Transcription
Between 1934 and 2016,the ABP certified 118,292pediatricians (pg 22).In 2016, 3,572 first-yearpediatric residents were intraining, a 17% increasesince 2001 (pg 35). Inaddition, 1,383 first-yearfellows were in training, an84% increase since 2001(pg 68).Of those recently takingtheir GP certifyingexamination, 40% plan onconducting researchduring their career (pg 60).Since 2001, the percent offemales entering asubspecialty fellowshipprogram has risen from50% to 68% (pg 68).Since 2001, the pediatricsubspecialty experiencingthe most growth in thenumber of first-year fellowshas been pediatricemergency medicine(134%) (pg 70).Pediatric PhysiciansWorkforce Data Book2016-2017THE AMERICAN BOARD of PEDIATRICS
Founded in 1933, the American Board of Pediatrics (ABP) is one of 24 physician certifying boards of theAmerican Board of Medical Specialties (ABMS). The ABP is an independent, nonprofit organization whosecertificate is recognized throughout the world as a credential signifying a high level of pediatric physiciancompetence.As a part of the ABP’s ongoing operations, data are compiled annually to generate this workforce data bookfor the benefit of the pediatric community and the public at large. Data are provided only in aggregate andin accordance with the ABP’s privacy policy, which can be found athttps://www.abp.org/content/privacy-policy.The information provided throughout this publication does not imply the expression of any opinion on thepart of ABP concerning the workforce needs of any area, state, territory, or country.CC BY-NCThis work, Pediatric Physicians Workforce Data Book, 2016-2017, issued by the American Board ofPediatrics, is licensed under a Creative Commons Attribution-Noncommercial 4.0 International License:made available at http://creativecommons.org/licenses/by-nc/4.0/. Permissions beyond the scope ofthis license may be available by contacting workforce@abpeds.org.Published by:The American Board of Pediatrics111 Silver Cedar CourtChapel Hill, NC 27514Telephone: 919-929-0461Web: www.abp.orgEmail: workforce@abpeds.orgSuggested Citation:American Board of Pediatrics, Pediatric Physicians Workforce Data Book, 2016-2017, Chapel Hill, NC:American Board of Pediatrics, 2017.2
Table of ContentsForeword . 4Acknowledgements . 5History of the ABP’s Pediatric Physicians Workforce Data Book . 6Methodology . 7Pediatric Physician Workforce: Entry and Progression . 7Description of Data Collection Points. 8Guide to Data Interpretation . 9Major Changes to the Pediatric Physicians Workforce Data Book in 2016 - 2017. 10Additional Resources. 11Key Definitions . 13Section 1. General Information on All Certified Diplomates . 19Section 2. General Pediatrics Residency Tracking Data . 32Section 3. General Pediatrics Certifying Examination Census Survey . 50Section 4. Subspecialty Fellowship Tracking Data . 65Section 5. Individual Subspecialty Information: General Information, Fellowship Tracking Data, andSubspecialty Certifying Examination Census Survey . 725.1. Adolescent Medicine . 755.2. Pediatric Cardiology . 935.3. Child Abuse Pediatrics . 1115.4. Pediatric Critical Care Medicine .1295.5. Developmental-Behavioral Pediatrics .1475.6. Pediatric Emergency Medicine.1655.7. Pediatric Endocrinology .1835.8. Pediatric Gastroenterology .2015.9. Pediatric Hematology-Oncology .2195.10. Pediatric Infectious Diseases .2375.11. Neonatal-Perinatal Medicine .2555.12. Pediatric Nephrology .2735.13. Pediatric Pulmonology .2915.14. Pediatric Rheumatology .309Section 6. Maintenance of Certification Enrollment Census Survey .3273
ForewordWelcome to the Pediatric Physicians Workforce Data Book, 2016-2017.For more than two decades, the ABP has shared workforce data about pediatric physicians with the largermedical community through the publication of an annual workforce data book. Over the years, this reporthas evolved to incorporate information across the entire span of a pediatrician’s career, from training andcertification through Maintenance of Certification (MOC). While we affirm that high quality pediatric careincreasingly relies on teams of professionals with backgrounds in multiple disciplines and specialties, thisreport builds on data available to the ABP concerning pediatric physicians.Tracking the pediatric physician workforce is essential for understanding its makeup, numbers, distribution,and practice patterns, but it is not just about publishing numbers. We believe this report provides valuableinformation