Transcription
EIGHTH EDITIONCLINICAL BIOCHEMISTRY &METABOLIC MEDICINE
This page intentionally left blank
EIGHTH EDITIONCLINICAL BIOCHEMISTRY& METABOLIC MEDICINEProfessor Martin Andrew Crook BSc MB BS MA PhD FRCPath FRCPI FRCPConsultant in Chemical Pathology and Metabolic MedicineGuy’s, St Thomas’ and University Hospital Lewisham, London, UK,and Visiting Professor, School of Science, University of Greenwich, UK
First published in Great Britain in 1971 by Lloyd-Luke (Medical Books) LtdSecond edition 1975Third edition 1979Fourth edition 1984Fifth edition published in 1988 by Edward Arnold (Publishers) LtdSixth edition published in 1994Seventh edition published in 2006 by Hodder ArnoldThis eighth edition published in 2012 by Hodder Arnold, an imprint of Hodder Education, Hodder and Stoughton Ltd, a division of HachetteUK,338 Euston Road, London, NW1 3BHhttp://www.hodderarnold.com 2012 Hodder & Stoughton LtdAll rights reserved. Apart from any use permitted under UK copyright law, this publication may only be reproduced, stored or transmitted in anyform or by any means with prior permission in writing of the publishers or in the case of reprographic production in accordance with the terms oflicences issued by the Copyright Licensing Agency. In the United Kingdom such licences are issued by the Copyright Licensing Agency: SaffronHouse, 6–10 Kirby Street, London EC1N 8TS.Whilst the advice and information in this book are believed to be true and accurate at the date of going to press, neither the author nor thepublisher can accept any legal responsibility or liability for any errors or omissions that may be made. In particular (but without limiting thegenerality of the preceding disclaimer), every effort has been made to check drug dosages; however, it is still possible that errors have beenmissed. Furthermore, dosage schedules are constantly being revised and new side effects recognized. For these reasons the reader is stronglyurged to consult the drug companies’ printed instructions, and their websites, before administering any of the drugs recommended in this book.British Library Cataloguing in Publication DataA catalogue record for this book is available from the British LibraryLibrary of Congress Cataloging-in-Publication DataA catalog record for this book is available from the Library of CongressISBN-13ISBN-13 [ISE]978-1-4441-4414-7978-1-4441-4416-11 2 3 4 5 6 7 8 9 10In order that we can ensure that students continue to benefit fromthe availability of our special editions, if you have purchased yourcopy in an un-authorized country, please email exportenquiries@hodder.co.uk letting us know where, when and from whichorganization or individual you made the purchase.Commissioning Editor:Project Editor:Production Controller:Cover Designer:Indexer:Joanna KosterJenny WrightFrancesca WardellAmina DudhiaLaurence ErringtonCover: PASIEKA/SCIENCE PHOTO LIBRARYTypeset in 11/13 pt Minion by Phoenix Photosetting, Chatham, KentPrinted and bound in IndiaWhat do you think about this book? Or any other Hodder Arnold title?Please send your comments to www.hoddereducation.com
ContentsPrefaceviiList of abbreviationsviii1 Requesting laboratory tests and interpreting the results12 Water and sodium63 The kidneys364 Acid–base disturbances595 Potassium836 Calcium, phosphate and magnesium957 The hypothalamus and pituitary gland1168 The adrenal cortex1299 The reproductive system14610 Pregnancy and infertility15711 Thyroid function16412 Carbohydrate metabolism17613 Plasma lipids and lipoproteins20014 Nutrition21615 Vitamins, trace elements and metals22416 The gastrointestinal tract23517 Liver disorders and gallstones25218 Plasma enzymes in diagnosis (clinical enzymology)27019 Proteins in plasma and urine28220 Purine and urate metabolism30321 Disorders of haem metabolism: iron and the porphyrias31022 Cardiovascular disease325
viContents23 Cerebrospinal, pleural and ascitic fluids33224 Metabolic effects of tumours33825 Therapeutic drug monitoring and poisoning34726 Clinical biochemistry at the extremes of age35827 Inborn errors of metabolism37128 Genetics and deoxyribonucleic acid-based technology in clinical biochemistry38429 Patient sample collection and use of the laboratory39130 Point-of-care testing397Appendix 1: Units in clinical chemistry401Index403COMPANION WEBSITEThis book has a companion website available at:www.hodderplus.com/clinicalbiochemistryThe website contains downloadable images from the book as well as self assessment questions.To access these resources please register on the website using the following access details:Serial number: 145jw76mc8fwOnce you have registered you will not need the serial number but can log in using the username and passwordthat you will create during your registration.
