Transcription
Women’sHealth PlanA plan for 2021-2024Women’s Health Plan A Plan for 2021-241
ContentsForeword by the Minister for Public Health,Women’s Health and Sport4Introduction by the Chair of the Women’s HealthGroup61 Why we need a Women’s Health Plan82 Women in Scotland today113 Our ambition124 Principles underpinningthe Women’s Health Plan134.1 Addressing inequalities144.3 Gender equality and intersectionality194.2 Life course approach4.4 Respectful and inclusive services5 Strategic context1520225.1 National Performance Framework225.3 Pregnancy and Maternity235.2 Other policies5.4 Screening5.5 Mental health6 Priorities7 Our approach7.1 Women’s Health Group7.2 Sub-groups8 Context2323Women’s Health Plan A Plan for 2021-249.4 Heart health9.5 Gender and health9.6 Lived experience10 How will we make change happen and whoneeds to be involved?10.1 Creating the conditions for change10.2 Who needs to be involved11 Conclusion3841434546464649ANNEX A - List of those involved50ANNEX C - Legal framework53ANNEX E - Library of resources and endnotes59ANNEX B - Strategic context: policy documents 52ANNEX D - Glossary of terms and acronyms54262627288.6 Heart health9.3 M enopause, menstrual health includingendometriosis35268.3 Menstrual health8.5 Menopause9.2 C ontraception, abortion, sexual healthand pre-pregnancy3425278.4 Endometriosis9.1 Actions which cut across all priority areas33248.1 Access to information and services8.2 Sexual health, contraception and abortion9 Priorities, aims and actions282929313
Foreword by theMinister for PublicHealth, Women’sHealth and SportI am proud to present theScottish Government’sWomen’s Health Plan. I believethat our vision for Women’sHealth is an ambitious one –and rightly so. Women’s healthis not just a women’s issue.When women and girls aresupported to lead healthy livesand fulfil their potential, thewhole of society benefits.In our debate on Women’s Health I quoted fromCaroline Criado Perez’s thought-provoking book‘Invisible Women’ and I wish to do the same here atthe beginning of our Women’s Health Plan, as shesays so much in the few words: ‘women are not, tostate the obvious, just men.’She goes on to explain: ‘Historically, it has beenassumed that there wasn’t anything fundamentallydifferent between male and female bodies otherthan size and reproductive function, and so, foryears, medical education has been focussed on themale “norm”, with everything that falls outside thatdesignated as “atypical” or even “abnormal”.’ Thishas to change. Women are not atypical – they are51% of Scotland’s population.Whilst we know that across Scotland there areexamples of excellent and innovative services forwomen there is a clear need for wider systemicchange to ensure that all our health and social careservices meet the needs of all women, everywhere.Together, we are working to address the inequalitiesin all aspects of health that women are facing. TheWomen’s Health Plan focusses on specific priorityareas where a need for improvement was identified.But the Plan is one part of a much wider picturewhen it comes to women’s health and wellbeing.The Scottish Government is committed to a rangeof actions to improve women’s health. The mentalhealth of women and girls is a priority within theMental Health Transition and Recovery Plan. WeWomen’s Health Plan A Plan for 2021-24have taken decisive action in relation to mesh,including halting its use in 2018, and we will pursuethe outcomes set out in the Mesh Survivors’ Charter.Cancer screening remains a priority and we willcontinue to deliver our Screening Inequalities Fundto tackle inequalities in the national populationscreening programmes, setting aside 2 million overthe next two years to tackle inequalities includingthose that have arisen as a result of COVID-19.We are continuing to implement our Recovery andRedesign: Cancer Services Action Plan. We aretackling violence against women and girls throughthe implementation of our Equally Safe Strategy. TheGender Pay Gap Action Plan is driving forward thechanges needed to reduce the gender pay gap foremployees in Scotland.Additionally, the Government’s 2021 Manifesto madea range of new proposals in relation to women’shealth. Work is underway now to develop newactions connected to these proposals. So, while theyare not addressed in this iteration of the Women’sHealth Plan, they will be progressed by the ScottishGovernment during this parliamentary term.This includes new action in relation to: establishing a dignified and compassionatemiscarriage service tailored to the needs ofwomen; the provision of paid leave for miscarriage andstillbirth, delivering this within the public sectorand calling on the UK Government to make thenecessary changes to employment law to make itavailable for everyone; a review of midwifery and health visitingpathways; unexpected pregnancy complications; age thresholds for Screening; and the establishment of a Scottish Institute forWomen’s Health.4
