Transcription
Research ArticleHyperbarric Oxygen Therapy in Rehabilitation ofCerebral PalsyNorihan Abdelaziz Elgazar†, Nivine Fathy Darwish, Hanan Mohamed Elsaadany, Mervat Abd Elsatar Elsergany, BinZhaoABSTRACTObjective: To identify the efficacy of the hyperbaric oxygen therapy in rehabilitation of CP children.Methods: The study included 60 cerebral palsy patients attending the outpatient clinic of Physical Medicine, Rheumatology and RehabilitationTanta University Hospital. They were assessed and divided into two groups: Group 1: (30 patients) referred to Hyperbaric Medical Institutionin Tanta university hospital to receive HBOT 40 sessions, in addition to their conventional rehabilitation program for six months. Group 2:(30 patients) received their conventional rehabilitation program only in the form of sessions of physical therapy three times per week for thetreatment period (six months).Results: Our study showed insignificant difference between 2 studied groups at 3 and 6 months in relation to gross and fine movement andreduction of spasticity.Conclusion: HBOT of minor role in improving motor delay and disabilities of CP and physical therapy is still the 1st line of rehabilitation inCP children.Keywords: HBOT; Rehabilation; Oxygen therapyIntroductionCP is a static encephalopathy which means braininjury that is non-progressive disorder of postureand movement of variable etiologies that maybeassociated with epilepsy, speech problems, visioncompromise and cognitive dysfunction [1,2].CP is caused by damage to the motor controlcenters of the developing brain and can occurduring pregnancy, childbirth or after birth up tothree years. The incidence of CP increases withpremature or very low-weight babies regardlessof the quality of care [3-6].Many impairments of sensation, perception,cognition, communication, behavioral problems,epilepsy, difficulties with sleeping, drooling andfeeding accompany motor disorders in CP andrequire medical management. Therefore, healthcare for children with CP requires the skills ofvariety of professions who must work efficientlyand collaboratively with the family as team.The goal of rehabilitation is to gain independencein activities of daily living school or work andsocial life. Child rehabilitation aimed to improvemobility, prevent deformity and educate theparents about the child’s problem. It also involveshelping the child to learn the skills he will needin daily life in school and while playing withfriends. Lastly rehabilitation means decreasingthe complications which arise as a result of thechild’s neuro-muscular impairments.Rehabilitation of CP children include traditionalphysiotherapy as electrotherapy, hydrotherapy,heat therapy, massage, therapeutic exercises,stretching exercises and functional therapyas hippo therapy and vojta technique whichprescribed to prevent contractures and tostrengthen the weak muscles to enable functionalPhysical Medicine, Rheumatology and Rehabilitation, Assiut University, EgyptAuthor for correspondence: Norihan Abdelaziz Elgazar, Physical Medicine, Rheumatology and Rehabilitation, Medicine, AssiutUniversity, Egypt, E-mail: wafaagad2015@gmail.com†IJOCS.1000164 2021International Journal of Clinical Skills (2021) 15(2), 377-384ISSN 1753-0431377
