Transcription
Guidelines and Standards for Performance ofa Pediatric Echocardiogram: A Report fromthe Task Force of the Pediatric Council of theAmerican Society of EchocardiographyWyman W. Lai, MD, MPH, FASE, Tal Geva, MD, FASE, Girish S. Shirali, MD,Peter C. Frommelt, MD, Richard A. Humes, MD, FASE, Michael M. Brook, MD,Ricardo H. Pignatelli, MD, and Jack Rychik, MD, Writing Committee, New York, New York;Boston, Massachusetts; Charleston, South Carolina; Milwaukee, Wisconsin; Detroit, Michigan; San Francisco, California;Houston, Texas; and Philadelphia, PennsylvaniaEchocardiography has become the primary imag-ing tool in the diagnosis and assessment of congenital and acquired heart disease in infants, children,and adolescents. Transthoracic echocardiography(TTE) is an ideal tool for cardiac assessment, as it isnoninvasive, portable, and efficacious in providingdetailed anatomic, hemodynamic, and physiologicinformation about the pediatric heart.Recommendations for standards in the performanceof a routine 2-dimensional (2D) echocardiogram,1 fetalechocardiogram,2 pediatric transesophageal echocardiogram,3 intraoperative transesophageal echocardiogram,4 and stress echocardiogram5 exist, as doguidelines for appropriate training in various echocardiographic disciplines.6-12 As part of the accreditation process for echocardiography laboratories,the Intersocietal Commission for the Accreditationof Echocardiography Laboratories has establishedbasic performance standards for pediatric TTE,13 butno other standards document exists for the performance of a pediatric TTE.The pediatric echocardiogram is a unique examination with features that distinguish it from otherechocardiograms. There is a wide spectrum ofanomalies encountered in patients with congenitalheart disease. Certain views are of added importanceFrom the Mount Sinai Medical Center, New York (W.W.L.);Children’s Hospital, Boston (T.G.); Medical University of SouthCarolina, Charleston (G.S.S.); Children’s Hospital of Wisconsin,Milwaukee (P.C.F.); Children’s Hospital of Michigan, Detroit(R.A.H.); University of San Francisco (M.M.B.); Texas Children’sHospital, Houston (R.H.P.); and Children’s Hospital of Philadelphia (J.R.).Reprint requests: Wyman W. Lai, MD, MPH, FASE, Division ofPediatric Cardiology, Box 1201, Mount Sinai Medical Center, OneGustave L. Levy Place, New York, NY 10029 (E-mail: wyman.lai@mssm.edu).J Am Soc Echocardiogr 2006;19:1413-1430.0894-7317/ 32.00Copyright 2006 by the American Society of Echocardiography.doi:10.1016/j.echo.2006.09.001for pediatric examinations: the subxiphoid (or subcostal), suprasternal notch, and right parasternalviews. The acquisition and proper display of imagesfrom these views are critical aspects of the pediatricTTE. In addition, special techniques are required forimaging uncooperative infants and young children,including sedation and distraction tools that willallow performance of a complete examination.The purposes of this document are to: (1) describe indications for pediatric TTE; (2) define optimal instrumentation and laboratory setup for pediatric echocardiographic examinations; (3) provide aframework of necessary knowledge and training forsonographers and physicians; (4) establish an examination protocol that defines necessary echocardiographic windows and views; (5) establish a baseline list of recommended measurements to beperformed in a complete pediatric echocardiogram; and (6) discuss reporting requirements andformatting of pediatric reports.INDICATIONSKnowledge of indications for an echocardiogram isimportant to obtain the information required for thediagnosis and proper treatment of the pediatricpatient. The general categories of indications areprovided below, with emphasis placed on the indications for a pediatric echocardiogram versus astandard adult study. For detailed age-specific lists ofindications, the reader is referred to prior publishedguidelines.14Children with suggested or known heart diseasefrequently require serial studies to evaluate theevolution or progression of heart disease. Serialstudies may be indicated at routine intervals formonitoring of valve function, growth of cardiovascular structures, ventricular function, and potentialsequelae of medical or surgical intervention.15-181413
1414 Lai et alCongenital Heart Disease: History, Symptoms,and SignsIndications for the performance of a pediatric echocardiogram span a wide range of symptoms andsigns, including cyanosis, failure to thrive, exerciseinduced chest pain or syncope, respiratory distress,murmurs, congestive heart failure, abnormal arterialpulses, or cardiomegaly. These may suggest categories of structural congenital heart disease includingintracardiac left-to-right or right-to-left shunts, obstructive lesions, regurgitant lesions, transpositionphysiology, abnormal systemic or pulmonary venousconnections, conotruncal anomalies, coronary artery anomalies, functionally univentricular hearts,and other complex lesions, including abnormal laterality (heterotaxy/isomerism). Certain