changes thatare necessary to improve quality improvement start with resources and changes thatare readily available and within their reachor control.As simple as the above may sound—it is, and it is not. Change first takes time,persistence and most of all commitment.focused on three segments: a) educationalcomponent, b) sharing the work by staffat RCH, and c) opportunity to continuethe work in the room. From a transformative learning perspective, the conferencebecame a space for the groups to exploreand share options for being and working together that the emerging solutionsrequired of them. They recognized theshared needs and desires and together theyplanned accordingly (Gilpin-Jackson, 2015).Our observation of the first year and ahalf was that individuals both on the coreNSQIP planning team and staff did notThere was a need to move from the traditional hierarchicalmodel to one that flips it upside down and essentially insideout, where the role of leadership is to support the ideas thatemerge from staff instead of making decisions. Some maysay leaders need to make decisions and there is no disputingthat, however when achieving sustainable long-term changeto socially rooted behaviors, we must ask the controversialquestion: “How is that working for us?” There can be a balancewhere leaders provide the minimum specifications needed ina change, however successful change is one owned by thosecarrying it out.The methodology requires actively working at all three levels consistently andsimultaneously, as each influences theother. It requires listening to the system toconstantly adapt and change as the systemchanges and evolves. Most of all it requirescreating the conditions for change thatdoes not feel “hard” or uncomfortable forthose involved in it. It requires individualleader coaching, strong facilitation designfor the workshops, and consistent collaboration throughout.Facilitating the JourneyThe annual conference became the coreavenue for facilitating the required transformations at scale, where all three groupscame together to generate new learningsand solutions across the spectrum ofNSQIP challenges. The annual conferencenecessarily understand the changes occurring. In leading the design of the changefrom a dialogic mindset, both structureddialogic processes such as PD/LS andprocess dialogic consulting, i.e. direct/formal and indirect/informal inquiry, andconversations were used by the OD teamto engage in ongoing meaning-making,planning, and change (Bushe & Marshak,2015). Every conversation was considered a change intervention. So, while theemergent nature was being tracked inthe mind of the consultant, it sometimesseemed unstructured and chaotic in theminds of the core group. The consultantthen took on the role of reducing the client’s anxiety, thereby moving them furtheralong in understanding their roles inchange and what they were experiencing(Marshak, 2016).The development of the content forworkshops seemed random and unstructured, however the emergence of thecontent was very structured within liberating structures. The workshop themselvesbuilt upon each other to be responsiveto the needs of the staff and the system.The core team, once socialized to the newmodel of change and mindset, were ableto co-facilitate. As processes and outcomesstarted making sense, participants startedto try to “figure out” the pattern of whatwas happening and how it was happening.For example, when individuals experiencedthe workshop they started to express thatthey too can build the workshop with Liberating Structures model and tools designedtogether as well as connection activitiesthat got people thinking about the content.This was positive from the perspective ofgetting people to this point of a developmental mindset. However, applied behavioral methodology isn’t about “figuring out”the secret ingredient but is about knowingthat in each recipe the secret ingredientneeds to change in response to the peopleinvolved and situation at hand. The secretingredient does not lie in the hands of one“expert” person or in one “perfect” process.This was demonstrated when the organization development consultant was awayand the group was tasked with organizinga workshop on their own. After trying tofigure out the “secret sauce” they defaultedback to the traditional way of doing thingswith highlights from what they had beenlearning. The experience of this workshopprovided the group with a different perspective that allowed them to recognize theintricacies and nuances that change workwith a dialogic OD mindset entails and theessential components that they needed toattend to. It also was the best demonstration to the team of the value of continuingto build their own capacity to work from adialogic mindset going forward.Sustaining the TransformationThe NSQIP data was being monitoredthroughout this intervention and if yourecall it had not changed in ten years. After1.5 years of NSQIP working in partnership with Organization Development 85Practicing in the Grey Area Between Dialogic and Diagnostic Organization Development: Lessons from Another Healthcare Case Study45
of the 100 indicators measured by NSQIPhad moved to either ‘exceptional’ or ‘asexpected’ metric (ACS Annual report,2016). The data sheet was no longerpainted red as it was prior to the intervention. More specifically this meant thatthere was an 85% reduction in morbidityacross all indicators and all programs. Thischange has never been seen before.This change in data allowed for seniorleaders to see the value in the work theNSQIP surgical core team was doing withOrganization Development. Those thatwere in denial that “this work” actuallyworked were no longer in denial. Staff alsowere able to see their impact on the NSQIPoutcomes that were measured and as aresult were actively asking for their data.Partnerships between support staff likeinfection control and prevention were cultivated and physician’s ears were perking upto the possibility of quality improvementat RCH.RCH had its third annual conferencethis year that looked and felt very differentto the first and