Research ArticleElgazar NA, Darwish NF, Elsaadany HM, Elsergany MAE, Zhao Buse of the upper extremity and to establish a betterwalking pattern. Also the current rehabilitationprograms of CP start using hyperbaric oxygenin addition to other rehabilitation programsbecause some clinical trials of using HyperbaricOxygen Therapy (HBOT) in CP have reportedsignificant improvement in study groups [7,8]. Treatment was once/day, 5 days/week for 40sessions Group 2HBOT involves inhaling 100% oxygen atgreater than one Atmosphere Absolute (ATA)in a pressurized chamber. HBOT has been usedsuccessfully in humans at varying pressuresto treat a range of conditions. Many clinicalapplications of HBOT are including treatmentof decompression sickness, arterial gas embolism,carbon monoxide poisoning, amyotrophic lateralsclerosis, and complex regional pain syndrome.However, HBOT has also been used at lowerpressures (1.5 ATA or less) with clinical successin conditions including ischemic brain injuryand CP [8].(30 patients) received their conventionalrehabilitation program only in the form ofsessions of physical therapy three times per weekfor the treatment period (six months).Therapeutic effects of HBOT in CP are due toan increase in dissolved oxygen in plasma andtissue that help tissue to regenerate which used totreat CP under the theory that improving oxygenavailability to damaged brain cells can reactivatesome of them to function normally but Its use totreat CP is controversial [8-10]. Stretching of tendoachilisMaterial and Methods CP children with age group up to 5 yearsThe study included 60 cerebral palsy patientsattending the outpatient clinic of PhysicalMedicine, Rheumatology and RehabilitationTanta University Hospital. They were assessedand divided into two groups: CP children with negative family history ofdegenerative brain insults Group 1(30 patients) referred to Hyperbaric MedicalInstitution in Tanta university hospital toreceive HBOT sessions, in addition to theirconventional rehabilitation program for sixmonths. (Hyperbaric oxygen therapy wasperformed in mono chamber hyperbaricchamber from SECHRIST Company Para medmade in USA) [11].378 Total oxygen breathing time is 60 minuteswith 5 minutes’ air break after 30 minutes’oxygen breathingPhysical therapy and rehabilitation program thatwas done in both groups using different typesof physical modalities 3 times per each week inaddition to exercises at home.Physical modalities in the form of Excersise (active, assisted active or passive) Massage to limbs affected Heat therapy in the form of infrared rays, hotpacks [12] Inclusion criteria CP diagnosed according to Scientificneurological examination to early detect delayin developmental mile stones CP children with absent any deformities ofany other musculoskeletal diseases Exclusion criteria Patients not fit for hyperbaric oxygen therapyas Patients with active epilepsy and recurrentseizers Patients with tension pneumothorax Patients with uncontrolled heart failure Eustachian tube dysfunction Patients was compressed and decompressed at2-3 psi/minute (pounds per square inch) withair, the rate depending on patient comfortand tolerance Patient with rupture ear drum Depth of pressurization with 1.5 AbsoluteAtmosphere ATA CP children with positive family history ofdegenerative brain insultsInternational Journal of Clinical Skills (2021) 15(2) Patient on mechanical ventilation Children of CP aged more than 5 years
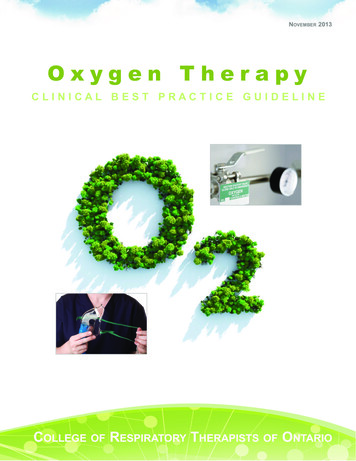
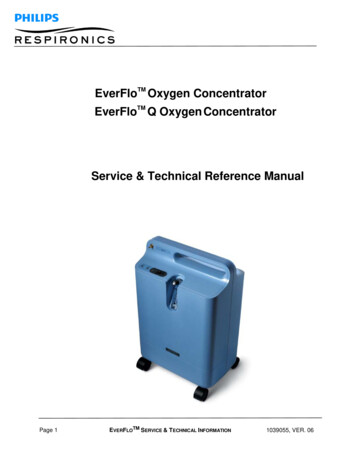