PrefaceWere it not for the textbook Clinical Chemistry in Diagnosis and Treatment by Joan Zilva and Peter Pannall, I wouldnot be a chemical pathologist. As a medical student, I was so struck by its clarity, depth and clinical relevance thatI decided that theirs was the medical field I wished to work in.Over the years, the field of clinical biochemistry has changed radically. Confusingly, there is no consensuson the name for this field of medicine, which is known variously as clinical chemistry, chemical pathology orclinical biochemistry, to name but a few. Additionally, the field now overlaps with that of metabolic medicine, aclinical specialty involved with the management and treatment of patients with disorders of metabolism. Clinicalbiochemistry laboratories have become further automated, molecular biology technologies have entered thediagnostic arena, and chemical pathologists have become more clinically orientated towards running out-patientclinics for a variety of biochemical disturbances. This book aims to address these new changes. Indeed, it is difficultto imagine a branch of medicine that does not at some time require clinical biochemistry tests, which may not betoo surprising, given the fact that every body cell is composed of chemicals!Unfortunately, there have been some difficulties in recent times, with a relative shortage of graduates enteringthe specialty, which has not been helped by some people’s attitude that clinical biochemistry is merely a laboratoryfactory churning out results that anyone can interpret. There are also concerns that medical student clinicalbiochemistry teaching may become ‘diluted’ as part of an expanding curriculum. It is hoped that this book willexcite a new generation to enter this fascinating and essential field, as well as benefit patients as their doctors learnmore about their biochemical and metabolic problems.I am most grateful to Dr Sethsiri Wijeratne, Dr Alam Garrib (particularly for molecular biology expertise) andDr Paul Eldridge for constructive criticism of the text. I am also grateful to Professor Philip Mayne for his earliercontributions and the anonymous medical student reviewer(s) who commented on the text. The book has alsogreatly benefited from the wise, helpful and experienced input of Dr Andrew Day – many thanks. Although everyeffort has been made to avoid inaccuracies and errors, it is almost inevitable that some may still be present, andfeedback from readers is therefore welcome.Martin CrookLondon, 2012Disclaimer The publishers and author accept no responsibility for errors in the text or misuse of the materialpresented. Drugs and their doses should be checked with a pharmacy, and the investigation protocols with anappropriate clinical laboratory. Dynamic test protocols should be checked with an accredited clinical investigationunit and may require different instructions in the elderly, children and the obese.
