Transcription
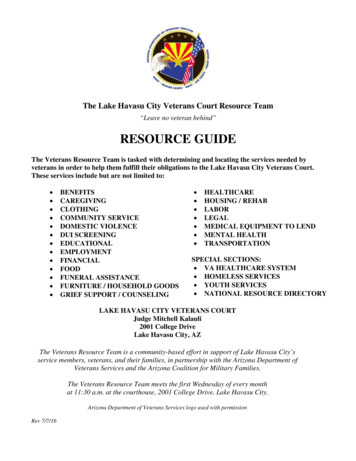
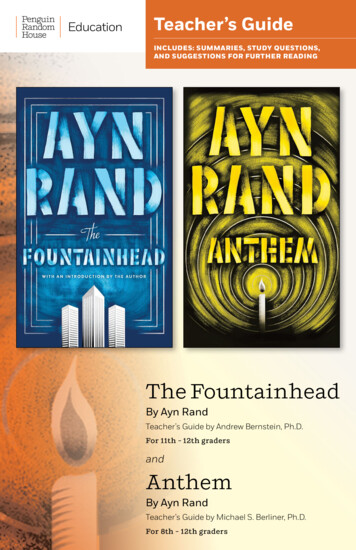
VETERANS RAND 36 ITEM HEALTH SURVEY(VR-36) Please do this: Instructions: This survey asks for your views about your health. This information will help keep trackof how you feel and how well you are able to do your usual activities.Please answer every question by filling in one circle on each line. If you are unsure about how to answera question, please give the best answer you can.1. In general, would you say your health is: EXCELLENTVERY GOODGOOD FAIR POOR2. The following questions are about activities you might do during a typical day. Does your health nowlimit you in these activities? If so, how much?NO, NOTYES,YES,LIMITEDLIMITED LIMITEDAT ALLA LOTA LITTLEa. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports?b. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf?c. Lifting or carrying groceries? d. Climbing several flights of stairs? e. Climbing one flight of stairs? f. Bending, kneeling, or stooping? g. Walking more than a mile? h. Walking several blocks? i. Walking one block? j. Bathing or dressing yourself? 3. During the past 4 weeks, have you had any of the following problems with your work or other regulardaily activities as a result of your physical health?NO,YES,YES,YES,YES,NONEA LITTLESOMEMOSTALLOF THEOF THEOF THEOF THE OF THETIMETIMETIMETIMETIMEa. Cut down the amount of time you spent on work or other activities.b. Accomplished less than you would like c. Were limited in the kind of work or other activities.d. Had difficulty performing the work or other activities (for example, it took extra effort).
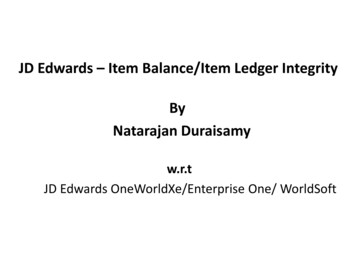
4. During the past 4 weeks, have you had any of the following problems with your work or other dailyactivities as a result of any emotional problems (such as feeling depressed or anxious)?NO,YES,YES,YES,YES,NONE A LITTLESOMEMOSTALLOF THEOF THEOF THEOF THEOF THETIMETIMETIMETIMETIMEa. Cut down the amount of time you spent on work or other activities.b. Accomplished less than you would like. c. Didn’t do work or other activities as carefully as usual.5. During the past 4 weeks, to what extent has your physical health or emotional problems interferedwith your normal social activities with family, friends, neighbors, or groups? NOT AT ALL SLIGHTLY MODERATELY QUITE A BIT EXTREMELY6. How much bodily pain have you had during the past 4 weeks? NONE VERY MILD MILD MODERATE SEVERE VERY SEVERE7. During the past 4 weeks, how much did pain interfere with your normal work (including both workoutside the home and house work)? NOT AT ALL A LITTLE BIT MODERATELY QUITE A BIT EXTREMELY8. These questions are about how you feel and how things have been with you during the past 4 weeks.For each question, please give the one answer that comes closest to the way you have been feeling.How much of the time during the past 4 weeks:a. Did you feel full of pep?b. Have you been a verynervous person?c. Have you felt so down inthe dumps that nothingcould cheer you up?d. Have you felt calmand peaceful?e. Did you have a lot ofenergy?ALLOF THETIME MOSTOF THETIME A GOODBIT OFTHE TIME SOME OF A LITTLETHEOF THETIMETIME PLEASE CONTINUE NONEOF THETIME
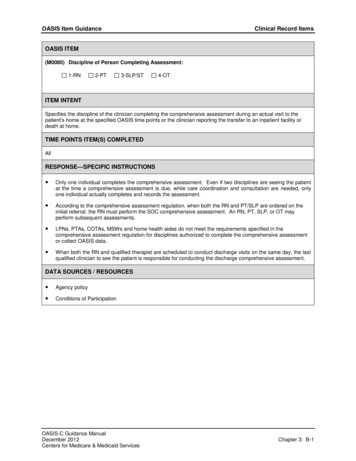