to pediatricians, pediatric residency and subspecialty training program directors, hospitaladministrators, policymakers, researchers, and others interested in ensuring that we have the skilledworkforce necessary to meet the health care needs of infants, children, adolescents, young adults, andtheir families.With this edition of the workforce data book, we have made numerous changes in the presentation andcontent of the information provided. We welcome your feedback as we seek to continually improve ourprocesses.Last, the scope and depth of the current ABP Pediatric Physicians Workforce Data Book, 2016-2017, wouldnot be possible without the information provided by trainees, program directors, and diplomates. We thankeach of you for your commitment to ensuring that every infant, child, adolescent, and young adult, nomatter what their background or where they live, has access to quality pediatric care.Sincerely,David G. Nichols, MD, MBAPresident & CEO,American Board of PediatricsLaurel K. Leslie, MD, MPHVice President, ResearchAmerican Board of Pediatrics4
AcknowledgmentsIn addition to the many program directors, residents, fellows, and practicing pediatricians without whom thisworkforce book would not be possible, the ABP also thanks its staff who assisted in data collection,entry, and management and in the production of the Pediatric Physicians Workforce Data Book, 2016-2017.ABP Workforce Project Team:Andrew Dwyer, PhDWorkforce Project Statistical ConsultantCathleen Koenig, MSWorkforce Project Data AnalystLaurel K. Leslie, MD, MPHWorkforce Project Senior AuthorAshley Tucker, MPHWorkforce Project Administrative AssistantAdam Turner, MPH, PMPWorkforce Project Primary Author and Project LeadSpecial Advisors:Linda A. Althouse, PhDVice President, Psychometrics & Assessment ServicesGail McGuinness, MDExecutive Vice PresidentVirginia A. Moyer, MD, MPHVice President, MOC & QualityThe ABP Workforce Project Team welcomes questions regarding the data presented in this book, as well asany comments and suggestions you may have for future editions. Please contact us at workforce@abpeds.org.5
History of the ABP’s Pediatric Physicians Workforce Data BookThe ABP was founded in 1933 and is one of 24 boards that make up the American Board of MedicalSpecialties (ABMS). These boards set standards for the various medical specialties that the public reliesupon to provide high quality health care. The ABP certifies general pediatricians and pediatric subspecialistsbased on standards of excellence that lead to high quality health care during infancy, childhood,adolescence, and the transition into adulthood. Its certifying examinations and assessment processes arean important mechanism through which the profession of pediatrics sets expectations regardingprofessionalism, pediatric practice, continuous learning, and ongoing practice improvement.The ABP has a long-standing history of gathering data regarding the pediatric physician workforce to informboth graduate medical education policy and workforce planning. The ABP gathers data through censussurveys administered in concert with its various examination processes, as well as tracking data collectedfrom program directors about the characteristics of residents and fellows in accredited training programs inthe United States, Puerto Rico, and Canada. These data have been used by program directors, hospitaladministrators, researchers, policymakers, and others. They provide a comprehensive view of the pediatricphysician workforce, from trainees in their first year of a medical residency through physicians engaged inretirement planning. These data also permit tracking of trends over time.The first workforce data book was published in 1992 under the leadership of James A. Stockman III, MD,President and CEO of the ABP from 1992 to 2012, with initial oversight provided by Robert Guerin, PhD,Vice President. The 1992 report included responses to census surveys administered at the time ofapplication to take the General Pediatrics Examination, as well as tracking data for first-year pediatrictrainees (Level 1) in Categorical General Pediatrics (GP) residency training programs.Since 1992, the ABP has published its workforce data annually; however, the content and format of thereport have changed over the last 24 years. Changes to the tracking data reported in the workforce databook have reflected changes in data collected from program directors as well as in the composition