List of abbreviationsABC1ATPaseATPadenosine triphosphate-binding cassetteprotein 1angiotensin-converting enzymeacid phosphatasealbumin to creatinine ratioadrenocorticotrophic hormone(corticotrophin)antidiuretic hormone (argininevasopressin)accident and emergency (department)a-fetoproteinacquired immunodeficiency syndromeautoimmune insulin syndromeacute kidney injury5-aminolaevulinic acidalkaline phosphatasealanine aminotransferase (also knownas glutamate pyruvate aminotransferase,GPT)arm muscle circumferenceantinuclear antibodyantineutrophil cytoplasmic antibodyatrial natriuretic peptidealdosterone-producing adenomaapolipoproteinadenine phosphoribosyl transferaseamine precursor uptake anddecarboxylationangiotensin II receptor antagonistangiotensin II receptor blockeramplification refractory mutationsystemaspartate aminotransferase (alsoknown as glutamate oxaloacetateaminotransferase, GOT)adenosine triphosphataseadenosine triphosphateBJPBMDBMIBMRBNPBPHBence Jones proteinbone mineral densitybody mass indexbasal metabolic ratebrain natriuretic peptidebenign prostatic CTCVCys ENAENTERCPESRcarbohydrate antigencalcium excreted per litre of glomerularfiltratecongenital adrenal hyperplasiacyclic adenosine monophosphatecalcium-sensing receptorcomputerized axial tomographycortisol-binding globulin (transcortin)carbonate dehydratase (carbonicanhydrase)carcinoembryonic antigencholesterol ester transfer proteincreatine kinasechronic kidney diseaseC-type natriuretic peptidecentral nervous systemcoenzyme Achronic obstructive pulmonary diseasecorticotrophin-releasing hormoneC-reactive proteincerebrospinal fluidcomputerized tomographycoefficient of variationcystatin C2,3-diphosphoglycerate1-desamino-8-D-arginine vasopressin(desmopressin ne sulphatedi-iodotyrosinedeoxyribonucleic aciddipeptidyl peptidase-4deep vein thrombosisextracellular fluidelectrocardiogramethylenediamine tetra-acetic acidestimated glomerular filtration rateextractable nuclear antigenear, nose and throat (department)endoscopic retrogradecholangiopancreatographyerythrocyte sedimentation rate
List of abbreviationsEUSendoscopic avine adenine dinucleotidefamilial combined hyperlipidaemiafamilial dysalbuminaemichyperthyroxinaemiafractional excretion of sodiumfractional excretion of phosphatefamilial hypercholesterolaemiaflavine mononucleotidefollicle-stimulating hormonefree T4free T3GADGDMGFRGGTGHGHRHGIPGLP-1GnRHG6PG6PDGRAglutamic decarboxylasegestational diabetes mellitusglomerular filtration rateg-glutamyl transferasegrowth hormonegrowth hormone-releasing hormonegastric inhibitory peptideglucagon-like peptide 1gonadotrophin-releasing hormoneglucose-6-phosphateglucose-6-phosphate dehydrogenaseglucocorticoid remediable atitis A virushaemoglobinglycated haemoglobinviral surface antigenhydroxybutyrate dehydrogenasehepatitis B virushuman chorionic gonadotrophinhepatitis C virushigh-density lipoproteinheparin extracorporeal low-densitylipoprotein precipitationHFEhuman haemochromatosis proteinHGPRThypoxanthine–guanine phosphoribosyltransferase5-HIAA5-hydroxyindole acetic acidHIVhuman immunodeficiency virusHLAhuman leucocyte antigenHMG-CoA 3-hydroxy-3-methyl glutaryl coenzyme AHMMA4-hydroxy-3-methoxymandelic acidHNFhepatocyte nuclear factorHONKhyperosmolal non-ketotic (coma)HRThormone replacement therapyhs-CRPhigh-sensitivity C-reactive protein5-HT5-HTPHVAhydroxytryptamine (serotonin)hydroxytryptophanhomovanillic acidIAHIDLIDMSIEMIFGIFNIgIGFIGTILINRidiopathic adrenal hyperplasiaintermediate-density lipoproteinisotope dilution mass spectrometryinborn errors of metabolismimpaired fasting glucoseinterferonimmunoglobulininsulin-like growth factorimpaired glucose toleranceinterleukininternational normalized ratioLADALCATLDHLDLLHLRlatent autoimmune diabetes of adultslecithin–cholesterol acyltransferaselactate dehydrogenaselow-density lipoproteinluteinizing hormonelikelihood ratioMCADDmedium-chain acyl coenzyme Adehydrogenase deficiencymean corpuscular haemoglobinmean corpuscular volumemodification of diet in renal disease(formula)monoethylglycinexylididemultiple endocrine neoplasiamonoclonal gammopathy ofundetermined nematurity-onset diabetes of the youngmucopolysaccharidosismagnetic resonancecholangiopancreatographymagnetic resonance imagingmessenger ribonucleic acidmelanocyte-stimulating hormonemitochondrial DNAmethylenetetrahydrofolate ImRNAMSHmtDNAMTHFRNADNADPNAFLDNAGnicotinamide adenine dinucleotidenicotinamide adenine dinucleotidephosphatenon-alcoholic fatty liver diseaseN-acetyl-b-D-glucosaminidaseix