8. Continued from page 4 How much of the time during the past four weeks:f. Have you feltdownhearted and blue?g. Did you feel worn out?h. Have you been ahappy person?i. Did you feel tired?ALLOF THETIME MOSTOF THETIME A GOODBIT OFTHE TIME SOMEOF THETIME A LITTLEOF THETIME NONEOF THETIME 9. During the past 4 weeks, how much of the time has your physical health or emotional problemsinterfered with your social activities (like visiting with friends, relatives, etc.)? ALL OFTHE TIME MOST OFTHE TIME SOME OFTHE TIME A LITTLE OFTHE TIME NONE OFTHE TIME10. Please choose the answer that best describes how true or false each of the following statements is foryou.DEFINITELY MOSTLYNOTMOSTLY DEFINITELYTRUETRUESUREFALSEFALSEa. I seem to get sick a lot easier than other people.b. I am as healthy as anybody I know.c. I expect my health to get worse. d. My health is excellent. Now we’d like to ask you some questions about how your health may have changed.11. Compared to one year ago, how would you rate your physical health in general now? MUCHBETTER SOMEWHATBETTER ABOUT THESAME SOMEWHATWORSE MUCHWORSE12. Compared to one year ago, how would you rate your emotional problems (such as feeling anxious,depressed or irritable) now? MUCHBETTER SOMEWHATBETTER ABOUT THESAME SOMEWHATWORSE MUCHWORSE
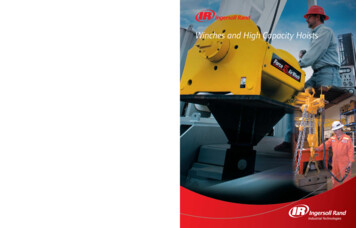
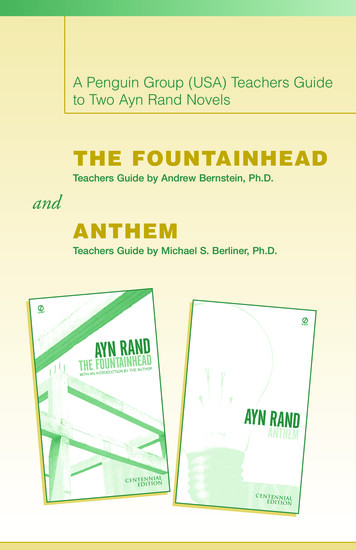
HOWTOSCORETHEVR- ‐36QUESTIONNAIRESTEP1: SCORING QUESTIONS:1, 11, 5, 7, 10b, 10d12345RESPONSE ASSIGNEDSCORE VALUE10075502502a, 2b, 2c, 2d, 2e, 2f, 2g, 2h, 2i, 2j1230501003a, 3b, 3c, 3d, 4a, 4b, 4c1234510075502506, 8a, 8d, 8e, 8h1234561008060402008b, 8c, 8f, 8g, 8i1234560204060801009, 10a, 10c123450255075100QUESTION NUMBERORIGINAL RESPONSE
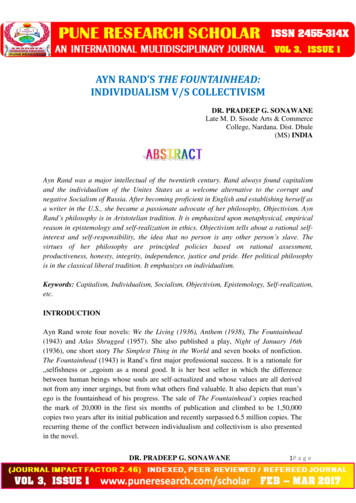
HOWTOSCORETHEVR- ‐36QUESTIONNAIREStep 2: Averaging Items to Form Scales for VR-36ScaleNumber ofitemsAfterscoring/recoding asper Step 1,average the followingitemsPhysical functioning102a, 2b, 2c, 2d, 2e,2f, 2g, 2h, 2i, 2jRole limitations due to physicalhealth43a, 3b, 3c, 3dRole limitations due to emotionalproblems34a, 4b, 4cEnergy/fatigue48a, 8e, 8g, 8iEmotional well-being58b, 8c, 8d, 8f, 8hSocial functioning25, 9Pain26, 7General health51, 10a, 10b, 10c, 10d
January 2000Volume 5A Publication for Members of Medical Outcomes TrustThe Veterans SF-36 Health StatusQuestionnaire: Development and Application inthe Veterans Health AdministrationMEDICALOUTCOMESTRUSTLewis E. Kazis, Sc.D.MONITORDr. Kazis is Director of the Veterans SF-36 Project for the Office of Quality and Performance for theVeterans Administration, Washington, D.C. He is the Chief of Health Outcomes for the Center forHealth Quality, Outcomes and Economic Research, a Health Services Research and DevelopmentField Program, Veterans Administration Medical Center, Bedford, Massachusetts. He is alsoAssociate Professor of Health Services at the Boston University School of Public Health.ContentsFeatureResearch SummaryInitiativesClinical PracticeApplicationsResearch & PolicyHealth SystemImprovementIssue 113579Most policy makers concede that reducing costs, maintaining quality of careand ensuring optimal patient outcomes are key priorities for restructuring thehealthcare system in the United States. In thisrapidly changing