andcontent of pediatric resident and fellowship training programs. Tracking data on second- and third-yeartrainees (Levels 2 and 3) were first collected and reported in the workforce data book in 1993 and 1994,respectively. In 1995, the ABP began collecting tracking data on first-year subspecialty fellows, but the datawere not considered sufficiently robust to include in the workforce book until the early 2000s. In addition,the ABP has added certifying examinations in several new subspecialties including DevelopmentalBehavioral Pediatrics (2002) and Child Abuse/Pediatrics (2009), as well as in several areas in concert withone or more of the other boards within ABMS (e.g., Hospice and Palliative Medicine [2008]).Changes to the workforce data book also have reflected a more extensive approach to the ABP’s censussurveys pursued under the leadership of Dr. Stockman; Gail A. McGuinness, MD, ABP Executive VicePresident (2002 to date); Linda Althouse, PhD, Vice President of Psychometrics & Assessment Services(2008 to date); and Gary L. Freed, MD, MPH, then Director of the Child Health Evaluation and ResearchCenter (CHEAR) at the University of Michigan. Often, these efforts were initiated in response to specificprojects undertaken by the ABP. For example, in 2009, the ABP, in concert with CHEAR, began collectingcensus survey data at the time of the resident in-training examinations (ITE) to inform the ABP’s ResidencyReview and Redesign Project (R3P). In 2009, the ABP launched its Maintenance of Certification (MOC)Enrollment Application Census Survey to include census survey data on practicing pediatricians; earlyanalyses focused on clinically inactive pediatricians. Additional data collection with subspecialty fellowsbegan as part of the Subspecialty Clinical Training and Certification (SCTC) Task Force (2010-2013) efforts,which examined the clinical training aspects of subspecialty pediatric training.To read more about changes to this edition of the report, please see the subsection entitled “Major Changesto the Pediatric Physician Workforce Data Book in 2016-2017” on page 10.6
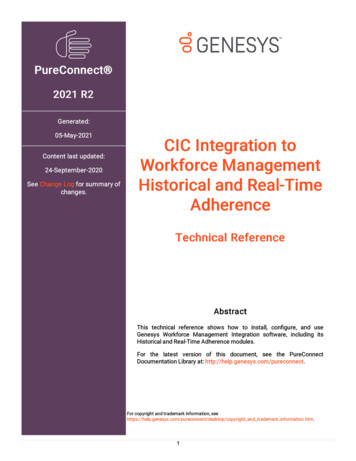
MethodologyThis section first describes the entry into, and progression through, pediatric residency training, certification,and Maintenance of Certification (MOC). Second, data collection efforts at the ABP are described withrespect to both tracking data and census surveys. Last, this section highlights additional changes made tothis edition of the data book, as well as additional resources that may be helpful when considering thelarger pediatric workforce.Pediatric Physician Workforce: Entry and ProgressionThe ABP’s interactions with a trainee begin once s/he completes medical school, either in the United States(U.S.) or internationally, and starts their residency training (see Figure A). In categorical pediatric residencyprograms, training typically lasts three years. The duration may be longer for individual residents if they arein training programs that are integrated with more than one of the American Board of Medical Specialties(ABMS)-approved specialties (for example, Medicine-Pediatrics (Med-Peds) programs provide training in bothadult and pediatric medicine and require four years of training). Alternatively, training may be shorter incertain circumstances (e.g., an international medical graduate is approved for having completed previoustraining in a non-accredited general pediatrics residency program).Most individuals choose to obtain board certification at the end of their training. Certification is a voluntaryprocess that goes above and beyond requirements for practicing medicine set by state licensing boards.Residents seeking initial certification in General Pediatrics (GP) through the ABP must: 1) complete anAccreditation Council of Graduate Medical Education (ACGME)-accredited training program in pediatrics, 2)receive an attestation from their program director of satisfactory performance during residency in each of sixdomains specified by the ACGME, and 3) obtain a valid, unrestricted medical license through the medicalboard in one or more states. The six domains specified by the ACGME, and endorsed by the ABP and ABMS,include professionalism, medical knowledge, patient care and procedural skills, practice-based learning andimprovement, interpersonal and communication skills, and systems-based practice.Upon passing the GP Certifying Examination, a pediatrician becomes an