Transcription
Using Hospital Admission,Discharge, and Transfer Data toCoordinate Care: Lessons fromTennessee and WashingtonSeptember 6, 2018A grantee of the Robert Wood Johnson Foundation
About State Health Value StrategiesState Health and Value Strategies (SHVS) assists states in their efforts totransform health and health care by providing targeted technical assistance tostate officials and agencies. The program is a grantee of the Robert WoodJohnson Foundation, led by staff at Princeton University’s Woodrow WilsonSchool of Public and International Affairs. The program connects states withexperts and peers to undertake health care transformation initiatives. Byengaging state officials, the program provides lessons learned, highlightssuccessful strategies, and brings together states with experts in the field. Learnmore at www.shvs.org.Questions? Email Heather Howard at heatherh@Princeton.edu.State Health Value Strategies 2
AgendaTennessee: Care Coordination ToolWashington: ER is for EmergenciesDiscussionState Health Value Strategies 3
ADMISSION DISCHARGE ANDTRANSFER IN TENNESSEEBrooks Daverman, Director of Strategic Planning
ADTs are the most actionable real-time electronicinformation in health care todayADT uses Increase primary care follow up from ED and inpatient visits Help primary care and behavioral health providers find hardto-reach patients Facilitate patient education on appropriate ED use Increase access to patients’ care history5
Tennessee Providers see the benefit of ADT “We’ve been able to really monitor the ADT feeds and recently noticed we had aconsumer that went 18 times for a hospitalization or ED visit over 90 days. That was eyeopening for us.”- Andrea Westerfield, Mental Health Co-op “We had a patient we’d been treating since 1993 for schizophrenia. When we startedreceiving admission, discharge and transfer feeds from the hospitals, we discovered thatshe would come to our office and then immediately head to the ER for treatment of herphysical health conditions. This was a real opportunity for us to improve care.” –PamWomack, CEO, Mental Health Co-op “It is not uncommon for one of our patients to discharge from the hospital and notunderstand what the next step would be in having their condition addressed. We utilizethe information from the ADT export as well as the ADT summary to help our patientsstay on track post discharge [ ]It is very helpful to have the name of the physician (at thehospital), and the admit diagnosis so we can link our members to resources andadditional follow up appointments. We also utilize the ability to pull ADT history, toidentify patterns of hospitalizations for our patients. This allows us to build supports forthe member that would reduce the need for rehospitalization for a condition that can besafely and appropriately addressed here at our office.” – Victoria Allen, LifeCareTwo minute video of Tennessee providers talking about ADT at:https://youtu.be/9Em69pakIfY6
In 2015 and 2016, MCO reps and consultants met with allTennessee hospitals to ask them to send ADT data. This iswhat they heard:How will you address[Lack of technical[insert technicalexpertise]privacy question]?What if payers[Lackof trust]use thistodeny payment?We can do this afterpriority]we[Lackfinishofourlong ITto-do list.What is the[Lack of 2-waybenefit tobenefit]hospitals?Sometimes we were talking to the wrong person7
TennCare and the Tennessee Hospital Association (THA)have a history of working together to solve problems. In2017, we worked together to get agreement with all hospitalsto share ADTs.Technical expertise[Lackof technicalthrough Audaciousexpertise]Inquiry (Ai)Long-term[Lack oftrustingtrust]partnershipPriority created byTHA Board[Lack of priority](agreement totimeline)Hospitals can[Lack of 2use data onwaybenefit]readmissionTHA was able to connect to the right personTennCare also tied hospital pool payments to submitting ADT data. 8
Over the past year, Tennessee has connected mosthospitals in the state9
Providers receiving ADT informationPatient-Centered Medical Home (PCMH): 67 primary care organizationscaring for 450,000 TennCare members at over 300 sites throughout the State.Tennessee Health Link: a health home program providing care coordination for65,000 TennCare members with significant behavioral health needs with 22behavioral health providers at over 100 sites throughout Tennessee10
TennCare ADT Data FlowADTADT ADTADTADT Care CoordinationToolADTClaims andAttribution11
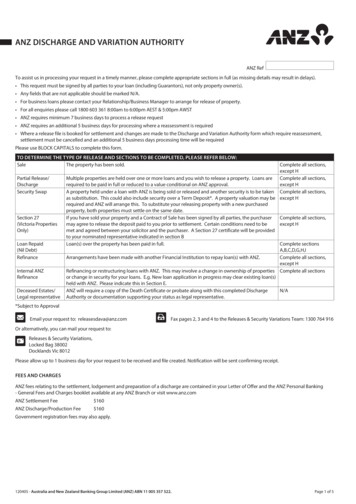
A multi-payer shared care coordination tool allows primary care providers toimplement better care coordination in their offices.Care Coordination Tool Functions Allows practices to view their attributed member panel Real time admissions, discharges, and transfers (ADT feeds)and follow-up tracking Patient risk scores Generates and displays gaps-in-care based on qualitymeasures and tracks completion of activities Displays claims – including pharmacy