Hyperbarric Oxygen Therapy in Rehabilitation of Cerebral Palsy Children with other deformities of anyother musculoskeletal diseases that limitsmovements Children with behavioral problemscase before 3 years that predispose to CP[13,14] Family history to exclude any case of positivefamily history of congenital brain diseases Children who were treated with botulinumtoxin or orthopedic surgery within the past 6month or dorsal rhizotomy within the past 2years Consanguinity of parents of patient Deaf and blind childrenResults All Patients will be assessed byThe following data was determined for eachpatient at time of start of the study. Completehistory taking from parents or child caregiver byasking them about Clinical examination: At start of study, 3months later and at the end of the studyOur study showed insignificant differencebetween 2 studied groups at 3 and 6 monthsin relation to gross and fine movement andreduction of spasticity. Natal history: Type of delivery to detect anydelay of labor causing insufficient oxygensupply to brain of babyAll children in both groups were assessed inGMFCS according to their ages. There wasinsignificant difference between both groupsbefore treatment, 3 months and 6 monthsof study according to GMFCS. There wasimprovement in both groups at 3 and 6 monthsfollow up compared to before treatment but thisimprovement was statistically insignificant withmore improvement in group 1 (Table 1 andFigure 1). Post-natal history: Accident or infection of6 months according to Gurdon and Duff at 3 Demographic data: (name-age-sex) Past history: as epilepsy, asthma, etc Prenatal history: To detect any abnormalitiesduring pregnancy period that predispose toCPResearch ArticleTable 1: Functional assessment of both studied groups (according to GMFCS) at the start of the study, 3 and 6 monthsfollow up.GroupsChi-square testGMFCSGroup IGroup 7Before4413.33413.35723.331033.3After 3 MonthsAfter 6 10.39533.31.0000.317-FrX22.0001.000p-valueFrX20. 1570.3173.0001.000p-value0.0830.317379
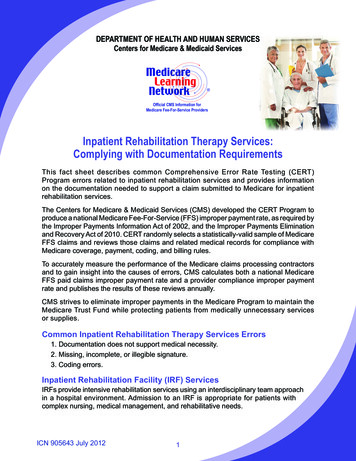
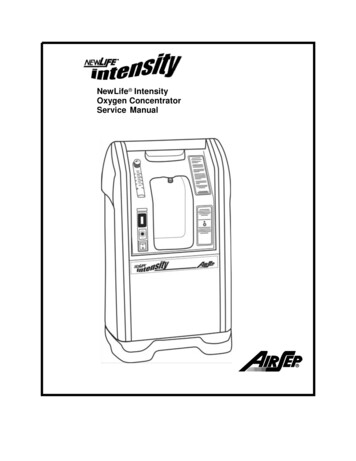
Research ArticleElgazar NA, Darwish NF, Elsaadany HM, Elsergany MAE, Zhao Band 6 months follow up compared to beforetreatment but this improvement was statisticallyinsignificant with more improvement in group 1(Table 2 and Figure 2).Figure 1: GMFCS in both studied group.Table 2: Functional assessment of upper limbs of both studied groups at the start of the study, 3 and 6 months followup (Gurdon and Duff assessment of hand).GroupsChi-square testGurdon and Duff assessment of handGroup IGroup II2p-valueXn%n%BeforeAfter 3 MonthsAfter 6 alue0.0830.157International Journal of Clinical Skills (2021) 15(2)0.5880.9640.5710.9660.9500.917
Hyperbarric Oxygen Therapy in Rehabilitation of Cerebral PalsyResearch ArticleFigure 2: Gurdon and duff assessment of hands in both studied group.Table 3: Modified Ashworth’s scale of both groups at the start of the study, 3 and 6 months follow up in both studiedgroups.GroupsChi-square testGroup IGroup IIModified Ashworthp-valueX2n%n%01BeforeAfter 3 MonthsAfter 6 -valueFrX20.3170.3172.001.00p-value0.1570.317381
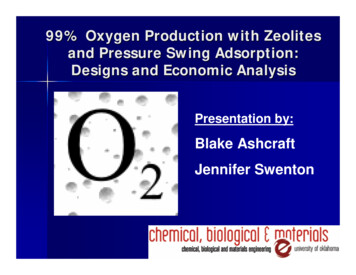
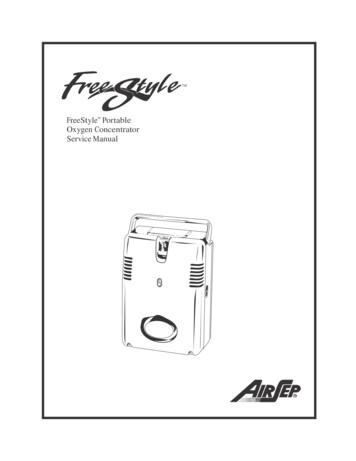