ABP diplomate and is automaticallyenrolled in MOC. Pediatricians may voluntarily elect to maintain their certification by participating in MOC. Ifa pediatrician participates in MOC, s/he chooses to meet standards of excellence with respect to lifelonglearning, assessment, and practice improvement. The ABP continues to track diplomates who participate inMOC throughout their careers.Pediatricians who have successfully completed their GP residency may choose to pursue subspecialtycertification and begin a pediatric subspecialty fellowship program (see second pathway in Figure A), even ifthey have not yet taken their GP Certifying Examination. However, they cannot be certified in a pediatricsubspecialty until they are certified in general pediatrics. Examples of pediatric subspecialties includepediatric nephrology, pediatric cardiology, and developmental-behavioral pediatrics.Subspecialty fellowship training typically follows a path towards certification similar to the GP certificationpathway. Depending on the subspecialty, certification may be administered by the ABP or administered byone of the other ABMS boards (e.g., American Board of Internal Medicine). In the case of co-sponsorship,Subspecialty Certifying Examinations may be administered to the other member boards’ diplomates, butcertification is awarded by the parent board (e.g., ABP to ABP diplomates and ABIM to ABIM diplomates).Figure A. Workforce Entry & ProgressionMedical SchoolChoice ofSpecialty andMatch ication andExaminationDiplomate Careerand Maintenanceof tificationApplication andExaminationDiplomate Careerand Maintenanceof Certification7
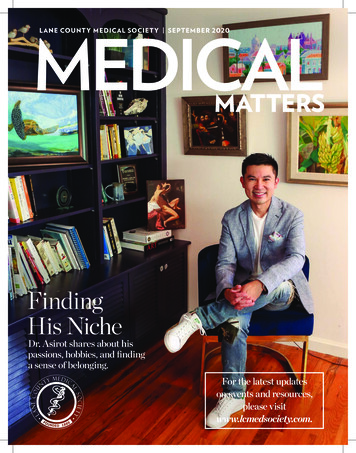
Description of Data Collection PointsThe information presented in this report is a consolidation of data collected for normal business operationsat the ABP through the tracking data and census surveys that ask questions about current and futurepractice patterns. Data are only reported in aggregate.Residency program directors submit basic tracking data annually to the ABP that includes demographics oftheir current pediatric residents as well as information about whether an individual resident is meetingstandards of clinical and professional performance set by the ABP. This tracking information informs the ABPregarding the number and demographics of residents who qualify to “sit for” (or “take”) the GP CertifyingExamination upon completion of their GP residency training. These tracking data are collected annually andplaced into the ABP’s Certification Management System (CMS).As a trainee progresses through residency, GP certification, subspecialty certification, and ultimately intoparticipation in MOC, the ABP collects and stores information. Figure B below illustrates a standard exampleof a trainee in a categorical general pediatrics residency.Data collection begins in the first year of residency with residency tracking data provided by residencyprogram directors at the time of the General Pediatrics In-Training Examination (GP ITE). The ABP offers theGP ITE to pediatric residents each year during their residency training. GP ITE scores are not used to makedecisions regarding board certification, but rather is intended to be used for educational purposes only. Anindividual trainee, in concert with his/her program director, may use the ITE scores to identify gaps in his/herknowledge. Program directors may also identify general gaps in knowledge across trainees at their program.A post-examination census survey is associated with the GP ITE in each year of training.Figure B. Workforce Data Collection for a Resident Completing a Categorical General Pediatrics Residency GP ResidencyYrs 1-3 The ABP receives tracking data from ACGME and Royal College of Physiciansand Surgeons of Canada accredited residency programs annually.Following the completion of the GP ITE, offered during each year ofresidency, a census survey is administered. GP CertificationProcessYrs 3-4MOC ProcessYrs 5-10, 11-15,etc.Residents who have met training requirements complete an application totake the GP Certifying Examination; a census survey is administered as partof that application process. Following the completion of the GP Certifying Examination, another census surveyis administered. After passing the GP Certifying Examination, diplomates are automaticallyenrolled in their first 5-year MOC cycle. At the beginning of the second cycle and each 5-year cycle thereafter,diplomates must re-enroll