Transcription
CT Protocols for Common Primary Care DiagnosesLacey J. McIntosh DO, MPHUniversity of Massachusetts Medical CenterUNECOM 2014CME Program/Reunion and Alumni Weekend:Primary Care in Today’s Changing Practice EnvironmentOctober 10-12, 2014University of New England Biddeford Campus
CT Protocols – IV Contrast Indications– Mass/malignancy/staging– Arterial phase May require a special multiphaseprotocol–––– Contrast has not yet reached theorgan, in arteries only– *Portal venous ams Organ has perfused, contrastreturning through venous system– Delayed phase Equilibrium state where contrasthas returned to venous system,beginning to be renally excreted Contraindications– Allergy– GFR 30 ( 45)– Caution in hypertension,diabetes, renal transplant, singlekidney, CRD Not needed––––2 Organ sizeFollow renal stonesHerniaRetroperitoneal hemorrhageCT Protocols Imaging Phases Affected by cardiac function,anatomy, and physiology
Renal Function Guidelines In the outpatient setting, the followingpatient population will require renalfunction screening within 30 days ofcontrast administration:Age 65 yearsHistory of renal disease, including ––––– Kidney transplantSingle kidneyKidney cancerKidney surgeryHistory of renal insufficiencyHistory of hypertension requiringmedical therapyHistory of diabetesMetformin (or metformin-containingdrug combinations) 3 CT Protocols eGFR 60(very low risk)No restrictionseGFR 45-60(low risk)If acute renal failure, consider IV hydration.Otherwise, encourage oral hydration andsalt loading as clinically appropriate.eGFR 30 – 44(moderate risk)Consider alternative exams (MRI/Ultrasound).Otherwise IV hydration required (seebelow) unless documented that medicalemergency precludes hydration. Iodixanol(Visipaque) contrast is suggested.eGFR 30(high risk)No IV contrast unless approved by nephrologyor deemed a medical emergency, whichmust be documented. Iodixanol(Visipaque) contrast is suggested in theevent of a documented medicalemergency/override authorizing theadministration of IV contrast.
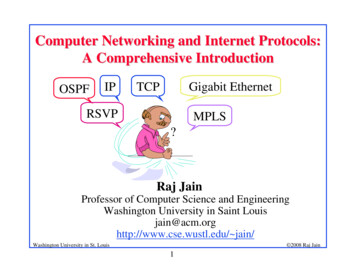
Organ evaluationIndication: “stone”4 CT Protocols PyelonephritisNormal
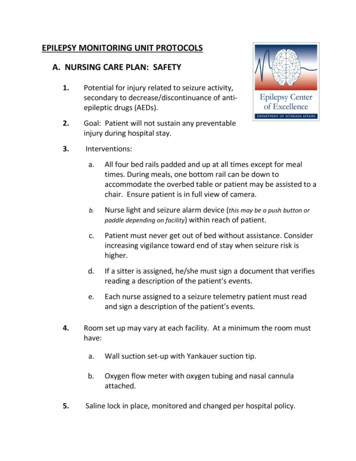
Mass evaluationIndication: “early satiety”5 CT Protocols Extra-adrenalPheochromocytoma
CT Protocols – Oral Contrast Indications - Body– Mostly for us to identify bowel From other structures Evaluate wall– VolumenBladder Contrast– Fistula– Bladder wall integrity Rectal Contrast– Fistula– Post surgical– Penetrating trauma– Functional– Evaluate gastric bypass– Post surgical is a must! Gastrograffin Contraindications– Intolerance– Will obscure your finding Not needed– Angiograms– Organ specific exams6 CT Protocols “Size Matters” Things are different in the ERsetting
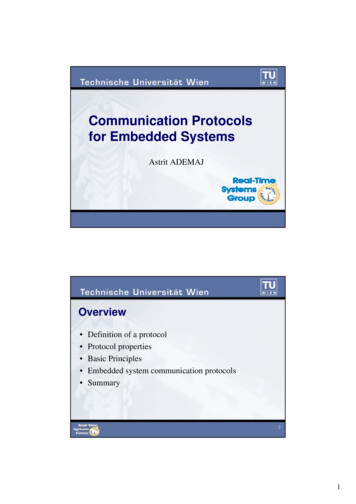
Early Acute AppendicitisNo Oral Contrast7 CT Protocols
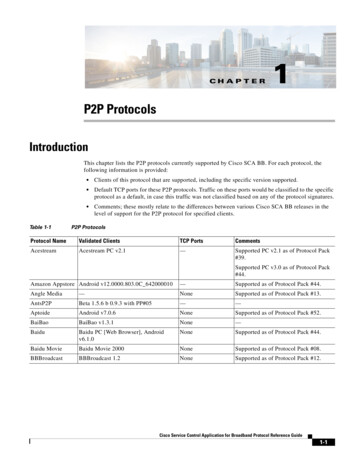
Early Acute AppendicitisWith Oral Contrast8 CT Protocols
Late Acute AppendicitisWith Oral Contrast “Internal Contrast”9 CT Protocols
