Transcription
GeriatricPhysical TherapyDescription ofSpecialty PracticeN BOARDICAOERMLIASICALTIEP HYSFASpecialty Council onGeriatric Physical TherapyT HE R A P Y S P ECAmerican Board of Physical Therapy Specialties
The Geriatric Description of Specialty Practice was prepared by themembers of a subject matter expert group and members of theSpecialty Council on Geriatric Physical Therapy and approved by theAmerican Board of Physical Therapy Specialties of the AmericanPhysical Therapy Association.Specialty Council on Geriatric Physical TherapyDeborah Kegelmeyer, PT, DPT, GCSMyla Quiben, PT, DPT, GCS, NCSTamara Gravano, PT, DPT, GCSSubject Matter ExpertsDon Backstrom, PT, MBA, GCSMaureen Euhardy, PT, MS, GCSCelinda Evitt, PT, PhD, GCSJill Heitzman, PT, DPT, GCS, FCCWSAnne Myer, PT, DPT, GCS, FCCWSSue Schuerman, PT, PhD, GCSWilliam Staples, PT, DPT, GCSConsultantJean Bryan Coe, PT, DPT, PhDThroughout this document, the editors have attempted to use language consistent with the Guide to Physical Therapist Practice anduniversally accepted concepts and terminology, without bias to anyparticular philosophy or school of thought. The references citedwith the case scenarios are given only to help the reader understandthe specific examples and are not intended to favor any particularschool of thought or philosophy. In addition, these references arenot intended to be inclusive.SLIASICALTIEP HYSpecialty Council on Geriatric Physical TherapyN BOARDICAOERMFAmerican Board of Physical Therapy SpecialtiesAThe Specialty Council on Geriatric Physical Therapy encouragesyour suggestions for improvement of this document. Your input andsuggestions will be considered in the development of the nextrevision. This is a working document and will be modified asnecessary.T HE R A P Y S P EC 2009, 1999, 1990 by the American Physical Therapy Association. Allrights reserved. No part of this document may be reproduced in any formor by any electronic or mechanical means, including information storageand retrieval systems, without written permission of the publisher.ISBN 978-1-931369-65-7For more information about this and other APTA publications, contact theAmerican Physical Therapy Association, 1111 North Fairfax Street,Alexandria, VA 22314-1488, 800/999-APTA (2782), www.apta.org.[Order No. E-45]
GeriatricPhysical TherapyDescription ofSpecialty PracticeN BOARDICAOERMLIASICALTIEP HYSFASpecialty Council onGeriatric Physical TherapyT HE R A P Y S P ECAmerican Board of Physical Therapy Specialties
Geriatric Physical TherapyTable of ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1Chapter 1: Description of Board-Certified Specialists in Geriatric Physical Therapy . . . 2Chapter 2: Description of Specialty Practice in Geriatric Physical Therapy . . . . . . . 4I. Knowledge Areas of Clinical Specialists in Geriatrics . . . . . . . . . . . . . . . . . 4A. Foundation Sciences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4B. Clinical Sciences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4C. Behavioral Sciences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4II. Professional Roles, Responsibilities, and Values of Clinical Specialists in Geriatrics . . 4A. Professional Behavior . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4B. Professional Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4C. Communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5D. Social Responsibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5E. Leadership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5F. Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5G. Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5H. Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5I. Advocacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5J. Evidence-based Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6III. Practice Expectations for Clinical Specialists in Geriatrics in the Patient/ClientManagement Model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6A. Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6B. Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9C. Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9D.Prognosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9E. Intervention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10F. Outcomes Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Chapter 3: Linking Practice Dimensions and ProfessionalResponsibilities to Knowledge Areas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13I. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13II. Case Scenarios . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Chapter 4: Examination Content Outline and List of Medical ConditionsSeen by Specialists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Chapter 5: Executive Summary of Practice Analysis . . . . . . . . . . . . . . . . . .I. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .II. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .A. Survey Instrument . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .B. Pilot Surveys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .III. Final Survey Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . .IV. Data Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .V. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .VI. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .iiII222222222222232323
