Transcription
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016ContinuousHome CareWhat Does It Mean and HowDoes a Hospice Make It Work?December 2016 WebinarWhat We Will Cover Today1. A review of the regulatory requirements for continuous homecare level of care2. A description of patients who are eligible for and can benefitfrom continuous home care level of care3. Documentation principles to support this level of care4. What a hospice should have in place to have a successfulcontinuous home care program5. The audits and monitors to have in placeLevels of Care (LOC)Medicare pays the hospice a per diem rate based on one of four levels of care– Routine Home Care– Inpatient Respite Care– General Inpatient Care– Continuous Home CareLevel of care determination– Made by the hospice interdisciplinary team (IDG)– Requires a change to the Plan of Care (POC)– Reevaluated by the IDG on a regular basis to assure appropriateness 2016 Hospice FundamentalsAll Rights Reserved1
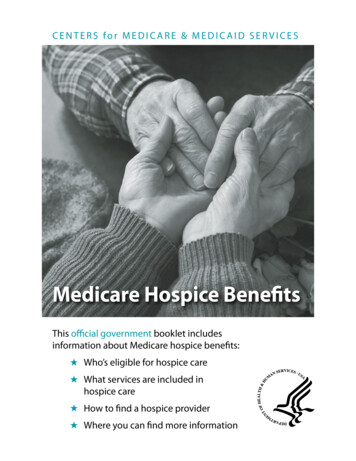
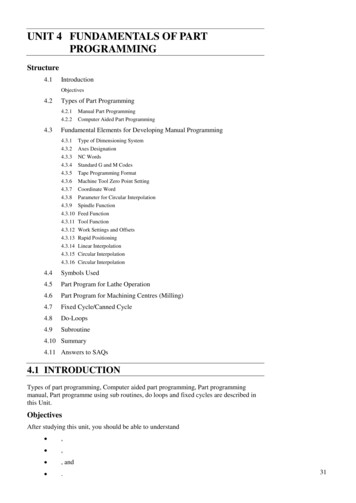
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Hospices Not Providing All Levels of CareCategoryNo GIP No CHCAll HospicesNorespiteNo GIPor CHC28%58%25%19%Less than 100100 – 1995725716054224117200 – 299300 – 4991785850116105500 or more23921By total # of Medicare Pts in 2013MedPAC Report to the Congress: Medicare Payment Policy March 2015The MedicareRegulationsRelating to Continuous Home CareSubpart F Covered Services§418.204 Special Coverage RequirementsPeriods of crisis.Nursing care may be covered on a continuous basis for asmuch as 24 hours a day during periods of crisis as necessaryto maintain an individual at homeEither homemaker or home health aide (also known ashospice aide) services or both may be covered on a 24‐hourcontinuous basis during periods of crisis but care duringthese periods must be predominantly nursing care 2016 Hospice FundamentalsAll Rights Reserved2
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Continuous Home CareA period of crisis is a period in which a patient requirescontinuous care, of which more than half is nursingcare, to achieve palliation or management of acutemedical symptoms and only as necessary to maintainthe patient at homeSubpart F Covered Services§418.204 Special Coverage RequirementsWhere It Can Be ProvidedPrivate residenceLong term care (when patient is not receiving Part A skilledcare)Assisted living facilityGroup homeHospice residential facilityContinuous Home Care PaymentPayment for continuous home care up to 24 hours/dayMinimum of eight hours of care during a 24 hour day (begins andends at midnight)More than half in any 24 hour period must be provided by ahospice employed RN or LPNIf a previously scheduled visit was made on the same day butprior to the start of the crisis, the visit time is not included in thecontinuous care hours 2016 Hospice FundamentalsAll Rights Reserved3
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Continuous Home CareProvided by a hospice employed RN or LPN/LVNMay enter into arrangements with another hospice program orother entity for the provision of core services in extraordinary,exigent, or other non‐routine circumstances.– Short‐term temporary event that was unanticipated– An unusual circumstance (not routine)– Must maintain professional managementContinuous Home CareContinuous home care hours are counted in 15 minuteincrements– Rounding to the next whole hour is not permitted– Units should only be rounded to the nearest incrementCare does not need to be continuousAll hospice aide or homemaker hours must be included in thecomputationMay not “discount” any portion of the hours in order to meetthe requirement that the care be predominantly nursing careMore Rules around Counting HoursCHC billing should reflect direct patient care during aperiod of crisisTime that cannot be counted– waiting for the patient to arrive– time taken for meal breaks, used for educating staff, usedto report etc.– Post mortem care– Modification of the plan of care and supervision of aides 2016 Hospice FundamentalsAll Rights Reserved4