in MOC, and an accompanying census survey isadministered.Before residency is completed, usually in the third year of training, residents can apply to take the GPCertifying Examination. Workforce census surveys are administered during the application process and,again, at the time a resident sits for the GP Certifying Examination. Often, when analyzing the data in thecensus surveys, the ABP uses responses from first-time takers, as graduated residents can take theexamination as many times as needed to pass, up to 7 years following residency completion. Analyses tablesand figures in this workforce data book are notated with the corresponding sample information.After a resident passes the GP Certifying Examination, s/he is considered a diplomate and is automaticallyenrolled in his/her first 5-year MOC cycle in the following year. At the end of that 5-year cycle, a diplomatemust complete an MOC application to enter a second, 5-year MOC cycle in the following year. A workforcecensus survey is associated with each opportunity for re-enrollment in MOC. It is important to note that thereis a duration of a least five years between when a diplomate takes his/her certifying examination and reenrolls in MOC. While most diplomates do meet MOC requirements and continue MOC on the regular 5-year8
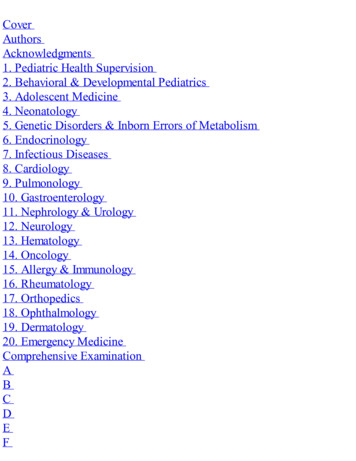
cycle, some allow their certifications to lapse by not completing all MOC requirements, thereby extending thetime between census surveys to greater than 5 years.While the text above details data collection points from the viewpoint of a general pediatrics diplomate,many of the same data collection points are relevant for individuals participating in a pediatric subspecialtyfellowship program and pursuing subspecialty certification. Program directors share information about thenumbers and demographics of individuals participating in their training programs. Pediatric subspecialtyfellows apply for and take Subspecialty In-Training Examinations (SITE). Subspecialty fellows may be askedto complete a census survey with their initial subspecialty certification application and following theirSubspecialty (SS) Certifying Examination. Figure C below depicts the experience of the standard subspecialtyfellowship participant.It should be noted that pediatric diplomates may choose at any time to exit this system by not re-enrolling inMOC, although most pediatricians do maintain certification. Thus, some tables in this report do not captureall practicing pediatricians, particularly those in Section 6. Maintenance of Certification Enrollment CensusSurvey. In these instances, the authors of this report have made notations regarding the included sampleand considerations for interpretation.Figure C. Workforce Data Collection for Diplomates Completing a Standard Subspecialist Fellowship SS FellowshipYrs 4-6 The ABP receives tracking data from ACGME and Royal College of Physiciansand Surgeons of Canada accredited fellowship programs annually.After completing the Subspecialty In-training Examination, offered during eachyear of fellowship, a census survey is administered. SS CertificationProcessYrs 6-7 MOC ProcessYrs matched withGP MOC cycleFellows who have met requirements complete an application to take theSubspecialty Certifying Examination; a census survey is administered as apart of the application process.Following the completion of the Subspecialty Certifying Examination, anothercensus survey is administered. After passing the Subspecialty Certifying Examination, a diplomate’s currentMOC cycle becomes his/her MOC cycle for all ABP-held certifications.Guide to Data InterpretationIndividuals using the information in this report should be aware of several considerations for datainterpretation, both for the data presented in this report and if trends are calculated comparing these datawith data presented in previous reports.Why might this be important? Clinical activity of the pediatric workforce is complex to measure. Section 1 provides information onall pediatricians ever certified over time. In addition, estimates are provided for the number ofpediatricians by state. However, the ABP is unable to report on whether individuals are clinicallyactive. Any data used for workforce estimates should control for rates of clinical inactivity and parttime employment among pediatricians. Section 6 provides estimates of clinical activity/inactivity andfull-time/part-time status for those diplomates who have participated in the Maintenance ofCertification (MOC) Enrollment Census Survey (i.e., diplomates at least five years out from their initialGP certification) and may be helpful for any estimates.Certification is a complex process that is continually evolving. The types of residency andsubspecialty programs that are required for certification have changed over time as certificationprocesses have changed. Table 1.1. displays the numbers of pediatric diplomates ever certified by9