xList of alcoholic steatotic hepatitisnon-esterified fatty acidneutrophil gelatinase-associated lipocalinNational Health Servicenon-islet cell tumour hypoglycaemianatriuretic peptidenon-steroidal anti-inflammatory drugnon-ST segment elevation myocardialinfarctionOGTTOTCoral glucose tolerance testornithine ARPRPPPSAPTHPTHRPpara-amino benzoic acidporphobilinogenpolymerase chain reactionpolyethylene glycolprimary hyperaldosteronismprotease inhibitorproteins induced by vitamin K absencephenylketonuriaprognostic nutritional indexpoint-of-care testingperoxisome proliferator-activated receptorphosphoribosyl pyrophosphateprostate-specific antigenparathyroid hormoneparathyroid hormone-related proteinRBPRDSRFLPretinol-binding proteinrespiratory distress syndromerestriction fragment lengthpolymorphismribonucleic acidreceiver operating characteristic (curve)renal replacement therapyRNAROCRRTSCIDSDSHBGSIADHSLESTEMIsevere combined immunodeficiencystandard deviationsex-hormone-binding globulinsyndrome of inappropriate antidiuretichormone secretionsystemic lupus erythematosusST-segment elevation inding globulintotal body watertricarboxylic acidtransferrin receptortotal iron-binding capacitytumour necrosis factorthyroid peroxidasethiopurine methyltransferasethyrotrophin-releasing hormonethyroid-stimulating hormonethyroid-stimulating immunoglobulintranstubular potassium gradientUGTUIBCURLuridine glucuronyl transferaseunsaturated iron-binding capacityupper reference limitVIPVLCFAVLDLVDBPVDRvasoactive intestinal polypeptidevery long-chain fatty acidvery low-density lipoproteinvitamin D-binding proteinvitamin D receptorWHOWorld Health Organization
1Requesting laboratory tests andinterpreting the resultsRequesting laboratory testsHow often should I investigate the patient?When is a laboratory investigation ‘urgent’?111REQUESTING LABORATORY TESTSThere are many laboratory tests available to the clinician.Correctly used, these may provide useful information,but, if used inappropriately, they are at best useless andat worst misleading and dangerous.In general, laboratory investigations are used: to help diagnosis or, when indicated, to screen formetabolic disease,to monitor treatment or detect complications,occasionally for medicolegal reasons or, with duepermission from the patient, for research.Overinvestigation of the patient may be harmful,causing unnecessary discomfort or inconvenience,delaying treatment or using resources that might bemore usefully spent on other aspects of patient care.Before requesting an investigation, clinicians shouldconsider whether its result would influence their clinicalmanagement of the patient.Close liaison with laboratory staff is essential; theymay be able to help determine the best and quickestprocedure for investigation, interpret results anddiscover reasons for anomalous findings.Interpreting resultsIs the abnormality of diagnostic value?Diagnostic performance234rapidly in patients given large doses of diuretics andthese alterations may indicate the need to instigate orchange treatment (see Chapter 5).Laboratory investigations are very rarely neededmore than once daily, except in some patients receivingintensive therapy. If they are, only those that areessential should be repeated.WHEN IS A LABORATORYINVESTIGATION ‘URGENT’?The main reason for asking for an investigation to beperformed ‘urgently’ is that an early answer will alterthe patient’s clinical management. This is rarely thecase and laboratory staff should be consulted and thesample ‘flagged’ as clearly urgent if the test is requiredimmediately. Laboratories often use large analyserscapable of assaying hundreds of samples per day(Fig. 1.1). Point-of-care testing can shorten resultturnaround time and is discussed in Chapter 30.HOW OFTEN SHOULD I INVESTIGATETHE PATIENT?This depends on the following: How quickly numerically significant changes arelikely to occur: for example, concentrations of themain plasma protein fractions are unlikely to changesignificantly in less than a week (see Chapter 19),similarly for plasma thyroid-stimulating hormone(TSH; see Chapter 11). See also Chapter 3.Whether a change, even if numerically significant, willalter treatment: for example, plasma transaminaseactivities may alter within 24 h in the course of acutehepatitis, but, once the diagnosis has been made, thisis unlikely to affect treatment (see Chapter 17). Bycontrast, plasma potassium concentrations may alterFigure 1.1 A laboratory analyser used to assayhundreds of blood samples in a day. Reproduced withkind permission of Radiometer Limited.