The work on the Women’s Health Plan beganbefore the pandemic – and the evidence wasalready stark about the inequalities impactingwomen’s health and the need for decisive action toaddress them. But Covid-19 shone an even brighterlight on these inequalities.Women have been even more adversely impactedby the Covid-19 pandemic. Inequalities havebeen exposed and exacerbated. The challengesof balancing childcare, paid work and caringresponsibilities with the stresses and uncertaintiesof the pandemic have been truly daunting for manywomen, and have undoubtedly affected their health.Learning from the pandemic – the needs of women,and its impact on services – has been central.Changes in service delivery have also highlightedpositive opportunities for change and these havebeen brought into the Plan.As Minister for Women’s Health, I am ambitious forwomen in Scotland. I am determined that we drivechange in women’s health. This, our first Women’sHealth Plan, signals this ambition and determinationthat we see change for women in Scotland, for theirhealth and for their role in society. We can be WorldLeaders in Women’s Health – starting here andnow.Maree Todd, MSPMinister for Public Health, Women’s Health andSportBut we know that the inequality women facethroughout their lives existed before Covid. For toolong women have been disadvantaged, and thishas impacted their right to health. It is time thatthis disadvantage is addressed and the inequalitythat women experience in relation to their health iseradicated.For example, when we provide high-qualityinformation and education on menstrual health,young women and girls are empowered tounderstand what is ‘normal’ and when they needto ask for help. When women are well informedand supported about the menopause, they canmake informed choices about what they need, inhealthcare, in the workplace and beyond. Whenresearch includes women, medicine can becomemore equitable. When we understand that hearthealth does not manifest ‘abnormally’ in women, wecan save lives. When women’s needs are taken intoaccount, we all flourish.Women’s Health is not only about reproductivehealth. Our Women’s Health Plan aims to reduceavoidable health inequalities for women and girlsacross the course of their lives – from puberty tothe later years – focussing on those areas that arestigmatised, disregarded or dismissed as ‘women’sproblems’. By supporting health in women and girlswe can expand their choices and opportunities toachieve their potential.Central to the development of the Plan have beenwomen’s voices. It is vital that women continueto inform their health and the health of women inScotland – I look forward to hearing from themas we implement the Plan and drive forwardimprovement.Women’s Health Plan A Plan for 2021-245
Introduction by theChair of the Women’sHealth GroupThe themes of Realistic Medicine resonatethroughout this Women’s Health Plan. One ofthe themes that emerged strongly from our livedexperience work was that women wish to takean active role in decisions around their health.Shared decision-making means ensuring womenhave access to accurate and relevant informationas well as being proactive in including women indiscussions about their health and healthcare.Women also want a personalised approach to‘Women’s health’ can be traditionally thought oftheir care, recognising that one model will not worksolely in terms of reproductive health, despite thefor all women. For example, women experiencefact that slightly more than half of the populationthe menopause in a variety of ways. For mostaccessing healthcare are actually women. Therewomen, their GP and the primary care team willare excellent examples of first-class care andbe able to support them where required throughinnovative approaches to improving the health oftheir menopausal years. However, some womenwomen. But undertaking the work to produce thiswill require more specialised support and will needPlan has brought into sharp focus the way thatonward referral. Healthcare professionals mustwomen and their health needs are not necessarilywork with women to understand their individualconsidered as different to men within our healthservices, and how our services can be failing to fully circumstances, health needs and preferencesin order that personalised and tailored care ismeet the needs of women. The lack of inclusion ofprovided. Finally, Realistic Medicine calls on uswomen in medical research, which then impactsall to be ‘improvers and innovators’. In order toon the availability and efficacy of treatments forimprove care for women we must work acrosswomen, is a very tangible example and illustrationof how we have not done enough to date to ensure sectors and organisations and look at innovativeways in which healthcare can be provided.services equally recognise and meet the needs ofCovid-19 has introduced and accelerated many ofwomen.these innovations, for example in the provision ofvirtual abortion care, but there is far more work toWhilst this Plan focusses on how changes inbe done.healthcare can improve the health of women, itis, of course, far