Transcription
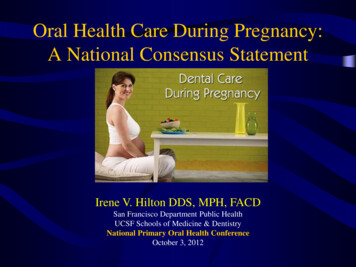
26/05/2017Dysphagia,oral care &hydrationAnita Lopes, RDDavid Beattie, cusCheekNursingBest xTracheaEsophagus2Swallowing phasesOral preparation:chewing, moistening,formation andcontrol of bolus1
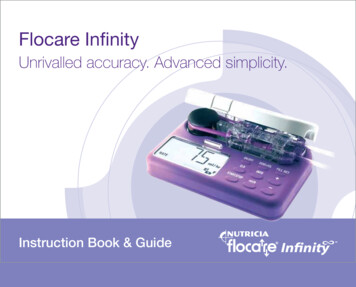
26/05/2017Swallowing phasesOral propulsive:transit of bolusto posterior oralcavitySwallowing phasesPharyngeal: airway protection, propulsionof bolus into esophagusSwallowing phasesEsophageal:transit to thestomach byperistalsis2
26/05/2017Normal Swallowhttps://www.youtube.com/watch?v PwVreNrTKBwDysphagiaOralPharyngealEsophagealSigns of dysphagiaOral stageNot managing secretionsLoss of food/fluid from the mouthUnable to form bolusFood residue in cheeks, on tongueor roof of mouth3
26/05/2017Signs of dysphagiaPharyngeal stageFrequent throat clearingCoughing, chokingGurgling or wet voiceNasal or oral regurgitationFood “stuck in throat”Absent swallowAspiration can be silent.Nursing Best Practices12A present or absent gag does not predictor rule out dysphagiaor aspiration.4
26/05/2017Dysphagia—negative outcomes Dehydrationmalnutritionskin breakdowndelayed rehab independence QOLaspiration pneumoniadeathDysphagia & stroke50% of stroke patients havedysphagia in the first few daysafter the stroke.Of these, 1/3 have swallowingdifficulties that persist beyond3 months post-onset.15Dysphagia & strokeBilateral,subcortical orbrainstem stroke60-70%Unilateralhemisphere stroke15%5
26/05/2017Dysphagia & pneumonia33% of patients withdysphagia developpneumonia requiringtreatment.Stroke & pneumonia35% of post-stroke deathsare caused by pneumonia.Aspiration on videofluoroscopyhttp://www.youtube.com/watch?v 1sFNMk875586
26/05/2017AspirationDysphagia Poor secretion AspirationManagementAspirationAspiration & Poor oral hygiene Pneumonia7
26/05/2017Why oral care?Pathogens that causeaspiration pneumonia (as wellas VAP) can colonize theoropharynx of critically illpatients within 48 hours ofadmission.Where doesoropharyngealbacteria endup?8
26/05/2017Why oral care?Most bacterial nosocomialpneumonia is caused byaspiration of bacteria from theoropharynx or upper GI tract.Why oral care?Nosocomial pneumoniaaccounts for 10-15% of allhospital acquiredinfections.Why oral care?Treatment with oral hygienealone can reduce occurrence ofpneumonia in older adults innursing homes by 30%.9
26/05/2017Why oral care?Patients who haveswallowing difficulties areat risk for poor oralhygiene and aspiration.Oral CareScreen stroke patients onadmission for obvioussigns of dental disease,level of oral care, andappliances.Oral care—considerationsIndependent?Needs help?Dependent?10
26/05/2017Oral care—considerationsOral care—considerationsCognition & LOCActivity toleranceUE functionHandednessOral motor functionSeverity of dysphagiaNPO?Patients who cannot eator drink have the highestoral care needs.What to do?11
26/05/2017Swabs are for moistureand relief—not forcleaning teeth.Suction at bedside12
26/05/2017Suction toothbrushH2O13
26/05/2017Dentures need cleaning too.Best practice guidelines final comment 14
26/05/2017Thickened fluids not a panacea 15
hygiene and aspiration. Oral Care Screen stroke patients on admission for obvious signs of dental disease, level of oral care, and appliances. Oral care—considerations Independent? Needs help? Dependent? 26/05/2017 11 Oral c