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Overlapping of HoursMay be circumstances when patient's needs requires more thanone covered discipline at a timeResults in an overlapping of hours between the nurse and hospice aideOverlapping hours are counted separatelyEnsure that these direct patient care services are clearlydocumented and are reasonable and necessaryWould be an unusual circumstanceWhat is Defined as a Crisis?Palliation / management of acute medical symptomsObservation and monitoring to control pain and otheracute symptomsRequire predominantly nursing careActively dying?– Must be a clinical need for services, such as pain controlRemember, CHC is an attempt to solve / manage thecrisis while allowing the patient to remain at homeContinuous Home CareNursing careSkilled observation and monitoring when necessarySkilled care needed to control pain and other symptomsMay be provided to residents of nursing facilitiesIf a patient’s caregiver has been providing a skilled level ofcare and the caregiver is unwilling or unable to continueproviding careMay precipitate a period of crisis because the skills of a nursemay be needed to replace the services that had been providedby the caregiver 2016 Hospice FundamentalsAll Rights Reserved5
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Cues Indicating the Need for Continuous Home Care Increase in calls to the office for help Difficulty managing symptoms with intermittent visits Increase in after hours calls Statements of wanting to go to the hospital or to call 911 Caregiver’s anxieties and fears escalating to where no longer canprovide skilled care Patients discharged from hospital still requiring short term skilledcare needsHow Does ItWork?Making it HappenDetermine need for CHC meets the requirements (changes incomprehensive assessment)– What happened that the patient needs and qualifies for CHC?Change in plan of care with IDG involvement– Comprehensive assessment drives changes in POC, i.e. what is the change in condition– What care is going to be provided to manage the needs that qualified the patient for CHC?– How will the POC be different?As appropriate, obtain physician orders for any new medications orinterventions 2016 Hospice FundamentalsAll Rights Reserved6
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016How Does It WorkChange level of care and provide appropriate staffDocumentation shows what happened that the patientnow needs and qualifies for CHC– Interventions attempted and response by patientWhen the Crisis Is ResolvedComprehensive assessment drives changes in POC, i.e. crisis isresolvedChange in plan of care with IDG involvementHow will the POC be different?Obtain physician orders as appropriate for any new medicationsor interventions, change in level of careWhen endingMonitor for few more hours to ensure patient crisis is really over – notjust “will stop CHC at end of shift”Involvement of IDGContinuous home care is primarily focused on skilled nursingneeds to maintain the patient at homeHowever .– The services of SWs and Chaplains are expected during these periodsof crisis– Make sure SW and Chaplain continue to address the psychosocial andspiritual issues which may have escalated depending on the crisis Assessments and plan of care 2016 Hospice FundamentalsAll Rights Reserved7
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016So How DoesDocumentation Fit InWith All This?Documentation Is The final chapter of the life story of a personSubjective description of objective realityHow we communicate about the patient and families needs,goals and careProvides a mechanism for understanding what is working andwhat still needs to be managed effectivelySupports what is medically reasonable and necessary to supportpaymentCHC DocumentationMust clearly support the reason (or crisis) and the need to interveneDocument as frequently as necessary to support continued CHC ‐ suggested atleast hourly– Services provided– Symptoms managed– Skilled nursing care/interventions provided Monitoring Care provided & response to care Frequency of medications– Patient’s condition and response to care– Type of personnel providing care 2016 Hospice FundamentalsAll Rights Reserved8
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Documentation by the RN Case ManagerDaily visits by the RNCM should tell the story of why CHC,effectiveness of interventions and care required to managecrisisProvide a summary of the last 24 hours and a plan for thenext– What interventions have been provided– Response to care– PlanCHC for Patients in Nursing FacilitiesDocumentation not only reflects care provided byhospice staff but also care provided by NF staffInclude copy of NF MAR to reflect medicationsadministered during the period of crisis if hospice staffnot administeringDocumentation includes care coordination with NF staffDocumentation Prior to the CrisisThere must be a clinical need precipitated by a crisis forthis level of care to be warranted– What did the assessment show prior to initiation– The clinical need such as services for pain control, must beclearly evident in the documentation– Response to interventions tried 2016 Hospice FundamentalsAll Rights Reserved9