environment, accountabilityfor patient care outcomes is a key priority. Tomeet these challenges of increased competitionand accountability, patient-based measures ofhealth are increasingly being adopted by healthcare systems as measures of outcomes. Thesemeasures define, from the patients perspectives, what is important in terms of both physical and psychological functioning.Patient-based measures are comprehensiveassessments of functional status (e.g., physical,psychological, social and role functioning) andoverall perceptions of health. They provideaccurate and valid summaries of health statusthat synthesize domains of morbidity, disability, and disease burden. They also give animportant summary description of the complexmix of patient characteristics.The Veterans Health Administration(VHA), is the nation s largest integrated healthcare system with approximately 4 millionenrollees in the VA system and about five percent of the total market share for hospitalservices in the nation.1 It serves a select groupof veterans with complex healthcare needs.Compared to veterans nationally and the general US population, users of the VA healthcaresystem not only have disabilities that are connected to their military service, they are alsoolder, poorer, less educated, and sicker withmore disease.2, 3 Lessons learned from the VAcan provide a model for monitoring the outcomes of care in other managed care systems,especially those serving older populations. Likeother healthcare systems that are seeking toadapt to a changing healthcare environment,the VA needs information about the health ofcurrent and prospective patients to anticipatepatient demand, design effective services, andevaluate the outcomes of its care.In a memorandum in March 1997, theUnder Secretary for Health, Dr. Kenneth W.Kizer stated:The Veterans Health Administration sperformance measurement system wasdesigned to ensure the delivery of excellent healthcare value as originallydefined by four domains of value: access,cost/price, technical quality, and customer satisfaction. VHA has decided toinclude functional status as the fifthdomain of value, given its increasingimportance in clinical medicine.4 (sic)In an environment of healthcare restructuring the VHA is aggressively moving towardsimplementing an outcomes management system. This system will capitalize on well established measures that have been developed bothinside and outside the VHA. Measures such asthe Veterans SF-36 are well-validated assessments of functional status that can be used tocharacterize the case-mix of patient populations. These measures can also be used to monitor the process and outcomes of care at the program or system levels.When administered to a patient population at a point in time, the Veterans SF-36 provides an indication of the case-mix, or diseasecomplexity of a patient group.5 Such measureshave a direct bearing on patient needs, workload, and costs of care. Through the Office ofQuality and Performance in the VHA, systemsusing the Veterans SF-36 are currently beingdeveloped.The Veterans Health StudyHistorically, the information regarding ambulatory care that is available to VA providers,11The Veterans SF-36 and scoring algorithms are available on request from the author.