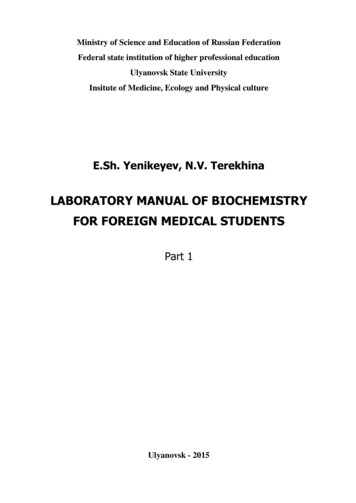
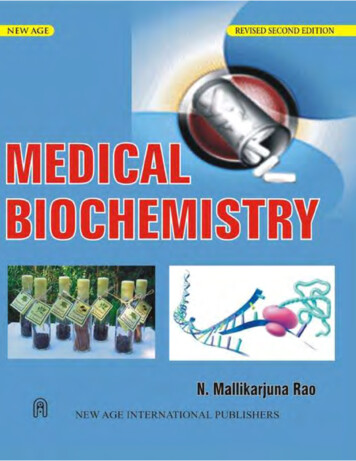
Requesting laboratory tests and interpreting the resultsLaboratories usually have ‘panic limits’, whenhighly abnormal test results indicate a potentially lifethreatening condition that necessitates contacting therelevant medical staff immediately. To do so, laboratorystaff must have accurate information about the locationof the patient and the person to notify.INTERPRETING RESULTSWhen interpreting laboratory results, the clinicianshould ask the following questions: Is the result the correct one for the patient?Does the result fit with the clinical findings?Remember to treat the patient and not the‘laboratory numbers’.If it is the first time the test has been performedon this patient, is the result normal when theappropriate reference range is taken into account?If the result is abnormal, is the abnormality ofdiagnostic significance or is it a non-specificfinding?If it is one of a series of results, has there beena change and, if so, is this change clinicallysignificant?Abnormal results, particularly if unexpected andindicating the need for clinical intervention, are bestrepeated.CASE 1A blood sample from a 4-year-old boy withabdominal pain was sent to the laboratory from anaccident and emergency department. Some of theresults were as follows:Test reference rangesBy convention, a reference (‘normal’) range (or interval)usually includes 95 per cent of the test results obtainedfrom a healthy and sometimes age- and sex-definedpopulation. For the majority of tests, the individual’sresults for any constituent are distributed aroundthis mean in a ‘normal’ (Gaussian) distribution, the95 per cent limits being about two standard deviationsfrom the mean. For other tests, the reference distributionmay be skewed, either to the right or to the left, aroundthe population median. Remember that 2.5 per cent ofthe results at either end will be outside the referencerange; such results are not necessarily abnormal for thatindividual. All that can be said with certainty is thatthe probability that a result is abnormal increases thefurther it is from the mean or median until, eventually,this probability approaches 100 per cent. Furthermore,a normal result does not necessarily exclude the diseasethat is being sought; a test result within the populationreference range may be abnormal for that individual.Very few biochemical tests clearly separate a ‘normal’population from an ‘abnormal’ population. Formost there is a range of values in which ‘normal’ and‘abnormal’ overlap (Fig. 1.2), the extent of the overlapdiffering for individual tests. There is a 5 per cent chancethat one result will fall outside the reference range, andwith 20 tests a 64 per cent chance, i.e. the more testsdone, the more likely it is that one will be statisticallyabnormal.No result of any investigation should be interpretedwithout consulting the reference range issued by the160PlasmaBilirubin 14 µmol/L ( 20)Alanine transaminase 14 U/L ( 42)Alkaline phosphatase 326 U/L ( 250)Albumin 40 g/L (35–45)g-Glutamyl transferase 14 U/L ( 55)Albumin-adjusted calcium 2.34 mmol/L (2.15–2.55)DISCUSSIONThe patient’s age was not given on the request formand the laboratory computer system ‘automatically’used the reference ranges for adults. The plasmaalkaline phosphatase activity is raised if comparedwith the adult reference range, but in fact is within‘normal limits’ for a child of 4 years (60–425). Seealso Chapters 6 and 18.140120Number of subjects210080604020‘Normal’subjectsOverlap between‘normal’ and ‘ill’‘Ill subjects’1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18Arbitrary unitsFigure 1.2 Theoretical distribution of values for‘normal’ and ‘abnormal’ subjects, showing overlap atthe upper end of the reference range.