syndromes,family history of inherited heart disease, andextracardiac abnormalities that are known to beassociated with congenital heart disease constitute clinical scenarios for which echocardiography is indicated even in the absence of specificcardiac symptoms and signs. Abnormalities onother tests such as fetal echocardiography, chestradiograph, electrocardiogram, and chromosomalanalysis constitute another group in which thesuggestion of congenital heart disease is addressedspecifically by echocardiography.Acquired Heart Diseases and NoncardiacDiseasesAn echocardiogram is indicated for the evaluation ofacquired heart diseases in children, including Kawasaki disease, infective endocarditis, all forms ofcardiomyopathies, rheumatic fever and carditis, systemic lupus erythematosus, myocarditis, pericarditis, HIV infection, and exposure to cardiotoxicdrugs. Pediatric echocardiography is indicated in theassessment of potential cardiac or cardiopulmonarytransplant donors and transplant recipients. Recently, echocardiography has been recommended inall children who are newly diagnosed with systemichypertension.19 Noncardiac disease states that affectthe heart such as pulmonary hypertension constitute an important indication for serial pediatricechocardiograms. Echocardiography may also beindicated in children with thromboembolic events,indwelling catheters and sepsis, or superior venacava syndrome.ArrhythmiasChildren with arrhythmias may have underlyingstructural cardiac disease such as congenitally corrected transposition or Ebstein’s anomaly of thetricuspid valve, which may be associated with subtleclinical findings and are best evaluated using echocardiography. Sustained arrhythmias or antiarrhythmic medications may lead to functional perturbations of the heart that may only be detectable byJournal of the American Society of EchocardiographyDecember 2006echocardiography and have important implicationsfor management.INSTRUMENTATION, PATIENT PREPARATION,AND PATIENT SAFETYInstrumentationUltrasound instruments used for diagnostic studiesshould include, at a minimum, hardware and softwareto perform M-mode, 2D imaging, color flow mapping,and spectral Doppler studies, including pulsed waveand continuous wave capabilities. The transducersused in pediatric studies should provide adequateimaging across the wide range of depths encounteredin pediatric cases. Multiple imaging transducers, ranging from low frequency (2-2.5 MHz) to high frequency(ⱖ7.5 MHz), should be available; a multifrequencytransducer that includes all these frequencies is also anoption. A transducer dedicated to the performance ofcontinuous wave Doppler studies should also be available for each study.The video screen and display should be of suitablesize and quality for observation and interpretation of allthe above modalities. The display should identify theparent institution, a patient identifier, and the date andtime of the study. The electrocardiogram should alsobe displayed in real time with the echocardiographicsignal. Range or depth markers should be available onall displays. Measurement capabilities must be presentto allow measurement of the distance between twopoints, an area on a 2D image, blood flow velocities,time intervals, and peak and mean gradients fromspectral Doppler studies.Data Acquisition and StorageEchocardiographic studies must be recorded andstored as moving images and must be stored on amedium that allows for playback of the recordedmoving images. This would include videotape ordigital recording media. It is unacceptable to storeor archive moving echocardiographic images on amedium that displays only a static image, such asrecording film or paper. Portions of the echocardiographic examination such as M-mode frames andDoppler spectral measurements may be displayedand recorded as a static image on media appropriateto the laboratory situation.Patient Preparation and SafetySufficient time should be allotted for each study according to the procedure type. The performance timeof an uncomplicated, complete (imaging and Doppler)pediatric TTE examination is generally 45 to 60 minutes (from patient encounter to departure). Additionaltime may be required for complicated studies. Allprocedures should be explained to the patient and/or