Description of Specialty PracticeIntroductionHistory of Specialization in Physical TherapyIn 1975, the House of Delegates of the American PhysicalTherapy Association (APTA) approved the concept of specialization and created the Task Force on Clinical Specialization.The task force was charged with identifying and definingphysical therapy specialty practice areas and with developingthe structure for and function of a Board-certified process.The document developed by the task force, “Essentials forCertification of Advanced Clinical Competence in PhysicalTherapy,” was adopted by the House of Delegates in 1978. Atthat time, the House recognized four specialty areas: cardiovascular/pulmonary, neurology, orthopedics, and pediatrics.In 1979, the House appointed the Commission for theCertification of Advanced Clinical Competence. Specialtycouncils for each of the four specialty areas were appointed bythe commission and charged with the development of competencies unique to the advanced clinician in their respectiveareas.In 1980, the Commission became the Board of Certificationof Advanced Clinical Competencies (BCACC). The Houseof Delegates recognized two more specialty areas that sameyear: sports and clinical electrophysiology. In 1985, the“Essentials for Certification of Advanced Clinical Competencein Physical Therapy” was revised by the House of Delegatesand the title was changed to “Essentials for Certification ofPhysical Therapist Specialists.” The BCACC was renamed theAmerican Board of Physical Therapy Specialties (ABPTS), andthe first specialty examination was administered in cardiovascular/pulmonary physical therapy that same year. The specialtyarea of geriatrics was approved in 1989. In June of 2006, theAPTA House of Delegates approved Women’s Health as thenewest area of physical therapist specialty practice.History of Specialization in Geriatric Physical TherapyThe Section on Geriatrics published its first report on specialization in geriatric physical therapy in 1982.1 In 1984 Whartonconducted a study that identified advanced-level tasks and theknowledge, skills, and attitudes needed for competent practice by physical therapists who work with geriatric patients.2In 1987 the Section on Geriatrics appointed a specializationtask force, chaired by Bonnie Teschendorf. In 1989 the APTAHouse of Delegates accepted the Section on Geriatrics’ petitionin support of geriatric specialization. Andrew Guccione, PT,PhD, FAPTA, Marybeth Brown, PT, PhD, and Rita Wong,PT, EdD, were appointed as the first members of the SpecialtyCouncil on Geriatric Physical Therapy. The council surveyedselected members of the Section on Geriatrics and membersof other sections who were considered content experts in thecompetencies originally identified in the Wharton study andthe Teschendorf task force. These survey data were used to fullydevelop the competencies that were subsequently approved bythe American Board of Physical Therapy Specialties (ABPTS)in June 1990. The first geriatrics specialist certification examination was given in February 1992.3The original Geriatric Physical Therapy Competencies werebased on the work of Wharton and were divided into sevenareas: (1) biology, psychology, and sociology of aging; (2)patient care; (3) communication; (4) education; (5) administration; (6) consultation; and (7) scientific inquiry.1 Since1989 major changes have occurred in the field of geriatricsand gerontology. For example, the science of age-related andpathological changes with aging has increased; the knowledgeof physical therapy examinations and interventions has grown;and the settings and regulations in practice have changed. Bythe mid-1990s these changes were so pervasive that the specialty council felt strongly that the original framework might notbe adequate to revalidate geriatric specialty practice. Therefore,a panel of past and current members of the Specialty Councilon Geriatric Physical Therapy met in Washington, DC, inApril 1996 to discuss a framework