Transcription
Journal Pre-proofLeaflet fracture and embolization from an On-X mechanical mitral valveErik Helgeland, MD, PhD, Kristoffer Andresen, MD, Karl Andreas Dumont, MD,Johannes Lagethon Bjørnstad, MD, .1016/j.xjtc.2020.06.021Reference:XJTC 213To appear in:JTCVS TechniquesReceived Date: 27 May 2020Revised Date:27 May 2020Accepted Date: 17 June 2020Please cite this article as: Helgeland E, Andresen K, Dumont KA, Bjørnstad JL, Leaflet fractureand embolization from an On-X mechanical mitral valve, JTCVS Techniques (2020), doi: https://doi.org/10.1016/j.xjtc.2020.06.021.This is a PDF file of an article that has undergone enhancements after acceptance, such as the additionof a cover page and metadata, and formatting for readability, but it is not yet the definitive version ofrecord. This version will undergo additional copyediting, typesetting and review before it is publishedin its final form, but we are providing this version to give early visibility of the article. Please note that,during the production process, errors may be discovered which could affect the content, and all legaldisclaimers that apply to the journal pertain.Copyright 2020 The Authors. Published by Elsevier Inc. on behalf of The American Association forThoracic Surgery
1Leaflet fracture and embolization from an On-X mechanical mitral valve2Erik Helgeland MD, PhD 1, Kristoffer Andresen MD 2, Karl Andreas Dumont MD 1, Johannes3Lagethon Bjørnstad MD, PhD 1,441Department of Cardiothoracic Surgery, Oslo University Hospital, Rikshospitalet52Department of Cardiology, Oslo University Hospital, Rikshospitalet64Institute of Clinical Medicine, University of Oslo789Conflicts of interest: None10Consent: The patient has provided written informed consent to the publication of this article.11Corresponding Author:12Erik Helgeland, MD, PhD13Department of Cardiothoracic Surgery, Oslo University Hospital, Rikshospitalet14Sognsvannsveien 20, 0372 OSLO15Email: helger@ous-hf.no16Article word count: 7561718191
20Central message21We report the case of a 26 year old male who presented with cardiogenic shock due to leaflet22fracture and embolization from an On-X mitral valve prosthesis implanted just one year23previously.2425262728293031323334353637382
39Leaflet escape is a dangerous, but exceedingly rare complication of modern mechanical heart40valves. Whereas some older models, in particular a version of the Björk-Shiley tilting disc41prosthetic valve, reported a 3.9 % cumulative incidence of leaflet escape [1], modern42mechanical bileaflet heart valves rarely fail. Only three previous cases of leaflet embolization43from On-X mechanical valves have been reported, two in mitral position and one in aortic44position [2-4]. Herein we report the fourth case, and the second to survive and recover from45surgery.46Clinical Summary47A 26 year old man presented to the emergency department of his local hospital with acute48onset of dyspnea during treadmill exercise. He had one year previously undergone elective49mitral valve replacement at another institution with an On-X 25/33 mitral valve with50conform sewing ring (On-X Mitral Heart Valve, Cryolife, Kennesaw, Georgia, USA) due to51rheumatic mitral stenosis with regurgitation. He was admitted in cardiogenic shock with52pulmonary edema and hypotension after minor hemoptysis. Transthoracic echocardiography53(TTE) revealed a large mitral regurgitation and increased antegrade velocity of 2.5 m/s over54the prosthesis, which prompted the suspicion of prosthetic valve thrombosis, despite his INR-55level being 2.3 at the time of admission. He was stabilized with non-invasive continuous56positive pressure ventilation before transfer to a tertiary hospital. He was taken directly from57the emergency room to the cardiac catheterization laboratory where fluoroscopy revealed58single leaflet opening (Figure 1A) and TTE confirmed the mitral valve prosthesis having a59single moving leaflet and large mitral regurgitation (Figure 1B). Intravenous thrombolysis60was administered on the suspicion of acute valve thrombosis with no beneficial or adverse61effects. The following morning he was still in cardiogenic shock, and was stabilized with an62intra-aortic balloon pump (IABP). Repeat TTE raised a suspicion that the non-visualized63leaflet was not in situ, which was later supported by transesophageal echocardiography3