Journal of the American Society of EchocardiographyVolume 19 Number 12parents or guardians before the onset of the study. Thepatient should be placed in a reclining position in acomfortable environment. A darkened room is preferable for the performance of the study. Appropriatepillows and blankets should be used for patient comfort and privacy. The sonographic gel should bewarmed to body temperature before the start of theexamination. It is recommended that appropriate distractions be provided in echocardiographic laboratories performing studies on preschool children. Thesemay include toys, games, television, or movies. Aparent or guardian should accompany all childrenduring the echocardiographic study except whereprivacy issues supersede.The laboratory should recognize the potentialneed for sedation of pediatric patients to obtain anadequate examination. Written policies including,but not limited to, the type of sedatives, appropriatedosing for age and size, and proper monitoring ofchildren during and after the examination shouldexist for the use of conscious sedation in children.20,21Each laboratory should have a written procedurein place for handling acute medical emergencies inchildren. This should include a fully equipped cardiac arrest cart (crash cart) and other necessaryequipment for responding to medical emergenciesin pediatric patients of all sizes.SKILLS AND KNOWLEDGEEchocardiography of congenital and acquired pediatric heart disease is an operator-dependent imagingtechnique that requires high levels of technical andinterpretive skills to maximize its diagnostic accuracy. Specialized training is required in the assessment of cardiovascular malformations to determinetreatment options and to assess outcomes after anever-increasing number of interventional and surgical procedures.PhysiciansBecause TTE is the primary diagnostic imaging modality in children with heart disease, pediatric cardiologists must possess basic skills in performance andinterpretation of transthoracic cardiac ultrasound,including M-mode, 2D imaging, and various Dopplermethods. Physicians who specialize in echocardiography of pediatric heart disease undergo extendedtraining in this domain.This committee reviewed and considered existing guidelines for training in pediatric echocardiography.8,22-24 The American College of Cardiology (ACC) Pediatric Cardiology/Congenital HeartDisease Committee and the ACC Training ProgramDirectors Committee have jointly developed newrecommendations for training in pediatric cardiol-Lai et al 1415ogy. The recommendations in the ACC/AmericanHeart Association/American Academy of PediatricsClinical Competency and Training Statement onPediatric Cardiology (Task Force 2: Pediatric Training Guidelines for Noninvasive Cardiac Imaging) represent the most recent guidelines and, with minormodifications, are incorporated in this document.25Levels of expertise. Physicians who practice TTEmay have one of two levels of expertise, core oradvanced. The core level includes the basic set oftechnical and interpretive skills required for graduation from a pediatric cardiology training programaccredited by ACGME. Physicians with this level ofexpertise are expected to be able to perform andinterpret TTEs in normal infants, children, andadolescents, and in those with childhood heartdisease with consultation as needed. “Advanced” is ahigh level of expertise in all aspects of pediatricechocardiography. Physicians with this level oftraining are expected to be able to perform independently and to interpret echocardiograms in patientswith all forms of congenital and acquired pediatricheart disease, and to supervise and train others.Table 1 outlines the required knowledge for the coreand advanced levels of expertise, and Table 2 delineatesthe required skills. Table 3 outlines the training methodsrecommended for the two levels of expertise.Evaluation of knowledge and skills. Unlike adultechocardiography, there is currently no formal testthat can be used to examine competency in pediatric echocardiography in North America. The optimalevaluation of clinical competence is, therefore,based on assessment of the trainee’s skills by thedirector of the pediatric echocardiography laboratory. Direct observation of the trainee during performance of echocardiograms provides informationabout imaging skills and understanding of the ultrasound instruments. The maintenance of a log ofechocardiograms performed by each trainee is required. Conferences in which echocardiograms arepresented provide an opportunity to assess skills ininterpretation of images and Doppler recordings.Conferences may also be used to promote andevaluate skills in research design and methods, andteaching effectiveness. The laboratory director, inconsultation with the teaching staff, should evaluateeach trainee in writing on a regular basis.Maintenance of knowledge and Skills. Clinicalcompetence in pediatric echocardiography requirescontinued practice of all forms of cardiac ultrasoundtechniques in an active program in which patientswith a wide range of pediatric heart disease are seen.To maintain core-level competence, a minimum of150 TTEs per year should be performed or interpreted. To maintain advanced-level competence, aminimum of 500 TTEs per year should be performedor interpreted. In addition, continued participationin intramural conferences and in continuing medical