for the new Descriptionof Advanced Clinical Practice (DACP). Those who attendedthis meeting were Rita Wong, Marybeth Brown, AndrewGuccione, Jill Johnson, PT, MS, GCS, Linda Crews, PT,MHS, GCS, and Kathleen Kline Mangione, PT, PhD, GCS.This group constituted the subject matter experts (SME) forthe revalidation study. The day-long meeting resulted in a consensus decision that the framework for the DACP would be ANormative Model of Physical Therapist Professional Education:Version 97 4 and the Guide to Physical Therapist Practice.5Laurita Hack, PT, PhD, FAPTA, was the survey consultant.References1. Greenwald NF. Educational activities related to geriatrics in physical therapy. Geritopics.1982;5(3):9-10.2. Wharton MA. Identification of Advanced Level Performance Tasks in Geriatric Physical Therapy[master’s thesis]. Pittsburgh, PA: University of Pittsburgh; 1985.3. Guccione AA, Brown M, Wong RA. Geriatric Physical Therapy Specialty Competencies.Alexandria, VA: American Board of Physical Therapy Specialties; 1990.4. A Normative Model of Physical Therapist Professional Education: Version 97. Alexandria, VA:American Physical Therapy Association; 1997.5. Guide to Physical Therapist Practice. Phys Ther. 1997;77:1163-1650.1
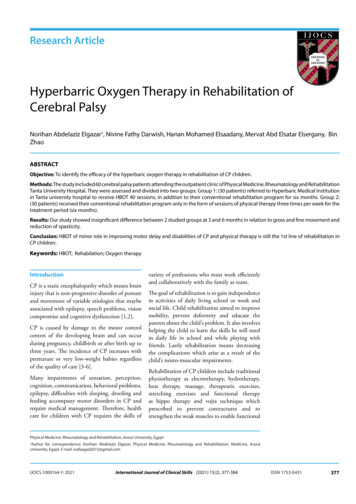
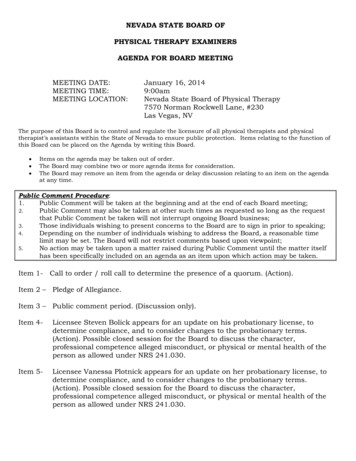
Geriatric Physical TherapyChapter 1: Description of Board-Certified Specialists in Geriatric Physical TherapyThe practice analysis survey drew responses from 395 practitioners, including 277 Board-certified specialists (GCS) and 118noncertified Geriatrics Section (GS) members. The following statistical information is based on the GCS survey respondents.While ABPTS collects similar data on all newly board-certified or recertified specialists, this survey sample (51 % response rate)represents the most current descriptive information on geriatric clinical specialists.1. Years of practice in physical therapy2. Level of education at entry into the profession8820073166150511003127805007Less than 1-2a year years031 years3. Highest-earned academic degree9CertificateBaccalaurete Master’sDegree4. Years of practice in geriatric physical therapy2Less than 1 YearAdvanced Master’s DegreeMaster’s Degree9311-15 Years4916-20 Years27No degreesbeyond entry level13530626-10 Years310203-5 Years61Doctoral Degree (PhD/EdD/clinical doctorate, other)61-2 Years20DPTDoctoralDegree60905. Sex12015021-30 Years41331 Years0204060806. Race/ethnic originAmerican Indian orAlaskan Native22.7316Asian or Pacific Islander4African American/Black200White77.3Hispanic/Latino3Pacific Islander orNative Hawaiian02Other0210050100150200
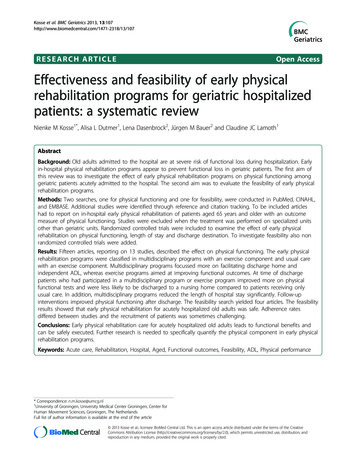
Description of Specialty Practice7. Educational method most used to develop geriatric clinical skills8. Have you been recertified?102Self ng210NO50Formal 3060901201509. Do you have another board certification?10. What is your primary current employment status?No89.5Full-time salaried/hourly20543Part-time salaried/hourlyFull- timeself employed20Part-timeself employedYes5.16Volunteer/ 0pro bono05010015020025012. Are you an APTA member?11. AgeUnder 25 YearsYes89.403325-34 Years11635-44 Years45-54 Years9755-64 Years26No10.6365-74 Years075 Years02040608010012013. Are you a member of the Section on Geriatrics?Yes79.5No20.53
Geriatric Physical TherapyChapter 2: Description of Specialty PracticeThe Description of Specialty Practice (DSP) describes the practiceof geriatric clinical specialists. It is based on the results of a practice analysis survey conducted in 2007. The results of responsesfrom 395 specialist and nonspecialist Section on Geriatrics members are presented in the following document.The content of the practice analysis survey was based on theGuide to Physical Therapist Practice,1 including the patient/clientmanagement model categories of examination, evaluation, diagnosis and prognosis, intervention, and outcomes. In addition,the Professional Roles, Responsibilities, and Values were based onProfessionalism in Physical Therapy: Core Values2 as well as the 1999version of the Description of Advanced Clinical Practice (DACP)for geriatrics.3 The Knowledge Areas section was based on theDACP and A Normative Model of Physical Therapist ProfessionalEducation.4The DSP represents specialty practice, which includes all elements of practice at entry to the profession. Only the elementsconsidered to be specialty practice, either in frequency, importance, or level of judgment are included here.I. Knowledge Areas of Geriatric Clinical SpecialistsA. Foundation Sciences Biology of aging Physiology of aging Neurophysiology Anatomy Neuroanatomy Pathophysiology Cellular biology (eg, phases of soft tissue