Transcription
Implementation of a Primary CareBased Teleretinal Screening Protocol forthe Los Angeles County Safety NetLauren Patty Daskivich, MD, MSHSLAC DHSCarol M. Mangione, MD, MSPHUCLA
Diabetic Retinopathy Diabetic retinopathy (DR) is a leading cause ofblindness in working-age adults in the United States Prevalence of diabetic retinopathy in a large study of Latinosin LA has been shown to be close to 50% THE leading cause of blindness in Los Angeles County Early Treatment Diabetic Retinopathy Study (ETDRS)showed that severe vision loss from diabeticretinopathy can be reduced by up to 94% byeffective treatments. At least 40-45% of diabetics who may benefit fromearlier detection and treatment of retinopathy arenot receiving it
Teleretinal Screening for DiabeticRetinopathy High sensitivity and specificity when comparedto gold standard (7 standard field fundusphotographs and indirect ophthalmoscopy by anophthalmic physician) Sensitivity: 71-82% Specificity: 92-96% Recognized by the American Academy ofOphthalmology No studies evaluating teleretinal screening in asafety net setting
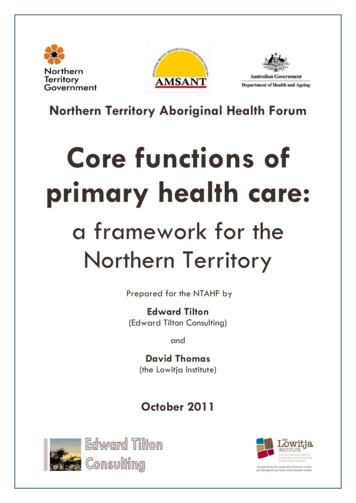
Clinical Pathway for TeleretinalImagingDiabe&c pa&entiden&fied at PCPvisitPa&ent sent fortelere&nal screeningat end of PCP visitPCP clinic submitseConsult based ondiagnosis/triagerecommenda&onsImages transmi edto reading centerImages reviewed, reportgenerated back to PCPImages acquiredPhotographer uploads imageto so:ware template andsubmits
Research QuestionProgram evaluation:Are we truly meeting our goals of increasing thenumber of patients screened and triaging thosein need of care in a more timely manner? Are we screening more patients for DR? Are wait times shorter? Does it cost less?
Methods Nonrandomized, quasi-experimental pretestposttest design Exposure at clinic level Historical controls Powered to detect a 15% difference (with a0.02 intra-clinic correlation) betweenintervention and control populations 5 clinics with control and intervention groups 120 subjects per clinic
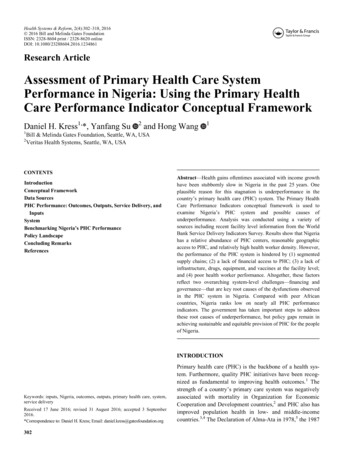
Outcomes: Aims 1-3Teleretinal ScreeningPrimary CareClinicControl (120 patients)6 monthsIntervention (120 patients)6 monthsPre-Post Analysis for Screening Rate for Diabetic Retinopathy:Screening rate at clinics post-TRS intervention – Screening rate at clinics pre-TRS interventionPre-Post Analysis for Patient Wait Time for Ophthalmology Appointment:Wait time for patients post-TRS intervention – Wait time for patients pre-TRS interventionPre-Post Analysis for Patient Wait Time for Definitive Ophthalmic Treatment for Moderate/Severe NPDR and PDR:Wait time for patients post-TRS intervention – Wait time for patients pre-TRS intervention
Outcomes: Aim 4 Complexity of societal vs. health systemsperspective What we can estimate Cost effectiveness of screening method – teleretinalimaging vs. direct eye exam Number of cases of blindness prevented andcompare to national estimates of cost of blindness Area for collaboration with health economist
CERP Aims Addressed Aim 1 – Promote bidirectional knowledge exchangebetween community and academia. Aim 2 – Build community and academicinfrastructure for sustainable partnered research Aim 4 – Build Health Services Research (HSR)methods into partnerships to accelerate design,production, and adoption of evidence-basedinterventions
TimelineActionStatusIRB approval from UCLA andLABioMedIRB approval from USCCompletedPre-intervention data collection at 4of 5 PC clinic sitesCompletedPre-intervention data collection atremaining PC site and 3Ophthalmology clinicsUnderwayJanuary 2014Implementation of DHS TeleretinalScreening ProgramUnderwayJanuary 2014 at study sites(June 2014 all sites)Post-intervention Data Collection at5 Clinic SitesPendingFebruary - March 2014Data Analysis and Preparation ofExtra-mural Grant ApplicationPendingApril - June 2014Under ReviewExpected Completion DateJanuary 2014
Added Value from CTSI Funding Access to Health Services Research andBiostatistical support available within the UCLACTSI Availability of the biostatistics core and healtheconomist to assist with data analysis Consultation to ensure that our quality assurancemechanisms are sufficient Advice on the design of a cost analysis of thisintervention Advice regarding additional pilot funding to assistwith dissemination if this project is found to besuccessful Research Assistant support
Next Steps and Products IRB approval obtained from UCLA, LABioMed; USC under review Major strides in implementation, including: Ensuring clinic access to fundus cameras for 13 DHS primary care sites Identifying and training fundus photographers (LVN/Medical Assistantlevel) Selecting and implementing the software platform for transmittingteleretinal images Creating a quality assurance mechanism for image acquisition andevaluation Establishing appropriate triage mechanisms for abnormal screeningphotographs integrated with eConsult, the new web-based LAC specialtyreferral system Teleretinal Screening has begun at 2 sites and will rollout to 11 moreover the next 6 months Currently developing a protocol for standardized referral timelinesacross LA County that will further streamline patient care
Teleretinal Screening for Diabetic Retinopathy High sensitivity and specificity when compared to gold standard (7 standard field fundus photograph