Journal of the American Society of EchocardiographyDecember 20061416 Lai et alTable 1 Required knowledge base for core and advanced levels of expertiseLevel of expertiseCoreRequired knowledge base AdvancedUnderstanding of the basic principles of ultrasound physicsKnowledge of the indications for transthoracic echocardiography in pediatric patientsKnowledge of common congenital heart defects and surgical interventionsKnowledge of Doppler methods and their application for assessment of blood flow and prediction of intracardiacpressuresKnowledge of the limitations of echocardiography and Doppler techniquesKnowledge of alternative diagnostic imaging techniquesKnowledge of standard acoustic windows and transducer positionsKnowledge of image display and orientation used in pediatric echocardiographyAbility to recognize normal and abnormal cardiovascular structures by 2-dimensional imaging and to correlatethe cross-sectional images with anatomic structuresFamiliarity with standard echocardiographic methods of ventricular function assessmentFamiliarity with major developments in the field of noninvasive diagnostic imagingIn addition to the knowledge base required in the core level: In-depth knowledge of ultrasound physics Ability to recognize and characterize rare and complex congenital and acquired cardiovascular abnormalities in avariety of clinical settings In-depth understanding of Doppler methods and their application to the assessment of cardiovascular physiology Familiarity with all echocardiographic methods available for assessment of global and regional ventricular function and knowledge of the strengths and weaknesses of these techniques Up-to-date knowledge of recent advances in the field of noninvasive cardiac imaging, including ability to reviewcritically published research that pertains to the field Knowledge of current training guidelines and regulations relevant to pediatric echocardiographyTable 2 Required skills for core and advanced levels of expertiseLevel of expertiseRequired skillsCore Ability to safely, properly, and efficiently use cardiac ultrasound equipment Ability to perform a complete transthoracic echocardiographic examination with proper use of M-mode,2-dimensional, and Doppler techniques in normal pediatric patients and in those with heart disease, with consultation as neededAdvancedIn addition to the skills required in the core level: Ability to perform independently a complete transthoracic echocardiographic examination with proper use of allavailable ultrasound techniques in patients with all types of congenital heart disease Ability to assess cardiovascular physiology and global and regional ventricular function using a variety of ultrasound techniques Ability to supervise and teach pediatric echocardiography to sonographers, pediatric cardiology fellows, andother physicianseducation activities related to advances in echocardiography is essential.SonographersThe committee reviewed and adopted guidelinespublished by the American Society of Echocardiography (ASE) in “Minimum Standards for the CardiacSonographer: A Position Paper” regarding the competence of sonographers performing echocardiograms.26 Separate credentialing requirements applyfor sonographers in each area of subspecialization(ie, pediatric vs adult TTE). A summary of theguidelines is as follows.The ASE believes that there are 3 primary elements involved in assuring the competence of acardiac sonographer.Credentialing and formal education. A cardiacsonographer must obtain a recognized credentialwithin the time frame and using the pathways specified by a credentialing organization recognized by theASE. A new cardiac sonographer entering the fieldmust comply with the formal educational requirements specified by the applicable credentialing organization, and must fulfill those requirements throughparticipation in a program recognized by the ASE.Technical competence. A cardiac sonographer mustdemonstrate and document technical competence in theperformance of those types of echocardiographic examinations that the sonographer performs.Continuing education. A cardiac sonographermust maintain his or her skills through participationin appropriate continuing education.
Journal of the American Society of EchocardiographyVolume 19 Number 12Lai et al 1417Table 3 Training methods recommended for core and advanced levels of expertiseLevel ofexpertiseCoreRecommended methods of training Training should take place in a pediatric echocardiography laboratory that serves a hospital with an accredited pediatriccardiology program, inpatient and outpatient facilities, neonatal and pediatric intensive care departments, a pediatric cardiac catheterization laboratory, and a congenital heart surgery program Supervised performance of at least 150 transthoracic echocardiograms (at least 50 in infants age ⱕ 1 y)* Review at least 150 transthoracic echocardiograms with a qualified staff pediatric echocardiographer* Participate in didactic conferences in which echocardiographic data are reviewed and their clinical applications arediscussed Reading of textbooks, review articles, and original research on pediatric echocardiography Attendance at CME courses that are either dedicated to or include pediatric echocardiographyAdvanced In addition to the training methods described in the core level: Perform at least 200 additional transthoracic echocardiograms (at least 50 in infants age ⱕ 1 y) with subsequent review andcritique of the examinations by the responsible staff pediatric echocardiographer* Review at least 200 additional transthoracic echocardiograms with a qualified staff pediatric echocardiographer* Trainees should gradually attain a high level of independence; the degree and rate at which independence is attainedshould be determined by the director of the laboratory Prepare and present echocardiographic data at clinical and didactic conferences Active participation in research that involves echocardiography of pediatric heart diseaseCME, Continuing medical education.