CT Abd/Pelvis I “Routine” 1 scan: Portal Venous Indications: Evaluate visceral organ Pain Unsure NOT optimal for looking atarterial anatomy or forocclusion (mesenteric ischemia)Acute PancreatitisNecrosisSplenic Vein Thrombus10 CT Protocols
Acute, UncomplicatedDiverticulitis11 CT Protocols
Complicated Diverticulitis withGas-Containing Abscess12 CT Protocols
Acute Cholecystitis13 CT Protocols
CT Abd/Pelvis I- or KUB 1 scan: Noncontrast Indications: Contrast is not necessaryto see the findings– Retroperitonealhemorrhage– Kidney stones– Organ size– Hernia Contrast might obscureyour finding– Hepatic steatosis Patient cannot havecontrast14 CT Protocols Splenomegaly (Lymphoma)
CT Liver I-/I 4 scans: Noncontrast, Arterial Portal Venous, Delayed Indications: Should be considered in any patient with cirrhosis– HCC detection or follow up– Characterization of previously detected liver mass (seen on US,Routine CT A/P)– Follow up ablation or TACE Consider including pelvis if first time or looking for ascites15 CT Protocols
ArterialNoncontrastHepatocellular Carcinoma16 Portal Venous Delayed
ArterialNoncontrastMassive Infiltrating Hepatocellular Carcinoma17 Portal Venous Delayed
ArterialNoncontrastCholangiocarcinoma18 CT ProtocolsPortal Venous Delayed
ArterialPortal VenousDelayedHemangiomasArterial19 CT Protocols
CT Pancreas I-/I 3 scans: Noncontrast, Arterial, PortalVenous Indications: Not appropriate for screening forpancreatic mass or for acutepancreatitis– To characterize a previouslydetected uncharacterized pancreaticlesion, surgical planningNoncontrast Resectability– Involvement of regional arteries andveinsPancreatic carcinomaWith encasement of the SMAArterial20 CT Protocols
CT Renal Mass I-/I 3 scans: Noncontrast, Arterial, PortalVenous Indications: Not appropriate for screening– To characterize a previouslydetected renal lesion Does not include a delayed phase, soit is not optimal for looking atcollecting system abnormalities ordetecting TCCNoncontrastRenal Cell CarcinomaArterial21 CT Protocols
CT Urogram I-/I 2 scans: Noncontrast, ComboNephrographic/Excretory Indications: Optimized study to look at renalparenchyma AND collectingsystem– Microscopic hematuria– Detecting transitional cellcarcinoma (TCC) Not good for looking at renal(parenchymal based) mass orindeterminate cystsTransitional Cell Carcinoma22 CT Protocols
23 CT Protocols
24 CT Protocols
25 CT Protocols
Other Body CT Protocols CT Enterography I O Volumen– 1 scan: Portal Venous– Indications: Crohns/IBD Malabsorption Renal Donor Protocol I-/I – 3 scans: Noncontrast, Arterial, Venous Liver Donor Protocol I-/I – 3 scans: Arterial, Venous, Delayed CT Colonography I-/O /CO2 – 2 scans: O prone and supine after previous day bowel prep
Thoracic Imaging27
CT Chest I- “Routine” 1 scan: Noncontrast Indications: Pneumonia/Atelectasis Emphysema Pulmonary nodules Pleural effusions Special scenarios: Low dose nodule f/u High resolution for interstitiallung disease More scans(supine/prone,inspiratory/expiratory)28 CT Protocols Pneumonia
CT Chest I “Routine” 1 scan: Portal Venous Indications: Mass/Malignancy Especiallylymphadenopathy Initial sarcoid Empyema Pulmonary artery size Not good for looking for PE (toolate)Empyema29 CT Protocols