from the full story. As a publicI would like to extend my very sincere thankshealth doctor, the importance of the social andto all the people involved in the developmenteconomic determinants of health, and the wayand creation of this Plan. Firstly, to Dr Catherinethey can disproportionately impact on womenCalderwood, former CMO, who had the vision tois very much on my mind. The factors whichset this work in motion. Secondly to the members ofimpact on a woman’s health stretch far beyondthe Women’s Health Group, particularly Vice Chairhealthcare services and include educationalopportunities, employment options, housing, caring Corinne Love, and the sub-group chairs AlisonScott, Heather Currie, Maggie Simpson, Ireneresponsibilities and income.Oldfather and the late Emma Ritch. I also want topay tribute here to Emma Ritch who representedWhilst outside the scope of this Plan, the verythe First Minister’s National Advisory Council onsignificant impact of social and economicdeterminants of health on women in particular must Women and Girls on our Women’s Health Group,and chaired the Gender and Health sub-group.be fully recognised.Emma was a tireless campaigner for women’sIt has been a great privilege to lead on thedevelopment of the Women’s Health Plan – as awoman, as a doctor, and as Interim Deputy ChiefMedical Officer for Scotland. Contributing not justto ensuring we support the best possible healthoutcomes for women, but also to ensuring all girlsand women of Scotland are able to reach their fullpotential is very close to my heart.Women’s Health Plan A Plan for 2021-246
equality and in her contribution to the developmentof this Plan she challenged us all to think differently.Her recent death leaves a huge void in thewomen’s equality movement, but where she ledwe must now follow. And finally, thank you to thewomen of Scotland who engaged with our livedexperience work. It is so crucial that the work toimprove the health of women in Scotland is drivenby the needs and wishes of women themselves.This Plan represents only the beginning of the workto address the inequalities that impact on women’shealth. It illustrates that we have some way togo in adequately shifting our focus to women’shealth, and that will need commitment, leadershipand effort from all those who provide services towomen. My ask of my fellow health and social careprofessionals is to think about how you specificallyconsider women in the design and delivery ofyour services, to ensure that the different waysdiseases can manifest in women, and the differenttreatments that might be appropriate for them arefully considered, to appreciate and understand thesystemic barriers women may face when seekinghealthcare and to play your role in breaking thesebarriers down. There is much work to be done but Iam more than confident that we have the skills andthe will to do this. Working together, we can and willimprove women’s health in Scotland.Professor Marion BainInterim Deputy Chief Medical Officer forScotlandWomen’s Health Plan A Plan for 2021-247
1Why we need aWomen’s Health PlanThe aim of this Plan is to improve healthoutcomes and health services for all womenand girls in Scotland. It is underpinned by theacknowledgement that women face particularhealth inequalities and, in some cases,disadvantages because they are women.Health is a state of complete physical,mental and social wellbeing and notmerely the absence of disease orinfirmity.World Health Organisation (WHO).A range of biological factors impact on women’shealth. Women and girls experience various healthneeds and risks during their lives which are not thesame as those of men. This may relate to startingand managing periods, choosing contraception,accessing abortion services, planning forpregnancy, managing menopause symptoms andthe manifestation of chronic conditions such asheart disease.In its 2019 publication ‘Better for Women’ theRoyal College of Obstetricians and Gynaecologists(RCOG) highlighted some of the unmet needs ofwomen in the UK and concluded that too manywomen are struggling to access basic healthcareand, when they do, health services too often missopportunities to ask the right questions, optimisethe resources available to prevent illness andensure the best outcomes.According to a British Heart Foundation Report, inScotland there are inequalities at every stage of awoman’s medical journey2.There is also considerable evidence of womenbeing undertreated or presenting disease in adifferent way to men. However, there is a significantdata gap in medical research which furthercontributes to health inequalities in the UK. Womenmake up 51.5% of Scotland’s population3 and yetwomen are less likely to be invited to, or participatein, medical trials and research.4 There is a historic,and ongoing, failure to include sex and genderdifferences in the design, delivery and analysis ofclinical research studies. A 2016 Oxford Universityreport5 highlights this issue, stating that for manyyears it was widely assumed that the occurrenceand outcomes of