Is the abnormality of diagnostic value?laboratory carrying out the assay. Some analytes haverisk limits for treatment, such as plasma glucose (seeChapter 12), or target or therapeutic limits, such asplasma cholesterol (see Chapter 13).Various non-pathological factors may affect theresults of investigations, the following being some ofthe more important ones.Between-individual differencesPhysiological factors such as the following affect theinterpretation of results.Age-related differencesThese include, for example, bilirubin in the neonate(see Chapter 26) and plasma alkaline phosphataseactivity, which is higher in children and the elderly (seeChapter 18).Sex-related differencesExamples of sex-related differences include plasmaurate, which is higher in males, and high-densitylipoprotein cholesterol, which is higher in premenopausal women than in men (see Chapters 13 and20). Obviously, sex hormone concentrations also differbetween the sexes (see Chapter 9).Ethnic differencesThese may occur because of either racial or environmentalfactors, for example plasma creatine kinase may be higherin black than in white people (see Chapter 18).Within-individual variationsThere are biological variations of both plasmaconcentrations and urinary excretion rates of manyconstituents, and test results may be incorrectlyinterpreted if this is not taken into consideration.Biological variations may be regular or random.RegularSuch changes occur throughout the 24-h period(circadian or diurnal rhythms, like those of bodytemperature) or throughout the month. The daily(circadian) variation of plasma cortisol is of diagnosticvalue, but, superimposed on this regular variation,‘stress’ will cause an acute rise (see Chapter 8). Plasmairon concentrations may fall by 50 per cent betweenmorning and evening (see Chapter 21). To eliminatethe unwanted effect of circadian variations, bloodshould ideally always be taken at the same time of day,preferably in the early morning and, if indicated, withthe patient fasting. This is not usually possible, andthese variations should be taken into account whenserial results are interpreted.Some constituents vary monthly, especially inwomen during the menstrual cycle. These variationscan be very marked, as in the results of sex hormoneassays, for example plasma oestradiol, which can only beinterpreted if the stage of the menstrual cycle is known;plasma iron may fall to very low concentrations justbefore the onset of menstruation. Other constituentsmay also vary seasonally. For example, vitamin Dconcentrations may be highest in the summer months.Some of these changes, such as the relation betweenplasma glucose and meals, have obvious causes.RandomDay-to-day variations, for example in plasma ironconcentrations, can be very large and may swamp regularcycles. The causes of these are not clear, but they should beallowed for when serial results are interpreted – for examplethe effect of ‘stress’ on plasma cortisol concentrations.The time of meals affects plasma glucoseconcentrations, and therefore correct interpretationis often only possible if the blood is taken when thepatient is fasting or at a set time after a standard dose ofglucose (see Chapter 12).Methodological differences betweenlaboratoriesIt has been pointed out that, even if the same methodis used throughout a particular laboratory, it isdifficult to define normality clearly. Interpretationmay sometimes be even more difficult if the resultsobtained in different laboratories, using differentanalytical methods, are compared. Agreement betweenlaboratories is close for many constituents partly dueto improved standardization procedures and becausemany laboratories belong to external quality controlschemes. However, for others, such as plasma enzymes,different methods may give different results. For varioustechnical reasons, the results would still vary unless thesubstrate, pH and all the other variables were the same.IS THE ABNORMALITY OF DIAGNOSTICVALUE?Relation between plasma and cellularconcentrationsIntracellular constituents are not easily sampled,and plasma concentrations do not always reflect thesituation in the cells; this is particularly true for those3
