Transcription
In the‘Golden Hour’Combat Casualty Care Research drives innovation to improvesurvivability and reimagine future combat careby Col Todd E. Rasmussen, Dr. David G. Baer, RADM Bruce A. Dolland MG Joseph Caravalho Jr.ADVANCING EN ROUTE CAREKnowledge and materiel solutions from military-specific, requirements-driven trauma researchpromise to improve survival and recovery after combat injury. Part of this effort will be toinnovate for Level II and III care aboard transport vehicles on land, air or sea or within localstructures of opportunity. (Photo courtesy of USAMRMC)80Army AL&T MagazineJanuary–March 2015
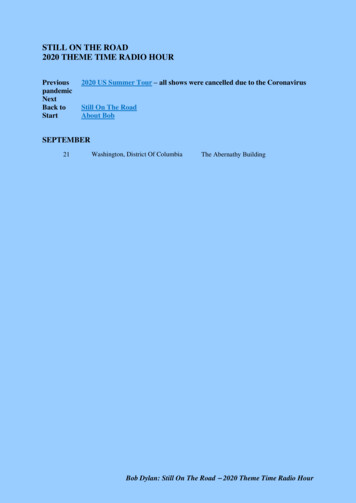
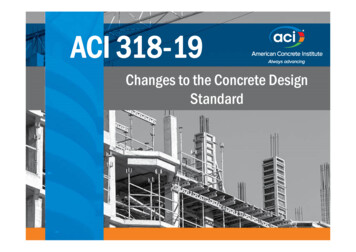
SCIENCE & TECHNOLOGYLUNG SUPPORTExtracorporeal (i.e., outside the body)membrane oxygenation (ECMO) technologyprovides a circuit to replace lung function inseverely injured casualties, such as the oneshown here. ECMO support machines exist orare being developed through combat casualtycare research. Older versions of these artificialorgan support machines were much larger andmore invasive, and required more personnel tooperate them. Discovery and innovation in thisarea of research will support the use of evensmaller, more autonomous units in forward, outof-hospital environments, including field anden-route care. (Photo by Lt Col Jeremy Cannon,M.D., U.S. Air Force Medical Corps)The burden of injury among U.S. service personnelduring the wars in Afghanistan and Iraq confirmedthe benefit of requirements-driven medical researchaimed at reducing combat-related mortality andimproving survival. While elements of trauma research existedbefore these wars, they were small, service-focused and not fullycoordinated. The wars also exposed the often overlooked factthat, unlike research in the areas of cancer, cardiovascular disease and behavioral health, the nation has no federal institutes orprivate foundations dedicated to funding trauma research. Thesacrifices of our men and women in uniform have re-emphasizedthe lesson that combat casualty care research is a military-specific imperative; there is no safety net in this endeavor.With this in mind, the U.S. Combat Casualty Care ResearchProgram (CCCRP) is charged with driving innovation in traumacare to support Force 2025 and Beyond. Central to this effort isa reappraisal of the time between injury and life- sustaining medical treatment—known as the “golden hour” standard. In the past,the end of the golden hour was marked by the time a patientarrived at a fixed facility or traditional echelon of care. Now thatadvanced resuscitative capability can be pushed closer to the pointof injury, regardless of setting or location, we must redefine thegolden hour end point. (See Figure 1 on Page 82.)CCCRP PS AND QSThe CCCRP guides the nation’s rejuvenated investment inrequirements-driven military trauma research. The program,co-located at Fort Detrick, MD, and the Defense HealthHeadquarters, Falls Church, VA, plans, programs, budgetsand oversees the execution of approximately 300 million inrequirements-driven research aimed at producing knowledgeand materiel solutions for the full spectrum of military traumacare, including at the point of injury, en route in rotary andfixed-wing transport, and in Level II through Level V facilities.The CCCRP’s primary task is the oversight and management ofscience and technology elements of funding. However, its staffand processes are integral to the life cycle of research, including the advanced development and acquisition of knowledgeand materiel and their relevant implementation in the practice of combat casualty care. The mission of the CCCRP isto produce solutions that improve survival and recovery fromcombat-related injury, and thereby empower and sustain thefighting force.The program staff resides within the Research Area Directorate –2 (RAD-2) of the U.S. Army Medical Research and MaterielCommand (USAMRMC) and the Research, Development andAcquisition Directorate of the Defense Health Agency (DHA).A S C . A R M Y. M I L81