*The recommended numbers of examinations outlined here represent minimal and not optimal requirements.EXAMINATION PROTOCOLExamination PrinciplesAlthough laboratory protocols vary, the basic elements of a standard examination involve 2D imagessupplemented by Doppler and color Doppler information in multiple orthogonal imaging planes. Thestudies are organized by acoustic windows fromwhich the heart is examined. The information maybe recorded in complete sweeps, multiple selectedsingle planes, or with a combination of both techniques.27-29 A complete examination protocolshould outline all views to be obtained, includingtheir preferred order, the imaging modalities to bedeployed for each view, and the preferred methodsfor recording and display. A list of the structures tobe examined with each view is helpful, and therequired versus optional measurements should beclearly defined.Many pediatric echocardiography laboratories begin the examination with subxiphoid, or subcostal,imaging instead of left parasternal views. This allowsfor the determination and display of visceral situs(site or location) at the beginning of an examination.Regardless of where the examination starts, thesegmental approach is used to describe all of themajor cardiovascular structures in sequence.30,31 Anabnormal finding, either structural or hemodynamic,must be fully examined. Quantification of ventricular function is often an important part of the examination.For a pediatric echocardiogram, by convention,the anterior and superior structures are displayed atthe top of the video screen, and the rightwardstructures are generally placed on the left side of theimage display. Therefore, the preferred method ofdisplay is with the image apex “inverted,” with theimage apex at the bottom of the video screen,during subxiphoid and apical imaging to demonstrate structures in their correct anatomic orientation. This is important because of the wide range ofanatomic variations frequently seen in patients withcongenital heart disease. The one exception to theleft-right rule of orientation is the parasternal longaxis view, in which the apex of the heart is displayed on the left side of the video screen in bothlevocardia and dextrocardia.The diagnostic accuracy of an examination depends greatly on the image quality. Technical adjustments must be made by the operator to improvesignal-to-noise ratio and image resolution. The appropriate probe and optimal transducer frequencyare selected to image the structures in question, andadjustments of the electronic (acoustic) focus depthare made throughout the study as necessary. Centering of structures of interest, using an appropriatedegree of magnification, and optimizing of windowsfor imaging and Doppler interrogation are critical forimage quality. Patient position, comfort, and level ofanxiety are important considerations throughout theexamination.As a pediatric echocardiogram is progressing, thesonographer or echocardiographer must keep inmind the indications for the study and the need toaddress issues that may affect treatment as theyarise. A complete examination may require thatcustom, or in-between, planes be used to investigateor display an abnormality. Whatever method ofrecording or display is selected as the laboratory
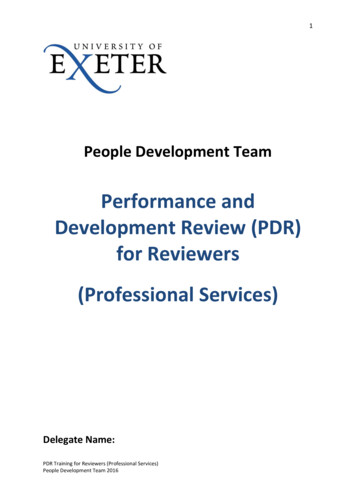
1418 Lai et alstandard, complete sweeps of the heart should bemade during the examination to rule out abnormalities at its base or apex or on one of its surfaces. Inaddition, the major vascular structures must beevaluated as part of a complete examination.Extracardiac structures are visualized during astandard TTE examination. Mediastinal abnormalities such as masses and cysts, if present, should benoted. Careful attention to symmetry and amplitudeof diaphragm motion and screening for pleuraleffusions from subxiphoid and flank windows isparticularly important in postoperative cardiaccases.Multiple Orthogonal Imaging PlanesThe standard views of a 2D echocardiogram, asdefined early on by the ASE,32 are all used as part ofa pediatric echocardiogram. In addition, there areimaging planes that are more commonly associatedwith a routine pediatric study: subxiphoid (subcostal), suprasternal notch, and right sternal border.These imaging planes provide unique informationregarding cardiovascular malformations that are often seen in childhood. A complete examinationrequires that the cardiovascular