disease were the same for menand women, and that our understanding of diseaseprocesses based on studies involving only menwould be equally relevant for women. An increasingbody of evidence suggests that this is not the case,and that we can improve our knowledge aboutdisease occurrence and disease outcomes – forboth men and women – by undertaking analyses ofhealth data disaggregated by sex and informed by agender perspective, as well as by including sufficientnumbers of women in scientific studies6.This document will use the term‘women’/‘woman’ throughout. It isimportant to highlight that it is not onlythose who identify as women whorequire access to women’s health andreproductive services. For example,some transgender men, non-binarypeople, and intersex people or peoplewith variations in sex characteristicsmay also experience menstrualcycles, pregnancy, endometriosisand the menopause. The actionsincluded within this Plan make clearthat all healthcare services should berespectful and responsive to individualneeds.This is not just about differences in reproductivehealth: various studies have shown that women donot always receive equal healthcare to men andthat outcomes for women are poorer than those formen. For example, when it comes to heart health,women are less likely than men to be prescribeddrugs that reduce the chance of a second heartattack and women are less likely to receivediagnostic testing, such as coronary angiographyimaging, within 72 hours of hospital admission1.Women’s Health Plan A Plan for 2021-248
In the UK one in three women will experience areproductive or gynaecological health problem atsome point in their lives7. Despite this in 2018 just2.1%8 of publicly funded research spend wasdedicated solely to reproductive health and childbirth,a reduction from 2.5% in 20149. Endometriosisaffects around 10% of women and girls globally, it istherefore estimated that one in ten women inScotland have endometriosis10. Despite this highprevalence, the average time to diagnosis from onsetof symptoms in Scotland is 8.5 years11. Althoughendometriosis is as common in women as diabetesand asthma, it has failed to attract the sameattention, support and funding as those diseases12.Simply put, we know less about how best to treatdiseases in women.Research suggests that patients’health outcomes can be related tothe gender of who they are treatedby. For example a study, publishedin 2021, suggested that that genderconcordance (when a female doctortreats a female patient) increases awomen’s access to treatments andspecifically that gender concordancereduced the risk of death following aheart attack.Does Patient-Physician GenderConcordance Influence PatientPerceptions or Outcomes?Inequities are also faced by the health andsocial care workforce. Women make up the vastmajority of the NHS workforce and whilst in thepast ten years the proportion of female doctorsand consultants has increased13, patterns ofoccupational segregation remain, with womensignificantly under-represented in areas such ascardiology and surgery. Women’s health is alsoimpacted by various social factors, including wherethey are born, their age, their ethnicity, their sexualorientation and much more.young people14. Between 2017 and 2020 thepoverty rate in Scotland was highest for singlewomen with children and 20% of single femalepensioners were living in relative poverty15. Being inemployment is not necessarily protective againstpoverty and women are more likely to be in workingpoverty than men16. Women are heavily overrepresented in occupations which tend to be lowerpaid and undervalued compared to those which aremale dominated17. Living in poverty is known to bedamaging for health and one of the main causes ofpoor health and health inequalities18. Public HealthScotland note that gender-based violence (GBV) isa major public health, equality and human rightsissue and is experienced unequally, with 17% ofwomen and 7% of men having experienced the useof force from a partner or ex-partner at some pointin their lives19. The latest annual data for Scotlandshows that 82% of domestic abuse incidentsreported had a female victim and maleperpetrator20. 20% of women have experiencedsexual abuse before the age of 1821.The Scottish Government is committed totackling poverty, addressing the Gender PayGap and the eradication of male violenceagainst women and girls. Significant workis being undertaken across the ScottishGovernment, the public and third sectors toaddress these major societal issues (seesection 5). While the primary focus of thisPlan is on the reduction in inequalities inhealth outcomes and the improvement ofhealth services for women, it is vital that thewider determinants of health are considered(see section 4).All of this adds to avoidable health inequalities forwomen.It is important to consider and understand theconditions in which women live, as this significantlyimpacts overall health and women’s ability toaccess healthcare services. For example, the riskof poverty is much higher