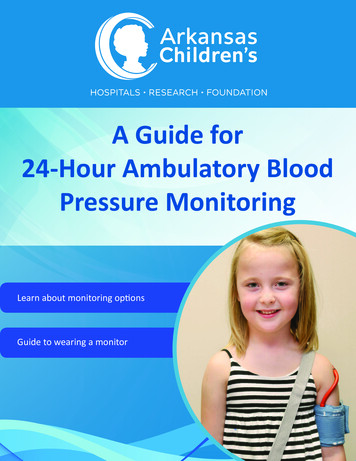
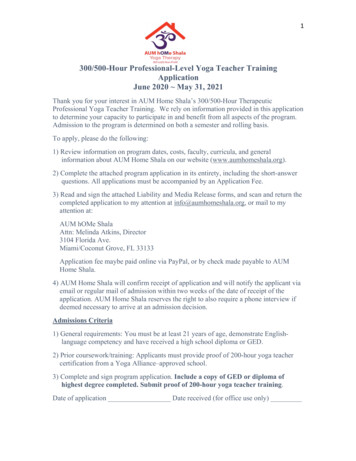
IN THE ‘GOLDEN HOUR’FIGURE 1In this construct, the CCCRP guidesand advises the investment of core Armyappropriations and Defense Health Program (DHP) research, development, testand evaluation (RDT&E) dollars.Research takes place at two ofUSAMRMC’s subordinate labora tories—the U.S. Army Institute ofSurgical Research at Joint Base SanAntonio, TX, and the Walter Reed ArmyInstitute of Research in Silver Spring,MD—and at civilian academic institutions and medical centers across thecountry, which conduct most of the workfunded by the DHP.EVOLUTION OF THE GOLDEN HOURThe traditional (pre-2015) concept of the golden hour is based on movement of the injured personto a fixed location or echelon of care within 60 minutes. The evolved concept for 2015 andbeyond involves delivering advanced resuscitative capability to the injured person within one hour,regardless of location or echelon of care. (SOURCE: Col Todd E. Rasmussen, USAMRMC CCCRP)FIGURE 2‘BOOKENDS’ TO RESEARCHThe JTS provides “bookends” for the CCCRP. On the left side, the JTS and clinical communityprovide observations and questions that the research program endeavors to answer withknowledge and materiel solutions. On the right side, the JTS and clinical community take, honeand integrate the results of that research to develop best practices and clinical guidance forcombat casualty care. (SOURCE: Col Todd E. Rasmussen, USAMRMC CCCRP)82Army AL&T MagazineJanuary–March 2015The CCCRP’s blended Army RAD-2and DHA staff is positioned to maximizecoordination of effort among the Army,Navy and Air Force and to create synergyamong the different contributors to themedical RDT&E investment. Throughactive program management, theCCCRP also aims to leverage traumarelated research dollars stemming fromcongressional special interest programsto maximize the Army and DHA investment. This multifaceted funding supportsthe advancement of groundbreakingtrauma research through a requirementsdriven, coordinated program structure.A THREE-PART DYNAMOThe effectiveness of the nation’s investment in combat casualty care researchis evident in the 50 percent decline incase fatality rates among U.S. servicepersonnel in Afghanistan between 2005and 2013. Evidence also exists that theresearch funded by the CCCRP has beeneffective in narrowing gaps established byDOD’s 2008 Guidance for the Development of the Force, meeting the high-levelstrategic goals of the military. Additionally, the impact is expanding beyond themilitary, as lifesaving advances in traumacare increasingly are being translated to
SCIENCE & TECHNOLOGYHELO HOSPITALSPC Giles Dunlop, a crew chief, raises a simulated casualty into his aircraft June 19, 2014, duringa personnel recovery exercise in Kuwait involving a UH-60 Black Hawk of 1st Battalion, 214thAir Ambulance, 42nd Combat Aviation Brigade (CAB) and a Kuwaiti Air Force SA 330 Pumahelicopter. The CCCRP’s research spans the full spectrum of military trauma care, including at thepoint of injury, en route in rotary and fixed-wing transport, and in Level II through Level V facilities.(New York Army National Guard photo by SGT Harley Jelis, 42nd CAB)the civilian setting, benefiting traumapatients across the country.These successes have been made possibleby integrating the CCCRP with its usercommunities, chief among them the U.S.Joint Trauma System (JTS). The JTSis DOD’s “go-to” entity for coordinating and optimizing trauma care in theoperational environment. Formalized asa Defense Center of Excellence, the JTSalso maintains the DOD Trauma Registry, the largest repository of combat injuryand injury management information inhistory. In this capacity, JTS and the processes it supports generate many of theclinical questions or requirements thatneed answers from research, and document the efficacy of innovations in care.Conceptually, experts have referred tothe JTS as “bookends” holding up eitherside of the medical research program.