CCT Screenshot: Landing Page13
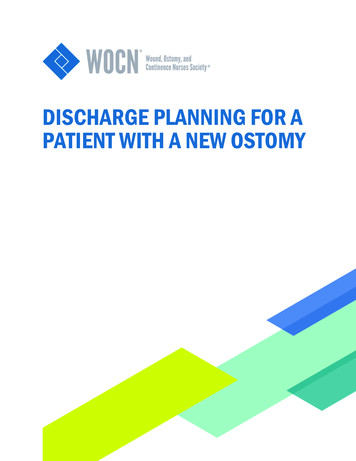
CCT Screenshot: ADT Tab14
CCT Screenshot: ADT DetailThis is the actual codeddiagnoses TennCarereceives in the DG1segment of the HL7. This isa diagnosis someoneentered in the EMR at thetime of visit.15
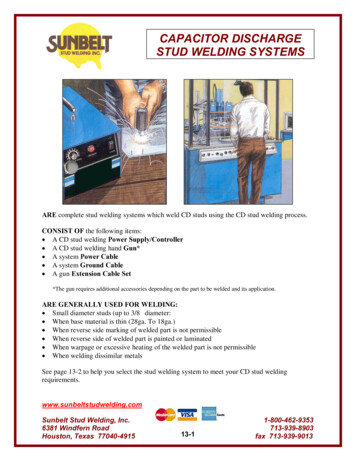
CCT Screenshot: Member Panels and Risk Scores Within the My Members tab, CCT users can: View information about their attributed members for each MCO View the member’s risk information at a glance and stratify members byrisk or disease16
CCT Screenshot: More Population Health ToolsCCT users can easily stratify theirpopulation by risk score and by diseasestate.17
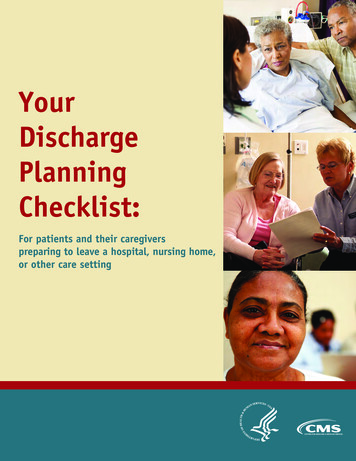
CCT Screenshot: Gaps in Care CCT users can view Gaps in Care for all of their attributed members. TheseGaps are closed based on weekly claims data loads and HEDIS-like rules.18
Thank youBrooks.Daverman@tn.gov19
ER is for Emergencies: ImplementingEmergency Room Best PracticesCharissa Fotinos, MDDeputy Chief Medical OfficerClinical Quality and Care TransformationSeptember 6, 2018Mary FlissDeputy for Clinical Strategy andOperations
Background Some patients visiting emergency departments couldbe treated effectively in a less costly setting There are evidence-based practices that can reducelow-acuity emergency room visits, coordinate care,and save health care dollars21
Creating the Partnership: Government In 2012, the Legislature passed House Bill 2127. Requires all Washington hospitals to implementseven best practices.22
Creating the Partnership: CoordinatedCare Washington State Hospital Association Washington State Medical Association Washington Chapter of the American College ofEmergency Physicians Washington State Health Care Authority23
Power of a Statewide Goal Standard policies in every hospital- No patient shopping for a different physician Safe Table Learning Collaboratives to share bestpractices Friendly competition towards a shared goal24
Seven Best Practices1.2.3.4.Track emergency department visits to avoid ED “shopping”Implement patient educationInstitute an extensive case management programReduce inappropriate ED visits by collaborative use ofprompt visits to primary care physicians5. Implement narcotic guidelines to discourage narcoticseeking behavior6. Track data on patients prescribed controlled substances7. Track progress of the plan to make sure steps are working25
Project Impact 98 hospitals now sharing emergency roominformation electronically 97 hospitals developed and use a standardized careplan format, providing consistent care no matterwhere a patient goes Expansion of care coordination efforts to allfrequently utilizers, regardless of payer Instant notification of Primary Care Providers26
Results Reduced ED Visits by 9.9% Reduced number of visits by frequent clients by10.7% Reduced visits resulting in a narcotic prescription by24% Reduced low-acuity visits by 14.2% High utilizers can generate multiple patient careplans, collaborative decision making as tomanagement Top 25 utilizers of EDs in WA have 1-7 clinical care guidelines27
Results cont. Using ED metrics for non-critical access hospitals ER is for Emergencies (adult and pediatric hospitals withemergency rooms only):– Percent of Patients with Five or More Visits to the Emergency Roomat the same facility with a Care Guideline Using information on high risk groups/high utilizers totarget interventions Adding claims data to enhance clinical information at thepoint of care28
Targeted Education Campaign29
Key to Successful State Initiatives Evidence-based Measurable Achievable benchmark, possible for everyone tosucceed with commitment and hard work Clear positive outcomes Strong partnerships30
Ongoing Barriers to Care Mental HealthAmong high utilizers of ER services, 80% havemental health issues Access to Dental CareRestoration of adult dental for Medicaid Patients Access to Primary CareExpanded medical health homes31
Other InformationER for Emergencies Data Dashboard: Go gton/data-dashboards click on the link to AIMData Dashboard Suite.32
Charissa Fotinos, MDDeputy Chief Medical OfficerClinical Quality and Care Transformationcharissa.fotinos@hca.wa.govTel: 360-725-9822Mary FlissDeputy for Clinical Strategy and OperationsClinical Quality and Care TransformationMary.Fliss@hca.wa.govTel: 360-725-181033
Q&AState Health Value Strategies 34
Thank You!Brooks DavermanBrooks.Daverman@tn.gov615-532-3163Charissa FotinosCharissa.Fotinos@hca.wa.gov360-725-9822Mary FlissMary.Fliss@hca.wa.gov360-725-1810Dan tate Health and ValueStrategies 35State Health Value Strategies 35
Allows practices to view their attributed member panel Real time admissions, discharges, and transfers (ADT feeds) and follow-up tracking Patient risk scores Generates and displays gaps-in-care based on quality measures and tracks comple