for women, disabledpeople, minority ethnic people, lone parents (themajority of whom are women) and children andIt is also clear that the impacts of the Covid-19pandemic have not been felt equally across thepopulation and that the most negative impactsfall on those least able to withstand them22. Themajority of unpaid carers are women, womenmake up the majority of the health and social careworkforce, the vast majority of lone parents arewomen23 and women are more likely to be victimsof domestic abuse24. Research conducted byClose the Gap suggests that Covid-19 has had adisproportionate impact on women, particularly inthe area of employment25. In Scotland, women haveaccounted for the majority of furloughed staff sinceJuly 202026. According to the Institute for FiscalStudies mothers are more likely to have quit orlost their job, or to have been furloughed, since thestart of the lockdown27. The challenges of balancingchildcare, paid work, caring responsibilitiesalongside managing the stresses and uncertaintiesWomen’s Health Plan A Plan for 2021-24Some NHS boards are involved withthe Equally Safe at Work accreditationprogramme. The programme supportsemployers to improve their employmentpractice to advance gender equality at workand prevent violence against women.9
of the pandemic should not be underestimated,particularly how this has, and continues, to impactwomen’s health.Another aspect of inequality that hasbeen particularly prominent has been thedisproportionate impact on minority ethnic people.The reasons for this are complex and include theinterplay between socio-economic disadvantage,high prevalence of chronic diseases and the impactof long-standing racial inequalities. To addressthese issues an Expert Reference Group onCovid-19 and Ethnicity was established to provideadvice and recommendations to the ScottishGovernment. The Women’s Health Plan has notspecifically investigated the impact of Covid-19on women and women’s health, but presentsin some of its proposed actions opportunities tofocus on groups of women who may have beendisproportionately affected by the pandemic.The Covid-19 pandemic has also createdopportunities to implement new ways of providingpatient care, particularly in respect of the provisionof contraception and the delivery of abortion care.A number of the new and innovative ways ofworking have developed quickly in response to thepandemic and are captured in this Plan for longerterm implementation.We have an opportunity to address theseinequalities. That is why we have developed thisWomen’s Health Plan to focus on the specifichealth needs of the women of Scotland.This Women’s Health Plan sets out how theScottish Government intends to reduce inequalitiesin health outcomes affecting women over the nextthree years, and beyond.We need to be careful to avoid biasin how patients are diagnosed andtreated. Women and men shouldhave an equal chance of receiving thecorrect diagnosis and treatment. Thisis work in progress.Professor Colin Berry, Professor ofCardiology and Imaging (Institute ofCardiovascular & Medical Sciences)Women’s Health Plan A Plan for 2021-2410
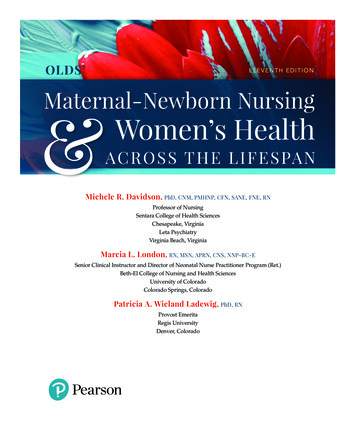
2Women inScotland todayAround 400,000women in Scotlandare of menopausal ageIt is estimated thatendometriosis affects1.5 million (1 in ten)women in the UK ofreproductive age, andit takes an average of8.5 years to diagnose.Women’s lifeexpectancy at birthin the most deprivedareas is 75.6 years,compared to 85.6years in the leastdeprived areas.In 2020, 13,815terminations ofpregnancy wererecorded in Scotland(13.4 per 1000 womenaged 15-44)Heart disease isthe leading causeof maternal deathin the UK⅓In Scotlandover a thirdof the femaleworkforce is over 5061%Average lifeexpectancy atbirth for a woman inScotland is 81.1 yearsIn 2020 therewere 46,809live births inScotlandof unpaid carersare womenIn the most affluent areas of Scotland,women experience 25.1 more years of goodhealth compared to the most deprived areas.51%of Scotland’spopulationare womenIn 2019-20 around400 women were inprison in Scotlandon an average day37% of women inScotland report livingwith a limitinglong-term conditionor disabilityIn 2020 the terminationrate was 2.2 timeshigher in the mostdeprived areascompared to theleast deprived areasPart-time employmentaccounts for 41.2 %of all women’semployment comparedwith 12.4% of allmen’s employmentWomen’s Health Plan A Plan for 2021-24In 2020 63% ofwomen in Scotlandwere between 16and 64, and 21%were 65 and over.Almost 1 in 10 deathsin women in Scotlandeach year are causedby ischaemicheart diseaseIn 20191.35 millionwomen inScotland werein employmentIn Scotland, womenaged under 25 arethe group most at riskof being diagnosedwith an STI.Over threequartersof the overallNHSScotlandworkforceare womenThe average age atwhich a woman willreach menopauseis 51Women make up an estimated 83%of the social care workforce in ScotlandTwelveis the average age at whicha woman has her first periodDeath from stroke is more commonfor women than menOn average, thelife expectancyof women with alearning disability is18 years shorterthan for women in thegeneral populationIt is estimated that thereare currently 300,000people in Scotlandliving with osteoporosis,a condition which ismore common inwomen than men11