healing, tissuemakeup, changes with aging, response to exercise)B. Clinical Sciences Pharmacology Kinesiology Pathokinesiology Exercise physiology Bariatric medicine Interpretation of special tests (eg, imaging, lab values) Principles of physical therapy evaluation and treatmentof geriatric patients with musculoskeletal, neuromuscular, cardiovascular, cardiovascular/pulmonary, integumentary, or cognitive impairments Physical therapy management of healthy eldersC. Behavioral Sciences Psychology of aging Sociology of aging Economics of aging Demography4 Epidemiology of chronic diseaseElements of communicationTheories of learningPrinciples of adult educationTeaching methodologyManagement techniques and principlesPrinciples of financial managementReimbursement mechanismsPolicy issues in agingConsultant role and processRoles of interdisciplinary team membersProgram developmentEvidence-based practiceII. Professional Roles, Responsibilities, and Values of GeriatricClinical SpecialistsA. Professional BehaviorThe physical therapist practicing as a geriatric clinical specialist exhibits the following behaviors reflecting the corevalues of a professional by: Demonstrating professional behavior in interactions(eg, family meetings, written instructions, end of lifediscussions, care transitions) with patients, clients, families, caregivers, other health care providers, students,other consumers, and payers. Adhering to legal practice standards, including federal,state, and institutional regulations related to patient orclient care and fiscal management. Practicing ethical decision making that is consistentwith the American Physical Therapy Association’sProfessional Code of Ethics. Participating in peer-assessment activities (eg, performance appraisals, student evaluations, chart reviews). Demonstrating sensitivity (cultural, religious, andsocial) in professional interactions. Interacting with patients, clients, family members,other health care providers, and community-basedorganizations for the purpose of coordinating activitiesto facilitate efficient and effective patient/client care. Promoting geriatric physical therapy as an autonomouspractice. Participating in the advancement of the physical therapy profession.B. Professional DevelopmentThe physical therapist practicing as a geriatric clinical specialist demonstrates professional development by: Formulating and implementing a plan for personal andprofessional development in geriatric physical therapy,based on self-assessment and feedback from others. Enhancing knowledge and skill in geriatrics by participating in continuing professional development (eg,
Description of Specialty Practiceadvanced degrees, certification, continuing educationseminars, self study, journal clubs, residency education). Participating in gathering evidence for practice in geriatrics.C. CommunicationThe physical therapist practicing as a geriatric clinical specialist exhibits effective communication by: Using active listening. Respectfully communicating (written and oral) withpatients, clients, family, caregivers, practitioners, consumers, payers, and policy makers. Respecting cultural differences during communication.D. Social ResponsibilityThe physical therapist practicing as a geriatric clinical specialist demonstrates social responsibility by: Displaying generosity as evidenced by the use of timeand effort to meet patient or client needs. Demonstrating social responsibility, citizenship, andadvocacy including community organizations (eg,clubs, Special Olympics, Senior Olympics, ArthritisFoundation). Providing physical therapy services to underserved andunderrepresented populations to include pro bonowork.E. LeadershipThe physical therapist practicing as a geriatric clinical specialist demonstrates leadership by: Actively participating in professional organizations andactivities related to geriatric physical therapy. Maintaining current knowledge of the activities ofnational and international physical therapy organizations related to geriatrics (eg, AARP, NationalOsteoporosis Foundation, White House Council onAging, International Association of Physical TherapistsWorking with Older People). Representing physical therapy and interacting withother professionals and organizations in activities relatedto physical therapy for geriatric patients (eg, Blueprinton Aging, Fall Free Summit, AARP, American GeriatricSociety). Promoting development of and participation in clinicalresidency programs in geriatric physical therapy.F. EducationThe physical therapist practicing as a geriatric clinical specialist demonstrates ability to educate others by: Using appropriate teaching methods, and providingevidenced-based