(See Figure 2.) On one side is the JTS’ability to identify and feed relevant gapsin treatment into the research program,which then endeavors to provide knowledge and materiel solutions to resolvethose gaps. The other is JTS’ ability toreceive, vet and integrate outcomes fromthe research program, be they knowledge or materiel solutions. The result hasbeen that JTS has established, and nowmaintains, more than 30 evidence-basedclinical practice guidelines.The relationship between CCCRP andJTS is an important construct and a lessonfrom the wars. The requirements-drivenRDT&E program bridges the chasmthat otherwise would exist between thebookends of clinical questions or needson one side, and evidence- and materielenabled clinical practice on the other.The swift translation of evidence fromthis sizable research program throughJTS to the battlefield represents a first inmilitary history.REDEFINING THEGOLDEN HOURWhile no one can predict the future ofcombat casualty care, it is prudent toassume it will play an important role inU.S. national security in the years ahead.Just as the world has become more complex from a geopolitical standpoint,anticipating the future of combat casualty care has also become more complex.In 2015, the CCCRP finds itself pressedfrom three sides to consider and developsolutions in a variety of combat injuryscenarios, including: A limited number of troops executing counterinsurgency operations inremote locations. Large, conventional troop formationsconducting operations in a Pacifictheater. Troops deployed and conducting combat operations in large urban areas (i.e.,mega-cities).A S C . A R M Y. M I L83
IN THE ‘GOLDEN HOUR’FIGURE 3Looking ahead to potential scenarios,CCCRP must ensure that medical innovation rises to the challenge by providingflexibility to combatant commandersregardless of operational complexities—for example, anti-access and area denial,prolonged field care, long-distancemedical evacuation or large volumes ofcasualties.In this effort, the program must bewilling to turn the doctrine of fixed ortraditional echelons of care on its sideand innovate for scenarios in which LevelII and III care is performed aboard transport vehicles (land-, air- or sea-based) orwithin local structures of opportunity.In such circumstances, field care may beprolonged, lasting for days or even weeks.Combat casualty care research withthese complex scenarios in mind promises to enhance resuscitative capabilityfor injured service personnel regardlessof environment, leveraging communications networks (i.e., telementoring) andtargeted resupplies of materials. In thefuture, CCCRP must focus on transforming the concept of the golden hourinto one bound not by the time to reachtraditional echelons of care or fixedfacilities, but the time until enhancedresuscitative capability can be deliveredto the injured troop, regardless of location or need for transport.Within CCCRP are five portfolios withlines of effort that aim to drive medicalinnovation. (See Figure 3.) In these, theprogram works to provide solutions totransform the golden hour and improvesurvival, lessen the medical logisticalrequirement and afford agility to thefuture joint force.DIRECTING INNOVATIONThese portfolios and lines of effort in which the CCCRP aims to drive medical innovation areintended to produce solutions that will not only transform the golden hour and improve survival,but also lessen the medical logistical requirement for the future joint force. (SOURCE: Col Todd E.Rasmussen, USAMRMC CCCRP)84Army AL&T MagazineJanuary–March 2015The medical RDT&E planned in theseportfolios is aimed at re-establishing andsustaining optimal physiology, regardless of the location of care. The resulting
