Transcription
GRADUATE PROGRAM IN PUBLIC HEALTHThe Director’s ColumnDr. Nils Hennig, Program DirectorA Happy New Year and a heartfeltwelcome to our new students.You are most welcome! The GraduateProgram in Public Health at theIcahn School of Medicine at MountSinai is dedicated to improving thehealth of communities and individualsand is based on the core values ofcommunity, sound science, diversity,social justice and engagement.I am excited to share with you this new issue of The Scoop.Learn about how our students and partners care and arepromoting public health and our core values. Our NGO partnerat Soft Power Health describes the threat of development tothe communities and the fragile ecosystem of the White Nile inUganda; one of our students writes about her prevention workon diarrheal illness in rural Uganda; another student reflects onaddressing child malnutrition in Haiti; learn about our program’snew offering in environmental exposures, risk and public health;get some insight on the Delivery System Reform IncentivePayment Program (DSRIP); learn about Mount Sinai’s Lab100— a cross between a wellness center and data collectingsoftware; and review our first annual Public Health ProfessionalDevelopment Conference and the latest Public Health GrandRounds focusing on Native American health and sovereignty.At the end of 2018, the National Center for Health Statisticsreported that, between 2016 and 2017, US life expectancycontinues to fall, making it the third consecutive year theUS has seen a decrease in life expectancy. Drug overdosesand increasing inequality are the main drivers of this trend.Reflecting on the last year, we have seen multiple additionalthreats to the public’s health from the current administration.It is actively rolling back policies that aim to curb climatechange and limit environmental pollution, and generallythreatens to cut federal funding for science and theenvironment. The administration is naming to the courtsopponents of reproductive freedom, food safety, workers’rights, gun safety and other important public health issues.On our southern border it has created a separation crisis,threating the well-being of migrant families. On a global level,the current administration tried unsuccessfully to block aWorld Health Assembly resolution encouraging governmentsto promote breastfeeding among their citizens. In addition,FALL 2018/WINTER 2019 – Issue 11it intended to remove from the resolution languagerecommending that countries curb the promotion of foodproducts that may undermine the health of young children,and threated the resolution’s sponsor, Ecuador, with economicpunishment if the changes were not approved. (It is only afew years ago that the Surgeon General’s Call to Action toSupport Breastfeeding reviewed the data on the practice andconcluded: “Breast milk is uniquely suited to the human infant’snutritional needs and is a live substance with unparalleledimmunological and anti-inflammatory properties that protectagainst a host of illnesses and diseases for both mothersand children.” A 2016 Lancet study found that universalbreastfeeding would save the lives of more than 800,000children a year, and generate about 300 billion in savingsfrom better economic outcomes and lower associatedhealthcare costs.)This administration is prioritizing private interests over thepublic good, putting the interests of wealth and industry first.These greed-driven policies that attack the structures thatkeep our air and water clean, our workplaces safe, and oureconomy fair, have dire consequences for our health. Healthis a product of our collective investment in improving thesocial, economic, and environmental conditions in which welive. When we neglect this investment and place the profitsof a few over the well-being of all, we invite poor health forourselves, our families and future generations.My main goals for the new year are to continue to supportour students in tackling the challenges of the present momentand provide them the tools needed to help create a morejust society that generates health for all. There is plenty ofwork ahead.At the end of 2018, the National Centerfor Health Statistics reported that,between 2016 and 2017, US lifeexpectancy continues to fall, makingit the third consecutive year the UShas seen a decrease in life expectancy.