structures be imaged from multiple orthogonal planes. This practiceminimizes artifacts caused by false dropout of structures imaged parallel to the beam of interrogation orshadowing from reflective structures proximal tothe area of interest.The imaging planes are identified by transducerlocation (subxiphoid, apical, parasternal, suprasternal notch, and right parasternal) and by the plane ofexamination relative to the heart (4-chamber,2-chamber, long-axis, and short-axis). In addition,imaging planes may be described as anatomic planes(sagittal, parasagittal, transverse, or coronal).The views and structures presented below aredescribed as seen in a patient with normal ornear-normal cardiovascular anatomy. Table 4 liststhe structures that should be visualized from thestandard examination views.Subxiphoid (subcostal) views. Subxiphoid imaging33,34 begins with the determination of abdominalvisceral situs in the transverse plane. In addition tovisualization of the liver and stomach, the spleenshould be sought in patients with abnormal abdominal visceral situs. The location of the hepatic segment of the inferior vena cava and descending aortain relation to the midline and one another are thendetermined. As the plane of imaging is angled fromthe abdomen to the thorax, the connections of thehepatic veins to the inferior vena cava are visualized,followed by the connection of the inferior vena cavato the right atrium. The patency of the inferior venacava should be documented; if a dilated azygos veinis seen posterior to the descending aorta, interruption of inferior vena cava should be suspected. TheJournal of the American Society of EchocardiographyDecember 2006Table 4 Structures viewed from standard examinationviewsSubxiphoid (subcostal) viewsInferior vena cavaHepatic veinsAbdominal aortaDiaphragmSuperior vena cavaLeft atriumRight atriumAtrial septumCoronary sinusPulmonary veinsMitral valveTricuspid valveLeft ventricleRight ventricleVentricular septumLeft ventricular papillarymusclesAortic valvePulmonary valveAscending aortaCoronary arteriesMain and branch pulmonaryarteriesPericardiumApical viewsInferior vena cavaLeft atriumRight atriumAtrial septumCoronary sinusSelected pulmonary veinsMitral valveTricuspid valveLeft ventricleRight ventricleVentricular septumLeft ventricular papillarymusclesAortic valvePulmonary valveAscending aortaMain and branch pulmonaryarteriesLeft parasternal viewsInferior vena cavaSuperior vena cavaLeft atriumRight atriumAtrial septumCoronary sinusPulmonary veinsMitral valveTricuspid valveLeft ventricleRight ventricleVentricular septumLeft ventricular papillary musclesAortic valvePulmonary valveAscending aortaCoronary arteriesMain and branch pulmonaryarteriesPericardiumSuprasternal notch viewsSuperior vena cavaLeft atriumPulmonary veinsAscending aortaSuperior thoracic aortaMain and branch pulmonaryarteriesAortic archProximal brachiocephalic arteriesLeft innominate veinRight parasternal viewsInferior vena cavaSuperior vena cavaRight atriumAtrial septumRight pulmonary veinsAscending aortaRight pulmonary arterydescending aorta at the level of the diaphragmshould be interrogated by Doppler. Any additionalvascular structures crossing the diaphragm shouldbe fully investigated.The subxiphoid long-axis sweep (Figure 1) beginsin the transverse plane and passes the inferior/posterior surface of the heart, which includes thecoronary sinus. The position of the left coronaryostium is well visualized as the ascending aorta isimaged. The posterior descending coronary arterymay be seen in the posterior interventricular groove.The long-axis view allows for good visualization of
Journal of the American Society of EchocardiographyVolume 19 Number 12Lai et al 1419Figure 1 Subxiphoid long-axis views demonstrated in sweep from nearly coronal plane back towardtransverse plane. 1, Right ventricular (RV) inflow and outflow are seen with pulmonary valve. 2, Withinferior angulation, long axis of left ventricle (LV), aortic (Ao) valve, and ascending Ao are seen. Superiorvena cava (SVC) is seen to right of ascending Ao, and main pulmonary artery (MPA) is seen to left.Connection of SVC to right atrium (RA) is demonstrated. 3, As transducer is angled back towardabdomen, atrial septum and pulmonary venous connections to left atrium (LA) are viewed. (Reproducedwith permission from: Geva T. Echocardiography and Doppler ultrasound. In: Garson A, Bricker JT,Fisher DJ, Neish SR, editors. The science and practice of pediatric cardiology. Baltimore: Williams andWilkins; 1997, p. 789-843).the atrial septum and color Doppler mapping of theanterior muscular septum.The subxiphoid short-axis sweep (Figure 2) startsin a parasagittal plane that includes the inferior andsuperior venae cavae. Imaging normally begins tothe right, allowing
Pediatric Cardiology (Task Force 2: Pediatric Train-ing Guidelines for Noninvasive Cardiac Imaging) rep-resent the most recent guidelines and, with minor modifications, are incorporated in this document.25 Levels of expertise. Physicians who prac