Research ArticleElgazar NA, Darwish NF, Elsaadany HM, Elsergany MAE, Zhao BFigure 3: Modified ashworth scale in both studied groups.There was insignificant difference between bothgroups before treatment,3 months and 6 monthsaccording to MAS. There was improvementin both groups at 3 and 6 months followup compared to before treatment but thisimprovement was statistically insignificant withmore improvement in group 1 (Table 3 andFigure 3).and hyperbaric pressure leads to improvementin tissue oxygenation and affects both oxygensensitive and pressure-sensitive genes. HBO2therapy can initiate vascular repair and improvecerebral vascular flow, induce regeneration ofaxonal white matter, stimulate axonal growth,promote blood-brain barrier integrity and reduceinflammatory reactions as well as brain edema[21].DiscusionAccording to fine motor assessment thatmeasured via Gurdon and Duff assessment thatwas done to assess hand function to allow doctorsto follow the improvement of hand function ofCP, there was insignificant difference between 2studied groups at start of the study.In relation to gross motor function followup of both groups at 3 and 6 months, therewas improvement occur at 3 and 6 monthscompared to the start of treatment in bothgroups with insignificant difference between the2 groups [15-17] but slightly better in group 1suggesting that the role of HBOT in improvingmotor function of CP after 40 sessions is of nosignificant importance as the result of study ofWaalkes et al. [18] that was designed to assessthe effect of HBOT as an adjuvant therapy inCP showing non-significant improvements inmotor function and spasticity and observedthat mild improvements were placebo effectsand therefore, HBOT therapy had no neurotherapeutic effects on TBI and CP also as theresult of Lacey et al. [19] that is against usingHBOT in rehabilitation of CP but this is againstthe result of Sethi et al. [20] which concludedthat HBOT associated with occupational therapyand physiotherapy is effective in improving themotor skills of children with CP that can beexplained that The combined action of hypoxia382In relation to hand function assessment at 3 and6 months’ follow-up, no significant differencebetween improvement in both studied groups asthe result of the study of Waalkes et al. [18] thatsuggest that by observing children at sessions ofHBOT there was no effect of it in improving finemovement by hands.Also our result can be explained by short timereceiving sessions of HBOT as there are debateabout minimum and maximum duration toreceive HBOT in CP as weeks to months arenecessary for brain tissue regeneration andangiogenesis, but the upper time limit fromwhich no further improvements are expectedremains unknown.International Journal of Clinical Skills (2021) 15(2)
Hyperbarric Oxygen Therapy in Rehabilitation of Cerebral PalsyResearch ArticleConclusionConflict of InterestPhysical therapy is still the first line ofrehabilitation in CP that must be started asearly as possible to improve gross and fine motordysfunction. HBOT of minor role in improvingmotor delay and disabilities of CP.There is no actual or potential conflict of interestin relation to this article.383