Hilar Lymphadenopathy inSmall Cell Lung Carcinoma30 CT Protocols
Lymphoma31 CT Protocols
Carcinoid Tumor32 CT Protocols
Metastatic Anaplastic Thyroid Carcinoma33 CT Protocols
CT Chest I PE Protocol 1 scan: Late Arterial (often done by bolus tracking) Indications: Pulmonary embolus Not good for looking at organs – contrast has not made it there yet34 CT Protocols
Saddle Pulmonary Embolism35 CT Protocols
Other Thoracic Protocols Cardiac studies (depending on availability) May be gated May require beta blocker tx Valves Anatomy Coronary Artery Evaluation36 CT Protocols
CT Angiograms CTA Stent I-/I No oral contrast– 3 scans: Noncontrast, Arterial,Delayed– Indications: CTA Aneurysm I-/I – 2 scans: Noncontrast, Arterial– Indications: Aortic aneurysm evaluation Acute bleed (liver, bowel,spleen, etc)– 3 scans: Noncontrast, Arterial,Portal Venous– Indications: Aortic dissection– Portal venous phase is includedto assess organ perfusion CT Protocols– Delayed phase to look fordelayed leak CT Extremity Runoff I-/I – 2 scans: Noncontrast, Arterial– Indications: CTA Dissection I-/I 37 Evaluate endovascular repair Cold limb, extremity ischemia– Large field of view gives poorspecial resolution– Usually ordered by vascularsurgery
Neuro38
CT Head I 1 scan: Noncontrast Indications: Almost always the firstline evaluation Acute trauma, suspectedhemorrhage, stroke Seizures, apnea, syncope,ataxia Workhorse of head CTMCA Infarct39 CT Protocols
Traumatic Hemorrhage40 CT Protocols
Venous Sinus Thrombosis41 CT Protocols
CT Head I 2 scans: Noncontrast,Contrast– Almost always do inADDITION to I- Indications:– Mass– Infection Can obscure smallhemorrhageDifferent from CTA Head(stroke) Abscess42 CT Protocols
CT Cervical Spine I 1 scan: Noncontrast Indications (bone):– Neck pain (DJD)– Post trauma– Post operative Not good for looking at thesoft tissues of the neckCompression Fracture43 CT Protocols
CT Neck I 1 scan: Portal Venous Indications:–––– MassMalignancyInfectionLymphadenopathyStill see cervical spineDifferent from CTA Neck (for stroke ordissection)Branchial Cleft Cyst44 CT Protocols
CTA Head and Neck I 2 scans: Noncontrast head; Arterialthrough the head and neck Indications:– *Stroke– Dissection– Post traumatic 45Different from CT Head and Neck I CT Protocols
Other Misc Neuro Exams CT Nasal Bones I– Trauma CT Sinus/Maxillofacial I– I if looking for infection/abscess, neoplasm CT Temporal Bones I– Hearing loss, cholestatoma, post surgical CT Parathyroid I – 4D parathyroid CT for parathyroid adenoma46 CT Protocols
Musculoskeletal Protocols For bone, contrast doesn’t add much– Only use I if planning to evaluate soft tissues or soft tissue component CT is best for bone– If concerned for soft tissues, MRI is far superior Ultrasound may be a good place to start (insurance issues)47 CT Protocols
Thank You! Please feel free to contact mewith any questions about thispresentation, CT protocols, orradiology in general! lacey.mcintosh@gmail.com48 CT Protocols
Helpful References ACR Appropriateness ateness-Criteria49 CT Protocols
CT Protocols for Common Primary Care Diagnoses Lacey J. McIntosh DO, MPH University of Massachusetts Medical Center UNECOM 2014