geriatric physical therapy educationalprograms to a variety of audiences including students,other health care professionals, the public, state andnationally elected officials, political groups and politicalcandidates, and third-party payers. Mentoring physical therapists, physical therapist assistants, and students by participating in clinical education and research related to geriatric physical therapy.G. AdministrationThe physical therapist practicing as a geriatric clinical specialist demonstrates administrative ability by effectively: Remaining current in reimbursement and regulatoryissues regarding public policy and delivery of servicesacross geriatric care settings. Remaining current in changes to economic drivers ofhealth care.H. ConsultationThe physical therapist practicing as a geriatric clinical specialist demonstrates consultation through: Promoting successful aging by providing information onwellness, impairment, disease, disability, and health risksrelated to age, gender, culture, and lifestyle. Providing expert consultation about geriatric issues toindividuals, businesses, educational institutions, government agencies, legal entities (eg, expert testimony), mediaoutlets, and other organizations. Meeting the needs of the geriatric patient/client throughactive involvement on multidisciplinary teams, whilerespecting each team member’s role.I. AdvocacyPhysical therapist specialists advocate for successful agingthrough direct patient care interventions, through education,through service, through research, through legislation, andthrough the development of community resources for geriatric patients/clients. Specifically, physical therapist specialistsin geriatrics: Assist geriatric patients/clients in obtaining access tohealth care and physical therapy services. Attempt to make the health care delivery system moreresponsive to the needs of geriatric patients/clients. Aid geriatric patients/clients in developing the skills toadvocate for themselves. Assist geriatric patients/clients in gaining access to allresources to assist in understanding their health conditionand managing it. Provide health promotion information to patients/clientsand the public. Disseminate evidence-based information to patients/clients, colleagues, other health care providers, and researchagencies. Seek opportunities to advocate for geriatric issues with policy and law-making bodies (eg, White House Conferenceon Aging, Long Term Care Summit, political action committees).5
Geriatric Physical TherapyJ. Evidence-based PracticeThe physical therapist practicing as a geriatric clinical specialist demonstrates evidence-based practice through: Critically evaluating new information associated with geriatric physical therapy including techniques and technology,legislation, policy, and environments related to patient/client care. Critically evaluating research findings specific to geriatricphysical therapy practice. Applying principles of evidence-based practice in geriatricphysical therapy practice (examination, evaluation, diagnosis, prognosis and intervention). Participating in collaborative or independent research tocontribute to the science associated with geriatric physicaltherapy practice. Participating in other scholarly activity that advances thepractice of geriatric physical therapy (eg, outcomes studies,literature reviews).III. Practice Expectations for Clinical Specialists in Geriatricsin the Patient/Client Management ModelA. ExaminationThe physical therapist practicing as a geriatric clinicalspecialist demonstrates examination by: History1. A systematic gathering of data from both the past andthe present related to why the patient/client is seekingthe services of the physical therapist. Obtain patienthistory through interview and data from other sources(eg, questionnaires, medical records, test results specificto geriatric patient issues) including:a) a medication interviewb) health status (eg, comorbidity, nutrition, depression, patient’s/client’s self report, family’s or caregiver’s report)c) social environment (eg, living situation, familystructure, abuse)d) functional status and activity levele) previous therapeutic efforts for this or related problems and their success or failure Systems Review1. Assess physiological and anatomical status (eg, cardiovascular/pulmonary, integumentary, musculoskeletaland neuromuscular systems).2. Appropriately examine communication affect, cognition, language, and learning style of patient/client. Tests and Measures1. Select and prioritize tests and measures based on history, systems review, scientific merit, clinical utility,and physiologic or fiscal cost to patient/client relativeto