4Requesting laboratory tests and interpreting the resultsconstituents, such as potassium and phosphate, thatare at much higher concentrations intracellularlythan extracellularly. A normal, or even high, plasmapotassium concentration may be associated withcellular depletion if equilibrium across cell membranesis abnormal, such as in diabetic ketoacidosis. Analyteconcentrations may differ between plasma (theaqueous phase of anticoagulated blood) and serum (theaqueous phase of clotted blood). The concentrationof potassium, for example, is higher in serum than inplasma samples because of leakage from cells duringclotting, and the total protein concentration is lower inserum than in plasma because the protein fibrinogen isremoved during the clotting process.Non-specific abnormalitiesThe concentrations of all protein fractions, includingimmunoglobulins, and of protein-bound substancesmay fall by as much as 15 per cent after as little as 30 minrecumbency, owing to fluid redistribution in the body.This may account, at least in part, for the low plasmaalbumin concentrations found in even quite minorillnesses. In-patients often have blood taken early in themorning, while recumbent, and plasma concentrationsof protein and protein-bound substances tend to belower than in out-patients (see Chapter 19).CASE 2A 54-year-old Nigerian man was seen in an accidentand emergency department because of chest pain.His electrocardiogram (ECG) was normal. Thefollowing results were returned from the laboratory,6 h after his chest pain started:PlasmaCreatine kinase 498 U/L ( 250)Troponin T 10 pg/L ( 20)DISCUSSIONThe raised plasma creatine kinase activity suggested anacute myocardial infarction (see also Chapters 18 and22). The patient was, however, subsequently found notto have had a myocardial infarction (confirmed by anormal troponin T result) and the raised plasma creatinekinase activity was thought to be due to his racial origin.(The reference range of 250 U/L was based on thatof the predominantly white UK population; normalplasma creatine kinase activity may be two to threetimes higher in black than in white people.)DIAGNOSTIC PERFORMANCEBefore one can interpret day-to-day changes in resultsand decide whether the patient’s biochemical statehas altered, one must know the degree of variationto be expected in the results derived from a normalpopulation. We have already discussed intraindividual(same person) analyte variation. However, there is alsounavoidable analytical variation.CASE 3One hundred patients with chest pain were screenedwith a new biochemical test that showed 80 to bepositive for chest pain. What is the test’s sensitivity?Answer: 80/100 100% 80%The same test was used on 100 patients without chestpain, and 95 had a negative screening result. What isthe test’s specificity?Answer: 95/100 100% 95%DISCUSSIONSensitivity is true-positive rate per total affected.Specificity is true-negative rate per total unaffected.Reproducibility of laboratory estimationsMost laboratory estimations should give results thatare reproducible to well within 5 per cent; some, suchas those for sodium and calcium, should be even moreprecise, but the variability of some hormone assays,for example, may be greater. Small changes in resultsproduced by relatively imprecise methods are not likelyto be clinically significant.Imprecision is the term used to describe the randomchanges that reduce the agreement between replicateassay measurements. This can be considered in terms ofthe within-assay precision, which is the assay variabilitywhen the same material is assayed repeatedly withinthe same assay batch, or day-to-day precision, whichis the variability when the same material is assayed ondifferent days.The assay coefficient of variation (CV) is usedto express imprecision and can be calculated by thefollowing equation:CV% standard deviation of the assay 100%mean of the assay results(1.1)This should be as small as possible for each assay, andcan be expressed as the intra-assay CV when describingthe imprecision within a single run or batch.
Diagnostic performanceTest sensitivity and specificityABCSensitivityDiagnostic sensitivity is a measure of the frequency of atest being positive when a particular disease is present,that is, the percentage of true-positive (TP) results.Diagnostic specificity is a measure of the frequency ofa test being negative when a certain disease is absent,that is, the percentage of true-negative (TN) results.Ideally, a test would have 100 per cent specificity and100 per cent sensitivity.Th
on the name for this fi eld of medicine, which is known variously as clinical chemistry, chemical pathology or clinical biochemistry, to name but a few. Additionally,