3Our ambitionOur ambition is for a Scotland where healthoutcomes are equitable across the population,so that all women enjoy the best possible healththroughout their lives.Healthcare forwomen will be holistic,inclusive, respectful,centred around theindividual and responsiveto their needs and choices.Women will be providedwith consistent, reliable andaccessible informationempowering them to makeinformed decisions abouttheir health andhealthcare.All professionals involvedin delivering health and socialcare services will work closelytogether to improve carefor women.Healthcare for women withcomplex needs, including thosewith additional social supportrequirements, will be deliveredinnovatively, including jointlywith third sector supportwhere appropriate.Women’s Health Plan A Plan for 2021-2412
4Principles underpinningthe Women’s Health PlanThe Plan is underpinned by the following principles:AddressinginequalitiesA life courseapproachResponding to the unjust andavoidable differences in people’shealth across the populationand between specificpopulation groups.Taking advantage of thedifferent stages in awoman’s life whichpresent both healthchallenges andopportunities to promoteand protect healthand wellbeing.Everyone who usesand provides NHSservices has a right to betreated as an individualand with consideration,dignity and respect.Acknowledging and respondingto the many characterisitics andfactors which shape women’slives such as ethnicity, disability,sexual identity and background.Gender equality andintersectionalityWomen’s Health Plan A Plan for 2021-24Respectful andinclusive services13
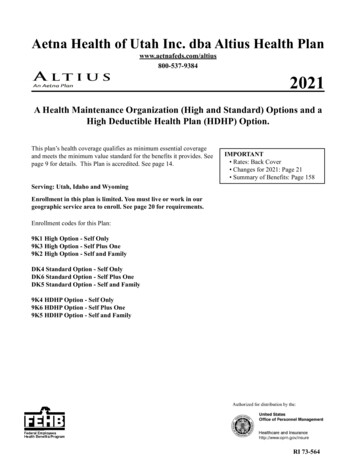
4.1 Addressing inequalitiesThe fundamental causes ofhealth inequalities are an unequaldistribution of income, power andwealth. This can lead to poverty andmarginalisation of individuals andgroups.Inequalities in health outcomes exist between bothmen and women and between different groupsof women in Scotland. In the most affluent areasof Scotland, women experience 25.1 more yearsof good health compared to the most deprivedareas28. Health inequalities such as this are unjustand preventable.We can reduce some health inequalities byidentifying gaps in health service provision,considering areas of best practice and developingactions to address these gaps, tailored to meet theneeds of all women. However we recognise this isonly part of a wider picture when it comes to healthand wellbeing.Women are individuals with individual needs,experiences and backgrounds which impact theirhealth and wellbeing. Multiple factors affect howwomen care for themselves, access information,seek advice, make choices, and their risk of illness.Social determinants of healthHealth inequalities are socially determined bycircumstances largely beyond an individual’scontrol. These circumstances can disadvantagepeople and limit their chance to live longer, healthierlives29.Social determinantsof healthPublic Health ScotlandHealth inequalities: What are they?How do we reduce them?These factors cannot be solely addressed by theWomen’s Health Plan, however improving accessto health services has an important role to play inreducing health inequalities.Health policy and resources need to take accountof the social determinants of health and delivery ofhealthcare has to be joined up and accessible to bemost effective. By working together, health, socialcare and third sector organisations can supportand empower women to make changes to theirlifestyles and live healthier lives. Health servicescannot themselves address health inequalitieswhich relate to deprivation, homelessness and poorhousing or education and lack of opportunities.Health services can however work alongside otherprofessionals, with different expertise. Working withlocal authorities, the third sector and other partnersin a holistic approach to women’s care can allowwomen the opportunity to address, for example,accessing social security support at the same timeas attending her doctor for contraception or herchildren’s health.The social determinants of health are theconditions in which we are born, we grow andage, and in which we live and work. The factorsbelow impact on our health and alsupportFamily incomeEmploymentOur communitiesAccess tohealth servicesWomen’s Health Plan A Plan for 2021-2414
By working together we can address some of thesegaps and meet the specific and individual needs ofwomen.I met up with the nurses again andthe whole team at the clinic, honestlyI haven’t looked back, the clinic iswel
Apr 26, 2021 · 7.1 Women’s Health Group 26 7.2 Sub-groups 26 8 Context 27 8.1 Access to information and services 27 . For too long women have been disadvantaged, and this has impacted their right to health. It is time that . Corinne Love, and the sub-group chair