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Admitting Documentation Document failed interventions tried prior to initiation of CHC Reasons why new interventions can’t be provided by thecurrent caregiver(s) Why the family (or for NF residents why the NF staff) can nolonger provide the carePaint a clear picture about why management in their currentenvironment is not realisticAdmitting DocumentationDoes this paint the picture why admitted?Patient continues to have increased dyspnea, respiratorydistress, and associated anxiety, despite increase in steroidsand other medication changes over the past 2 days. Patient inneed of inhalation treatments every 2 – 3 hours and IVmedications every 4 ‐ 6 hoursWould it support CHC admission?Admitting DocumentationWhat about this case?Reason for CHC: Patient resides in a NF. Recent CVA withleft sided paralysis, difficulty swallowing resulting in theneed for thickened liquids and pureed diet. Difficultywith speech. 2016 Hospice FundamentalsAll Rights Reserved10
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Documentation of CHC Level of Care Should Answer these questions– Why here?– What is happening that can’t be managed in the home or atcurrent level in facility setting?Reflect a more intensive level of care– Shouldn’t read the same as the routine home care notesExpect to include– Medication adjustments or other stabilization treatments– Supporting documentation that the family / NF cannot provideneeded careOngoing DocumentationShould include––––––What the reason for level of care now is (today)Assessment of signs and symptomsMedication changes, titration, patient responseADL needs and dependencyVital signsCaregiver teachingPaint the picture of the patient and patient needs as identifiedon the Plan of CareOngoing DocumentationPain management requiring skills of nurse– Complicated technical delivery of medication– Can include teaching to patient or family on how toadminister– Frequent evaluation– Frequent medication adjustment– Aggressive treatment to control pain 2016 Hospice FundamentalsAll Rights Reserved11
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Ongoing DocumentationSymptom Changes––––––Sudden deterioration, requiring skills of nurseUncontrolled nausea/vomitingUnmanageable respiratory distressFrequent, skilled wound careOpen lesions requiring frequent skilled careNew or increased delirium, agitationClinical Notes Must Continuously and consistently support the terminalprognosis and reason for higher level of care Reason for admission or continued stayMeasures being taken to resolve the reason for admission orcontinued stayDocuments to problems, interventions and goals in POCProvide the reader with a visual of the whole case, ratherthan a stagnant snapshot in timeContinuous Care DocumentationDoes this tell the story of why?Death is imminent and family is unable to cope Actively dyingNo outputNo blood pressureFalling oxygen levelsWhat would be a better description?What is the real reason for CHC? 2016 Hospice FundamentalsAll Rights Reserved12
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016How to Build aSuccessful CHCProgramReview & Evaluate Current Data1.2.3.4.5.6.Referrals not admittedAfter hours calls for increased symptom managementLive discharges due to hospitalizations in non‐contracted facilityUnplanned hospitalizations# of patients requiring daily visits that are lasting severalhoursPatient / family complaintsBuilding Internal AwarenessSupport staff as they learn how to appropriately usethis new resourceTeach staff that CHC is a patient right and not stafffailureUse IDG to discuss situations where CHC could havebeen used to improve patient care and outcomes 2016 Hospice FundamentalsAll Rights Reserved13
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Building a CHC TeamBased on review of data, estimate number of patients / daysof potential CHCStart smallStaffingUse of LPNsUse of RNsNo Agency for RN / LPNsUse of Hospice AidesIdentification of educational needsDocumentation NeedsElectronic or paperSign‐in logsHourly documentationKnow how your software counts staff CHC hoursBased on payroll / visit time?Monitoring &Auditing 2016 Hospice FundamentalsAll Rights Reserved14