subspecialty; several of the subspecialties did not exist when the first workforce data book waspublished in 1992. Others have changed in important but subtle ways.SS Certifying Examinations are typically offered every other year. Regardless of when training ends, arecently graduated fellow may have to wait anywhere from a few months to more than a year beforea certifying exam in his/her subspecialty is available. This also affects how frequently census surveyinformation is collected for each subspecialty, as the survey is administered after the SS CertifyingExamination. Accordingly, the data included in this book from these census surveys may be fromeither 2015 or 2016.MOC has also evolved. Prior to 1980, a formalized, systematic mechanism to re-assess apediatrician’s knowledge or skills did not exist. Voluntary recertification began in 1980 andcontinued to evolve into the MOC process of today. Currently, individuals who have obtained theirinitial certification on or after May 1, 1988, and who wish to maintain certification must participate inMOC.The ABP has changed its data collection processes for the residency and subspecialty trainingprogram tracking data in the ABP’s Certification Management System over time. For example, chiefresidents are currently included in program directors’ reports to the ABP. They will be excludedbeginning in 2018-2019 so that the tracking data collection reverts to its primary mission: to trackindividuals who are seeking certification.The content, timing, and processes of the ABP’s census surveys have changed over time. For 20162017, data are reported from the GP Certifying Examination Census Survey, SS CertifyingExamination Census Survey, and MOC Enrollment Census Survey. Census surveys administeredduring the In-Training Examinations (ITE) were being revised during the development of this bookMajor Changes to the Pediatric Physicians Workforce Data Book in 2016-2017In 2015-2016, the ABP embarked on a review of the tracking and census data collected and published inthe annual workforce book under the leadership of Laurel K. Leslie, MD, MPH, Vice President, Research,2015 to date. As part of that process, the ABP garnered feedback from a variety of stakeholders who haveused the data in the workforce data book to inform planned revisions.Changes to the workforce data book this year include:General Formatting: Additional Information on the History, Content, and Methodology of the Pediatric PhysiciansWorkforce Data Book. In this version, the background text has been expanded to permit the readerto better understand the history of the ABP’s annual workforce data books and its data collectionand analysis processes. Additional Information on Entry and Progression in Pediatrics. Because not all readers may beknowledgeable about pediatric training and certification processes, information has been added onentry into and progression through the field of pediatrics. Key Definitions. Given that not all the readers are familiar with terms commonly employed indescribing pediatric physicians’ training and certification processes, a section has been addeddefining commonly used terms and abbreviations.Changes to Tables, Figures, and Maps: Inclusion of Data Source, Sample, Response Rate, Missing Data, and Considerations forInterpretation in each Table, Figure, or Map. Footnotes have been added to most tables to aid thereader in data interpretation. These include:o Source of Data. Data presented vary in their source and may be drawn from tracking dataentered into the ABP’s Certification Management System (CMS), results from the threecensus surveys described previously, or another source such as U.S. Census Data.10
Sample. The samples for the tables published in the following secti
Pediatric Physicians Workforce Data Book 2016-2017 Between 1934 and 2016, the ABP certified 118,292 pediatricians (pg 22). In 2016, 3,572 first-year pediatric residents were in training, a 17% increase since 2001 (pg 35). I