criticality of data.62. Perform tests and measures to include:a) Aerobic Capacity/Endurance Aerobic capacity during functional activities (eg,activities of daily living [ADL] scales, indexes,instrumental activities of daily living [IADL]scales, observations) Aerobic capacity during standardized exercise testprotocols (eg, ergometry, step tests, time/distancewalk/run tests, treadmill tests, oxygen titration,wheelchair tests) Cardiovascular signs and symptoms in response toincreased oxygen demand with exercise or activity,including pressures and flow; heart rate, rhythm,and sounds; oximetry; and superficial vascularresponses (eg, angina, claudication, and perceivedexertion scales; electrocardiography; observations;palpation; sphygmomanometry) Pulmonary signs and symptoms in response toincreased oxygen demand with exercise or activity,including breath and voice sounds; cyanosis; gasexchange; respiratory pattern, rate, and rhythm;and ventilatory flow, force, and volume (eg, auscultation, dyspnea and perceived exertion scales,gas analyses, observations, oximetry, palpation,pulmonary function tests) Effects of other medical and pharmacologicalinterventions on aerobic capacity/endurance (egtelemetry, pacemaker, cardiac medications)b) Arousal, Attention, and Cognition Arousal and attention (eg, adaptability tests,arousal and awareness scales, profiles, questionnaires) Cognition, including ability to process commands(eg, safety awareness checklists, management ofhome exercise program, interviews, mental statescales, observations, questionnaires) Communication and language barriers (eg, functional communication profiles, interviews, inventories, observations, questionnaires, assessment ofexpressive/receptive aphasia) Consciousness, including agitation, dementia,delirium, and coma (eg, clinical signs and symptoms, scales) Motivation and capacity to participate in intervention Orientation to time, person, place, and situation(eg, attention tests, learning profiles, mental statescales) Recall, including memory and retention (eg,assessment scales, interviews, questionnaires)c) Assistive and Adaptive DevicesThe physical therapy specialist in geriatrics performs
Description of Specialty Practicetests and measures to determine the potential benefits and use of assistive/adaptive devices based onknowledge of ADA guidelines on accessibility andbased on patient mobility and ability to performtasks. These tests and measures include: Assistive or adaptive devices and equipment useduring functional activities (eg, ADL scales, IADLscales interviews, observations) Components, alignment, fit, and ability to carefor the assistive or adaptive devices and equipment (eg, interviews, logs, observations, pressuresensing maps, patient/caregiver reports) Remediation of impairments, functional limitations, or disabilities with use of assistive or adaptive devices and equipment (eg, activity statusindexes, ADL and IADL scales, aerobic capacitytests, functional performance inventories, healthassessment questionnaires, pain scales, videographic assessments, assessments of energy conservation and energy expenditure) Safety during use of assistive or adaptive devicesand equipment (eg, diaries, fall scales, interviews,logs, observations, patient/caregiver reports) Assessment of financial resources/communityresources to assist in obtaining devices and equipment and home modificationd) Circulation (Arterial, Venous, Lymphatic) Cardiovascular signs, including heart rate, rhythm,and sounds; pressures and flow; and superficialvascular responses (eg, auscultation, electrocardiography, girth measurement, observations, palpation, sphygmomanometry, ankle/brachial index,perceived exertion scales) Cardiovascular symptoms (eg, angina, claudication) Lymphatic system function (eg, girth and volumemeasurements, palpation, observation of skin texture) Physiological responses to position change, including autonomic responses, central and peripheralpressures, heart rate and rhythm, respiratory rateand rhythm, ventilatory pattern (eg, auscultation,electrocardiography, observations, palpation, skincolor changes, sphygmomanometry, pharmacological signs and symptoms)e) Environmental, Home, and Work (PurposefulActivity) Barriers Current and potential barriers (eg, checklists,interviews, observations, questionnaires) Physical space and environment (eg, ADA compliance standards, observations, photographi
American Physical Therapy Association, 1111 North Fairfax Street, Alexandria, VA 22314-1488, 800/999-APTA (2782), www.apta.org. [Order No. E-45] A M E RI C A N B O D O F P H Y S I C A L T HERA P Y S P E C A L T I E S. Physical Therapy Description of Specialty Practice Specialty C