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016Processes to MonitorPre‐billing review of clinical notes to support level ofcare– Crisis management– Documentation supports ongoing need– Any patients in CHC greater than 3 daysIDG updates the POC when change level of care– From RHC to CHC– From CHC to RHCCHC Processes to MonitorContinuous home care log– Time patient arrived– Time patient diedClinical notes– Hourly documentation presentVerify logs to documentation for accuracy of timesPredominantly nursing care (RN/LPN)Summary – Key Concepts CHC§ 418.204 – Special coverage requirementsNursing care may be covered on a continuous basis for as muchas 24 hours a day during periods of crisis as necessary tomaintain an individual at homeA period of crisis is a period in which a patient requirescontinuous care, of which more than half is nursing care, toachieve palliation or management of acute medical symptomsand only as necessary to maintain the patient at home 2016 Hospice FundamentalsAll Rights Reserved15
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarDecember 2016To Contact UsSusan omRoseanne comCharlene omThe information enclosed was current at the time it was presented. This presentation is intended to serve as atool to assist providers and is not intended to grant rights or impose obligations.Although every reasonable effort has been made to assure the accuracy of the information within these pages,the ultimate responsibility for the correct submission of claims and response to any remittance advice lies withthe provider of services. 2016 Hospice FundamentalsAll Rights Reserved16
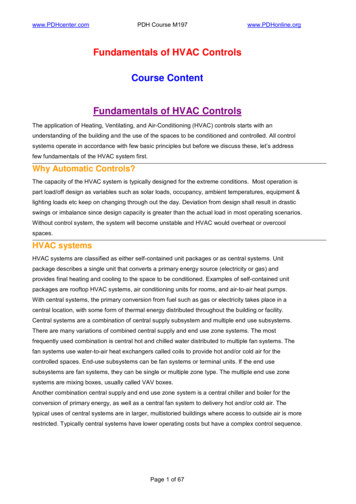
SymptomPain ControlDocumentation Reflects At home, pain was out of control despite medication changes Through and complete pain assessment(s) Medication adjustments, interventions and responseo Route, titration, use of prn, frequency Use of any complimentary therapies and response Respiratory DistressNausea / Vomiting /DiarrheaFamily CaregiverTeachingInsomniaR&C Healthcare Solutions8.2016 Breath sounds / or lack ofUncontrolled secretions / frequent need for suctioningSeverity of dyspneaAssociated tachypneaCough with evidence of symptoms such as anorexia, nausea, vomiting,exhaustion, rib fracture, musculo-skeletal painAnxiety levelDifficulty sleeping / sleeping positionRestlessnessElevation of head of bedInability to complete a sentence without gaspingSVN treatments Nausea / diarrhea intractable at home with current anti-emetic / anti diarrhearegime Assessment of nausea /diarrhea and interventions Frequency, amount, type of emesis or diarrhea Complaints of nausea without emesis Effects of diarrhea on skin integrity Hydration status Caregiver need to learn new modalityCaregiver willingness to learnModifications to plan of care to adapt into a home settingActual caregiver teaching provided and level of understanding Lowered pain threshold Sleep patterns Assessment of psychosocial historyPage 1
SymptomDocumentation Reflects Ascites Type of woundPainfulMalodorousDisfiguringFrequent dressing changesDescription of woundMedication(s) required prior to dressing changesDressing changes and other treatmentsPatient’s response to treatments, dressing changesDescription of patient behaviorsNeed for presence to controlEffect of agitation on patient and familyAmount, frequency, and effectiveness of medication required to controlagitationRespiratory compromiseDiuretic history and responseResponse to paracentesis (if applicable)Abdominal girthOther edemaFluid Overload Position of patientOxygen needsAmount of dyspneaEdema (amount and location)Difficulty sleeping at nightCardiac statusWound CareAgitationImminent DeathR&C Healthcare Solutions8.2016 Terminal restlessnesso Agitationo Deliriumo Hallucinations Clinical signs and symptoms of imminent death Inability for family to cope with the patient dying at homeo Psychological interventionso Spiritual interventionsPage 2
Dec 05, 2011 · Continuous Home Care What We Will Cover Today 1.A review of the regulatory requirements for continuous home care level of care 2.A description of patients who are eligible for and can benefit from continuous home care level of care 3.Documentation principles to support this level of File Size: 639KB