SCIENCE & TECHNOLOGYsolutions aim to provide continuousresuscitative, intensive, definitive andrecovery care that is mindful of, butnot constrained by, complexities ofthe operational environment. Militarytrauma research, development and acquisition play a vital role in responding tothe unique needs of injured U.S. servicepersonnel in current and future combatscenarios. They empower and sustain thefighting force and improve the flexibilityof combatant commanders while augmenting national security.CONCLUSIONThe CCCRP’s uniquely “top-down,”requirements-driven medical researchis recognized nationally as an effective alternative to other federal entitiesthat fund investigator-initiated researchwithout specific urgency. CCCRP isessential, as no other entity—federal orprivate—funds trauma research. As theprogram sets its eyes on 2025 and beyond,including reappraisal of the golden hour,its efforts will continue to be patient- andphysiology-focused, aimed at developingsolutions to meet warfighters’ needs andenable an agile joint force in future combat missions.For more information, review the followingjournal articles and links: “Where do we go from here?”—Journal ofTrauma and Acute Care Surgery (http://journals.lww.com/jtrauma/), Vol. 75,Issue 2. “Military trauma system in Afghanistan:lessons for civil systems?”—Current Opinion in Critical Care (http://journals.lww.com/co-criticalcare/), Vol. 19,Issue 6. “Implications of combat casualty care formass casualty events”—The Journal of theAmerican Medical Association (http://jama.jamanetwork.com/), Vol. 310,No. 5.THE STUFF OF LIFEFrench lyophilized plasma, a freeze-dried product developed by the French military with U.S.military technology, has helped to successfully resuscitate critically injured U.S. Special Forcescombat casualties. Such innovations can transform the meaning of the golden hour. (Photo bySteven Galvan, USAISR Public Affairs) JTS & CCAT [critical care air transport] Clinical Practice Guidelines,http://www.usaisr.amedd.army.mil/ clinical practice guidelines.html.COL TODD E. RASMUSSEN (USAF) isdirector of the CCCRP, Fort Detrick, MD.He has an M.D. from Mayo Medical Schooland a B.S. in pharmacy and premedicalstudies from the University of Kansas. Hehas American Board of Surgery certification in general surgery and vascular surgery.He served as deputy commander of theU.S. Army Institute of Surgical Research(USAISR) from 2010 to 2013.DR. DAVID G. BAER is deputy director ofCCCRP. He holds a Ph.D. in genetics andmolecular biology from the University ofHawaii and a B.S. in biology from TrinityUniversity. His previous assignments includeactive-duty Army service as a research scientist at USAISR, where his work focusedon improving treatment for combat-injuredSoldiers. He is Level III certified in science and technology management and is amember of the Army Acquisition Corps.RADM BRUCE A. DOLL is deputy commander of USAMRMC, Fort Detrick, MD,and director of the Research, Developmentand Acquisition Directorate of the DHA,Falls Church, VA. He has a D.D.S. degreefrom the State University of New York atBuffalo School of Dentistry, an executiveMBA from the Naval Postgraduate Schooland an undergraduate degree from ColgateUniversity. He is a diplomate of the American Board of Periodontology.MG JOSEPH CARAVALHO JR. is thedeputy surgeon general and deputy commanding general of the U.S. Army MedicalCommand, Washington, DC. He has a Master of Strategic Studies from the U.S. ArmyWar College, an M.D. from the UniformedServices University of the Health SciencesSchool of Medicine and a B.A. in mathematics from Gonzaga University. He holdscurrent certification in nuclear cardiology.Before assuming his current role, he servedas commanding general of USAMRMC.A S C . A R M Y. M I L85
the research program, be they knowl-edge or materiel solutions. The result has been that JTS has established, and now maintains, more than 30 evidence-based clinical practice guidelines. The relationship between CCCRP and JTS is an important construct and a lesson from the wars. The requirements-dr