Research ArticleElgazar NA, Darwish NF, Elsaadany HM, Elsergany MAE, Zhao BReferencesmedical institute. Pediatrics 102, e53 (1998).1. Jindal P, Rosenbaum P, Direzze B, et al.Treatment and rehabilitation of childrenwith cerebral palsy in India. Dev Med ChildNeuro 61, 1050-1060 (2019).2. Adam T, Juan C, Mark P, et al. Symptomsburden in individuals with cerebral palsy. JRehabil Res Dev 47, 863-867 (2010).3. Hiltz D, Thurman J, Gwinn-I-lardy K, et al.How common are the n common neurologicdisorders? Neurology 68, 326-337 (2007).4. Ferrari A, Cioni G. The spastic forms ofcerebral palsy: A guide to the assessmentof adaptive functions. ASJC Italy 88, 3-15(2010).5. Tommiska V, Heinonen K, Lehtonen L, et al.No improvement in outcome of extremelylow birth weight infant population between1996-1997 and 1999-2000. J Paediatrics 19,29-36 (2007).6. Svraka E, Loga S, Brown I. Family quality oflife: Adult school children with intellectualdisabilities in Bosina and Herzegovina. JIntellect Disabil Res 55, 365-388 (2011).9. Hadanny A, Abbott S, Efrati S, et al. Effectof hyperbaric oxygen therapy on chronicneurocognitive deficits of posttraumaticbrain injury patients: Retrospective analysis.BMJ 8, 23387 (2018).10. Raelina S, Theresa C, Woods M, et al.Hyperbaric oxygen therapy: Indications,contraindications, and use at a tertiary carecenter. Aorn J 107, 443-450 (2018).11. Butler C, Campbell S. Evidence of the effectsof intrathecal baclofen for spastic anddystonic cerebral palsy AACPDM treatmentoutcomes committee review panel. DevMed Child Neurol 42, 34-45 (2000).12. McDonagh M, Morgan D, Carson S, et al.Systematic review of hyperbaric oxygentherapy for cerebral palsy: The state of theevidence. Dev Med Child Neurol 49, 942-947(2007).13. Farmer J, Sabbagh A. Selective dorsalrhizotomies in the treatment of spasticityrelated to cerebral palsy. Child Nerv Sys 23,991-1002 (2007).7. Gabb G, Robin ED. Hyperbaric oxygen: Atherapy in search of diseases. J Chest 92,1074-1082 (1987).14. Gretl l, Rocky f, Ernest S, et al. Hyperbaricoxygen therapy: Exploring the clinicalevidence advances in skin and wound care.Adv Skin Wound Care 107, 442-453 (2017).8. Waisman D, Shupak A, Melamed Y, et al.Hyperbaric oxygen therapy in the pediatricpatient. The experience of the israel naval15. Hanft B, Pilkington K. Therapy in naturalenvironments: The means or end goal forearly intervention? Infants Young Child 12,384International Journal of Clinical Skills (2021) 15(2)1-13 (2000).16. Azhar M, Zareen A, Saleem Z, et al.Evaluation of role of hyperbaric oxygentherapy in children with cerebral palsy: Ourexperience at armed forces hospital, KingAbdul Aziz naval base, KSA. Paediatrics J 11,1407-1411 (2017).17. Wang Y, Zhu Y, Qiu B, et al. Study on theeffectiveness of hyperbaric oxygen nursingand treatment for children with cerebralpalsy. Acta Medica Mediterranea J 35,657:660 (2019).18. Waalkes P, Fitzpatrick DT, Stankus S, et al.Adjunctive HBO treatment of children withcerebral anoxic injury. US Army Med Dep J13-21 (2002).19. Lacey D, Stolfi A, Pilati L. Effects of hyperbaricoxygen on motor function in children withcerebral palsy. Ann Neurol 72, 695-703(2012).20. Sethi A, Mukherjee A. To see the efficacyof hyperbaric oxygen therapy in grossmotor abilities of cerebral palsy childrenof 2-5 years, given initially as an adjunct tooccupational therapy. Indian Occup J 1, 7-12(2003).21. Carole S, Serge L, Pierre M, et al. Hyperbaricoxygenation therapy in treatment ofcerebral palsy: A review and comparisonto currently accepted therapies. J of AmerPhysi and Surg 12, 109-113 (2007).
sessions of physical therapy three times per week for the treatment period (six months). Physical therapy and rehabilitation program that was done in both groups using different types of physical modalities 3 times per each week in addition to exercises at home. Physical modalities in the form of Excersise (active, assisted active or passive)