even the second one. Theconference moved away from the NSQIPdriven premise. Although the data is stilla measure for change, the conferencewas all encompassing of quality improvement at a site level—the whole RCH wasinvited to the quality improvement day.Although there were two guest speakers,the highlight was the rapid-fire presentations where staff at RCH shared the qualityimprovement work they participated in.The core group that started out solelyNSQIP focused, has emerged into one thatis truly multidisciplinary with representation from across the hospital. They evennoted that since their focus has changedtheir name must also represent the change.They are now called the Quality Improvement League.As the hope of all Organization Development consultants is to work themselvesout of a job we can safely say we have donethat. The group is mature enough and hasthe basic foundations that has allowed usto step away and let it emerge and morphinto what it needs to be. However, we arealso aware that sustaining changes fromdialogic OD processes is often difficult ifsustaining structures to support ongoing46OD PRACTITIONER Vol. 50 No. 42018dialogue, planning and integration are notput in place (Roehrig, Schwendenwein, &Bushe, 2015). We are now transitioningthe work to a site-based consultant whowill loosely hold this group and guidethem as they develop fully. Consultationwill continue with the authors if/as neededto design ways to amplify and embed thechanges and fan the continued spread andscale of dialogic OD practices across thesite. The forums for continued follow-up,integration and tracking of outcomes havealready been instituted through the periodic workshops and annual conference.ConclusionI made the case recently that for ODpractitioners to grow what we want moreof we must focus on OD as the application of the behavioral and social sciencesto develop groups of people from wherethey are to where they want to go throughhigh-e ngagement and high-inquiry processes(Gilpin-Jackson, 2018). I argued that ODpractitioners might consider the following six conditions to amplify our influence. This case study met all the criteriaas follows:1. Claim unique value and space of supporting development in organizationsand practicing OD such that: “methodologies need to be used holarchically, where one flows into the otheras we nimbly switch between them asneeded, versus as an either/or.” Thiswas certainly what happened in thiscase as the lead consultant MelissaCrump switched between methodological orientations to meet clients wherethey were initially within a dialogicframework, then focusing on creating a dialogic mindset and learningtransformation as the next step, andsubsequently leading the group towhole-scale dialogic practices.2. Expand OD practice domain to workat full scope. One way I proposed thatwe do that was that we would betterengage the wisdom and power of thecrowd to galvanize leadership supportfor required systems changes. Thiswas the predominant orientation ofthis case study.3. Return to the values-base of our field.I asked: How might we be persistentin practicing these values in ways thatallow them to grow? Positive Devianceand Liberating Structures were listedas one of the exemplars of thrivingdialogic OD practices enabling this.4. Build and share portfolios of cases andresearch. I foreshadowed this case nowoutlined here as an example of a casestudy that had achieved desired resultsbased on the continuum of OD practice. Our client-sponsor has also beenprofiled elsewhere for his leadership inthis case as well as received an organizational award as a result (O’Conner,2017)5. Forge new partnerships: QualityImprovement was listed as a disciplinewhere practicing OD could thrivebecause of the complex adaptive challenges facing today’s healthcare.6. Engage in disruptive practice: As hasbeen described, the process engaged inwas certainly a disruption from the traditional diagnostic orientation the clientwas initial most comfortable with.ReferencesAmerican College of Surgeons. (2018).ACS National Surgical Quality Improvement Program. Retrieved from rican College of Surgeons (ACS)NSQIP. (2016). Royal ColumbianHospital Semiannual Report: SiteSummary.Argyris, C. (2005). Double-loop learningin organizations: A theory of actionperspective. In K. G. Smith & M. A.Hitt (Eds.), Great minds in management.Oxford, UK: University Press.Bouckenooghe, D. (2010). Positioningchange recipients’ attitudes towardchange in the organizational changeliterature. The Journal of Applied Behavioural Science, 46(4), 500–531. doi:DOI:10.1177/0021886310367944Bushe, G. R. (2010). Turning away fromdiagnosis. In W. J. Rothwell, J. M. Stavros, R. L. Sullivan, & A. Sullivan(Eds.), Practicing organization development: A guide for leading change.
San Francisco, CA: John Wiley andSons, Inc.Bushe, G. R. (2017). Where organization development thrives: Winner of the Val Hammond researchcompetition. Retrieved from ives/Bushe, G. R., & Marshak, R. J. (2009).Revisioning organization development: Diagnostic and dialogic premisesand patterns of practice. The Journalof Applied Behavioural Science, 45(3),378–383.Bushe, G. R., & Marshak, R. J. (2015).Introduction to the Practice of DialogicOD. In G. R. Bushe & R. J. Marshak(Eds.), Dialogic organization development: The theory and practice of transformational change (pp. 33–56). Oakland:CA: Berrett-Koehler.Bushe, G. R., & Marshak, R. J. (Eds.).(2015). Dialogic organization development: The theory and practice of transformational change. Oakland, CA:Berrett-Koehler.Cameron, K. (2005). Organization effectiveness: Its demise and re-emergencethrough positive organization scholarship. In K. G. Smith & M. A. Hitt(Eds.), Great minds in management(pp. 304–330). Oxford, UK: UniversityPress.Gilpin-Jackson, Y. (2015). Transformativelearning during dialogic OD. In
Practicing in the Grey Area Between Dialogic and Diagnostic Organization Development Lessons from Another Healthcare Case Study By Yabome Gilpin-Jackson with Melissa Crump In 2013, the Practicing in the Grey Zone article was published outlining how