64(Figure 1C). Plain X-ray of the abdomen was unable to visualize any escaped leaflet. He was65thus taken directly to the operating room for emergency mitral valve surgery which confirmed66the diagnosis of leaflet escape. The old prosthesis was explanted (Figure 1D) and replaced67with a new prosthesis of the same size and brand. Postoperative CT without contrast located68the missing leaflet in the abdominal aorta just above the bifurcation (Figure 2A). Laparotomy69was performed the following day and the valve lid was explanted through a transverse70aortotomy (Figure 2B and C). Only after vessel closure was the IABP removed under direct71visual control to avoid any tears or damage to either the device or the vessel wall. The72remaining one quarter piece has not been accounted for but is suspected to lay distal to the73knees, as this is the only area not yet imaged. The patient was discharged to his local hospital74four days after admission and was doing well without any lasting disability at his three75months postoperative follow up. A written informed consent has been obtained for the76publication of this case report.77Comment78Our institution implemented the use of the On-X valve prosthesis in year 2000, and has per792019 implanted 775 mechanical mitral prostheses, of which 426 were On-X valves. We80perform 59% of all mitral valve operations in Norway [5]. This is the first case of leaflet81fracture we have observed in this prosthesis, and only the fourth ever published in the82literature. One other reported failure has been with the On-XMC 25/33 which has the conform83sewing ring[2], while this information is not available for the other two cases, one in aortic[4]84and one in mitral position[3]. As illustrated in this case report, distinguishing leaflet escape85from valve thrombosis can be challenging with fluoroscopy and TTE. Transesophageal86echocardiography can give valuable information when evaluating suspected prosthetic valve87dysfunction but is not always available or might require anesthesia which could destabilize a88hemodynamically compromised patient. A non-contrast CT scan however is fast, readily4
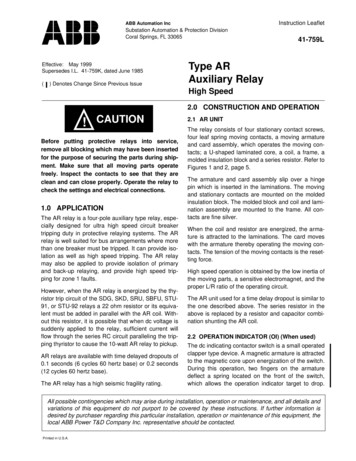
89available, does not require sedation and could indirectly have made the diagnosis by90localizing the escaped leaflet. Of note, we could not visualize the fragment using plain X-ray.91As this is one of the earliest leaflet escapes on record with any modern mechanical valve92prosthesis, the fractured leaflet was examined by scanning electron microscopy, alas without93finding any certain cause of the fracture. The manufacturer has, after its own review, not been94able to identify any flaws or errors in the production of the prosthesis, but it is well known95that surgical mishandling during implantation of mechanical prosthesis can create96microscopic surface scratches leading to weak points for later fracture.97Central picture legend:9899Explanted On-X mitral prosthesis with one leaflet missing.100101Video Legend:102103Video showing fluoroscopy and transesophageal echocardiography with 3D reconstruction of104a patient in cardiogenic shock with one leaflet of his On-X mitral prosthesis missing.105106Figure legends:107Figure 1108Fluoroscopy (A), transthoracic echocardiography (B) and transesophageal echocardiography109with 3D reconstruction (C) of a patient in cardiogenic shock showing his mitral prosthesis110with one missing leaflet and a large regurgitation. After emergency mitral valve replacement,111this picture shows the explanted prosthesis with one leaflet clearly missing (D). Photo credit:112Øystein Horgmo, University of Oslo.5
113114Figure 2115Computer tomography without contrast taken postoperatively shows the location of the116embolized leaflet in the abdominal aorta, denoted by white arrow (A). Three quarters of the117missing valve lid (B) was removed from the abdominal aorta via laparotomy (C). The118remaining one quarter piece has not been accounted for but is suspected to lay distal to the119knees, as this is the only area not yet imaged. Photo credit: Øystein Horgmo, University of120Oslo.121Acknowledgements:122The authors gratefully acknowledge the talented surgeons who performed the operations123described in this case report: Sigurd Birkeland MD, PhD, Karl Andreas Dumont MD, Beate124Rikken Lindberg MD and Sabine Helena Wipper MD, PhD.1251.126127valve: a continuing clinical concern. Circulation, 2005. 111(21): p. 2850-7.2.128129Amoros Rivera, C., et al., Survival After Mitral Valve Replacement for Leaflet Escape in aContemporary On-X Mechanical Valve. Ann Thorac Surg, 2019. 108(5): p. e307-e309.3.130131Blot, W.J., et al., Twenty-five-year experience with the Bjork-Shiley convexoconcave heartKageyama, S., et al., Sudden haemodynamic collapse caused by leaflet escape of thecontemporary On-X mechanical valve. Eur J Cardiothorac Surg, 2018. 54(3): p. 608.4.Nora Göbel, M., Sara Tanriverdi, MD, Ragi Nagib, MD, Ulrich F.W. Franke, MD, PhD,132Cardiogenic shock due to leaflet migration of On-X aortic mechanical prosthesis. The Annals133of Thoracic Surgery, 2020. 109(3).1341355.Data from the Norwegian Heart Surgery s/norsk-hjertekirurgiregister1366
49 mitral valve replacement at another institution with an On-X 25/33 mitral valve with 50 conform sewing ring (On-X Mitral Heart Valve,