Veterans Healthadministrators, and policy makers hasbeen quite limited. The Veterans HealthStudy (VHS), a service directed projectthat was launched in 1992, has as its primary goal the development and application of methodology for assessing healthrelated quality of life (HRQoL) withinthe VHA. These assessments are primarily structured questionnaires administeredto the patient and are reliable and validin ambulatory populations. The VHSimplements and demonstrates the validity of using patient-derived measures ofhealth, since this information reflects thehealthcare needs of veterans that can beused for monitoring the outcomes oftheir care.The VHS was designed to develop,test, and disseminate information systems for monitoring patient-derived outcomes of ambulatory care within theVA. The VHS has as its principal goal togenerate measures of functional statusthat are tailored to the veterans needsand represent the complex health characteristics of its patient population. Thesehealth characteristics of veterans, orpatient-mix, include the sociodemographics and mix of diseases for anambulatory patient population that usesthe VA system of care.The conceptual framework andmethods of the VHS are described elsewhere.6-7 We characterize the health status of patients using multidimensionalassessments of HRQoL. In doing this,we build on the work of previous studies, most notably the Rand HealthInsurance Experiment and the MedicalOutcomes Study (MOS).8-9 These studies have demonstrated the value and utility of patient-based measures ofHRQoL.The VHS has gone beyond thiswork and has developed a core set ofgeneral measures of health status and disease as part of a comprehensive set ofassessments, which can be used by theVA and other healthcare systems forresearch and patient management purposes. Unlike the MOS where administrative data was not available, the VHShas capitalized on the rich secondaryadministrative databases available in theVA; these include diagnoses, data on utilization of services and procedures, onMonitor, January 2000, volume 5, issue 1an inpatient and outpatient basis.Patient-derived measures of health havebeen merged with administrative data atthe individual patient level. The access tothese databases has provided a uniqueand powerful opportunity to examinepatient outcomes in the context of casemix measures obtained that are externalto the patient-derived assessments.The VHS is a four-year prospectiveobservational study of health outcomesin patients receiving ambulatory carefrom the VHA. A panel of 2425 patientshave been followed annually for clinicaland HRQoL assessments. The details ofthe VHA design and sampling procedures are described elsewhere.5 Bothgeneral and disease-specific HRQoLassessments have been validated in thisstudy. This methodology is particularlygermane to VA healthcare, which servespatients with a complex profile of conditions, sociodemographics, and militaryhistory that is strongly related to theireligibility for VA care. The VHS haspublished 15 articles in peer-reviewedjournals with general and disease-specificassessments for the Veterans SF-36, diabetes, osteoarthritis, chronic low backpain, chronic lung disease and alcoholrelated problems (references and scoringalgorithms available on request). In addition, a comorbidity index has also beenvalidated as a case-mix adjuster for measures of health status and healthcare utilization.One of the cornerstones in the VHSis the development of the Veterans SF36, a short form health status assessmentdesigned specifically for use among veterans. The Veterans SF-36, adapted fromthe MOS SF-36,10-11 spans the range ofhealth concepts from physical to psychological status. The Veterans SF-36 provides a means to measure patient outcomes of care.The Veterans SF-36The Veterans SF-36 is our primary measure of health-related quality of life. Thisassessment has been documented as reliable and valid in ambulatory VA patientpopulations.7,12 This assessment buildson the MOS SF-36 and has been adoptedby the VHA as one of the performance2measures of functional status.Modifications to the MOS SF-36 includechanges to the role items (role limitations due to physical and emotionalproblems), where response choices thatwere originally dichotomized yes/nochoices are now five-point ordinal choices ( no, none of the time to yes, all ofthe time ). These changes to the SF-36increased the precision and discriminantvalidity of the role scales and physicaland mental component summaries. Thechanges to the role scales of the SF-36demonstrated increases to the precisionof the scales by more than 100 percentfor the role-physical and 80 percent forthe role-emotional. The changes to thesetwo scales also lowered the floor andraised the ceiling of the metric as reflected in each of the scales distributions. Inaddition, the modified scales when usedin calculating the physical and mentalcomponent summary scales haveimproved precision by five percent (seesummary scale description below).The Veterans SF-36 has been widelyused, disseminated, and documented inthe VA.13 Like the MOS version of theSF-36, the Veterans SF-36 measures eightconcepts of health: physical functioning(PF), role limitations due to physicalproblems (RP), bodily pain (BP), generalhealth perceptions (GH), energy/vitality(VT), social functioning (SF), role limitations due to emotional problems (RE),and mental health (MH). A measure ofreliability, or the internal consistency, ofitems measuring a concept about healthis given by Cronbach s alpha. This statistic ranges from 0.00 to 1.00, where higher values indicate greater reliability.Scales or concepts with values of 0.70 orhigher are considered acceptable.Results for the Veterans SF-36 scales giveCronbach s alphas ranging from 0.93 forphysical functioning to 0.78 for socialfunctioning. Items from each conceptare summed and rescaled with a standardrange from 0 to 100, where 100 denotesthe best health. These eight conceptshave also been summarized into twosummary scores: a physical componentsummary (PCS) and a mental component summary (MCS). The summaryscales are based upon distinct physicaland mental constructs well documentedFeature continues on page 13
Veterans HealthResearch Summary: 1998-1999Welsh CH, Thompson K, Long-Krug S.Evaluation of patient-perceived health statususing the Medical Outcomes Survey ShortForm 36 in an intensive care unit population.Crit Care Med 1999 Aug;27(8):1466-71OBJECTIVE: Baseline patient functional statusas assessed by providers is correlated with mortality after intensive care unit (ICU) admission.We wanted to see if patient self-perception ofhealth status before admission to an ICU correlated with functional outcome. DESIGN:Prospective survey on a convenience sample.SETTING: Single urban university-affiliatedVeterans Affairs Medial Center. PATIENTS:One hundred ninety-nine patients in surgicaland medical/coronary ICUs. INTERVENTIONS: None. MEASUREMENTS: Patientassessed baseline health status was monitoredwith the Medical Outcome Survey Short-Form36 (SF-36), consisting of 36 questions that evaluate eight health status concepts. In addition,baseline functional status (Zubrod scale) wasdetermined and severity of illness (AcutePhysiology and Chronic Health Evaluation[APACHE] II) data were collected. Zubrod functional status, which includes mortality, wasdetermined 6 wks and 6 months after ICUadmission, and correlation coefficients were calculated. MAIN RESULTS: We found it feasibleto collect SF-36 health status data on a 9% sample in this setting. Less than 1% of responseswere completed by proxy. The SF-36 data wereinternally consistent, and several of its scalesincluding general health perception and physicalfunctioning correlated with patient Zubrod functional status (r2 .08, p .001; r2 .14, p .001) at 6 wks as did vitality (r2 .04, p .01),social function (r2 .03, p .05), and physicalrole function (r2 .02, p .053), although to alesser extent. Similar correlations were alsofound with 6-month functional status. CONCLUSIONS: We conclude that use of the SF-36is time efficient in an ICU setting and correlateswith 6-wk and 6-month functional outcome. Itcorrelates as well with functional outcome aseither the baseline Zubrod functional status orthe APACHE II severity of illness measurement.The five-question general health evaluation portion correlated almost as well with outcome asthe more extensive 36-item questionnaire. Use ofthe SF-36 may define patient populations forcomparison across hospitals. It may also targetindividuals with needs for additional posthospitalization care, including rehabilitation servicesor nursing home placement.Skinner KM, Furey J. The focus on womenveterans who use Veterans Administrationhealth care: the Veterans AdministrationWomen s Health Project. Mil Med 1998Nov;163(11):761-6Women have served in every war and conflict inour history, but the effects of military duty onwomen are largely unknown. This article discusses the history of women in the military andpresents findings from the VeteransAdministration Women s Health Project. Thisstudy was designed to describe the health-relatedquality of life of women veterans who receiveVeterans Administration ambulatory care. Weassessed health status using the Short Form 36,an easily administered 36-item health survey thathas been widely used and that has been shownto be reliable and valid. We compared ShortForm 36 scores between veteran and nonveteranwomen. The results indicate that veteran womenscore lower on every scale compared with nonveteran women.Unwin C, Blatchley N, Coker W, Ferry S,Hotopf M, Hull L, Ismail K, Palmer I, DavidA, Wessely S. Health of UK servicemen whoserved in Persian Gulf War. Lancet 1999 Jan16;353(9148):169-78.BACKGROUND: Various symptoms in military personnel in the Persian Gulf War 1990-91have caused international speculation and concern. We investigated UK servicemen. METHODS: We did a cross-sectional postal survey on arandom sample of Gulf War veterans (Gulf Warcohort, n 4248) and, stratified for age and rank,servicemen deployed to the Bosnia conflict(Bosnia cohort, n 4250) and those serving during the Gulf War but not deployed there (Eracohort, n 4246). We asked about deployment,exposures, symptoms, and illnesses. We an
VETERANS RAND 36 ITEM HEALTH SURVEY (VR-36) Please do this: Instructions : This survey asks for your views