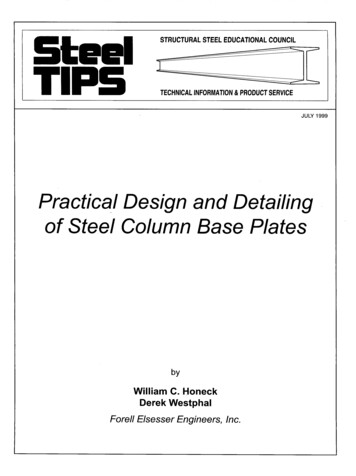
Save the White NileBy Jessie Stone, MD, Founder and Director of So Power HealthThe Nile is Africa’s most important river. It supports at-risk communities andfragile ecosystems. It is also Uganda’s most precious natural resource.As a pathway to development, large hydro-dam projects in thedeveloping world have received vast investment. Presently,the government of Uganda, with the support of the World Bank,is constructing a series of five large hydro-dams on the Nile.The second of these projects, known as The Isimba Dam, isnearing completion.Hydro-dam projects in Africa also increase the burden ofschistosomiasis, a parasitic infection that relies on human andsnail hosts to complete its life cycle. Schistosomiasis is foundthroughout the Nile River, where local people come to bathe,wash clothes, collect drinking water and swim. Schistosomiasis,like malaria, may be fatal if untreated. Unlike malaria it has aslow, insidious and debilitating progression, principally infectingthe liver, before ending in death.Photo: The Isimba DamHistorically, countries building large dams are laden withenormous debt that they can never repay. An Oxford Universitystudy of 235 large-scale hydroelectric projects built since 1934revealed average cost overruns of 90%. Countries like Ugandarely on the World Bank and recently, China, for financing thesedams. But once built, these projects struggle to generate enoughmoney to repay the debt they create. Numerous examples of thesefailures dot the landscape throughout Africa, South America,China, and Indonesia. Uganda’s experience with the BujagaliDam (completed 2012) and now Isimba, has put them on thispath. Currently over-budget and behind its projected completiondate, Isimba has been plagued by poor construction, impropermaterials and staffing problems.In one of the great ironies of development, the electricitygenerated by these mega dams is rarely affordable for those whoare most in need. Instead, it is exported and sold as profit for thegovernment and dam financiers.It has been well-documented that reservoirs formed bylarge dams in sub-Saharan Africa increase malaria rates insurrounding areas. In Uganda, malaria is the biggest infectiousdisease killer in the country. Over-burdened Ugandan hospitalsare swamped with cases of malaria, and the disease kills morepregnant women and children under five than any other. Damslike Isimba are massive reservoirs, providing ample breedinggrounds for mosquitos that carry malaria.2Photo: A local resident wades in the Nile River.With the completion of the Isimba Dam, rates of malaria andschistosomiasis will skyrocket in a portion of Uganda’s mostin-need population as well: rural poor residents already sufferingfrom malnutrition. Increasing the burden of these diseasesin people suffering with malnutrition will have disastrousconsequences on their ability to survive.Of the 33,000 people treated last year at the So Power HealthClinic I founded and have run since 2006, 20% of the patientshad malaria, schistosomiasis or malnutrition. Children arethose most affected by malnutrition and malaria. Many of thesepatients come from areas soon to be flooded by Isimba.Furthermore, these communities have received no compensationfor their homes and livelihoods that are soon to be lost. Researchshows that displaced people never recover their standard of living— even when compensated. These are the same people that thehydroelectric power generation is supposed to be helping develop.With no obvious positive benefit to the majority of Ugandans, andwith the surety that many will be worse off a er the dam, why isthe World Bank continuing to push large dam projects?continued on page 3
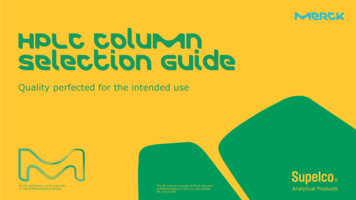
Water, Diarrheal Illness, and the Rotavirus VaccineIn Rural UgandaBy Rana Lamisa, MPH student in the Global Health TrackNama Wellness Community Center, NAWECas known by the staff and residents, islocated along with its sister organization,Komo Learning Center, in the village ofLukojjo, overlooking Kayunga Road. Onthe other side of the road is a steel-gateddoor, behind it — my home for two months.This past summer I worked with NAWECas part of my Global Health SummerExperience. A er days filled with publichealth training and work, I kept my eyesopen. I spent my evenings si ing undera mango tree overlooking the side of theroad people-watching.Within a few days I noticed somethingperplexing. Why was I seeing peoplewalking around with bright yellow plasticcontainers? How come I didn’t have thiscontainer? I saw women from the nearbystores coming to the back of my house,where my neighborslived. Was it a socialvisit or somethingelse? One evening,I saw a group ofchildren walkingon the side of theroad, laughing andcarrying yellowcontainers. I startedasking questionsand quickly figuredPhoto: A child caringout what was goinga “jerry can” in Lukojjoon. The containers,Village in the Mukonocalled jerry cans,District, Uganda.originally filledwith cooking oil, were repurposed for watertransport and storage. I had completelymissed this essential component of the livesof mostly everyone around me because, dueto the rare internal supply of water that wehad at our home, I was not experiencingthis myself.In Uganda, about 21 million people livingin small towns and rural areas lack accessto clean drinking water. A person withlimited or no access to quality water,usually from a protected borehole well ormunicipal supply, will have to go to othersources- such as surface water, unprotectedcontaminated wells, or vendors sellingwater of unknown quality. Unsafe practicesare widespread, and have an especiallydevastating effect on child mortality.My supervisor explained that there weremany pediatric patients showing at theclinic for diarrhea and dehydration. Wasthere a connection between quality ofdrinking water and diarrheal illness? Oneof the most common causes of diarrhea ininfants and young children is rotavirus.It accounts for more than a third ofdiarrhea deaths in children younger thanfive years worldwide, with more than halfof these deaths in sub-Saharan Africa.A new rotavirus vaccine had just beenapproved by the Ministry of Health tobe distributed by NAWEC, and I had theopportunity to investigate. I conducteda baseline survey to assess the need forthe rotavirus vaccine within Nama SubPhoto: A clinic visit set up by Nama WellnessCommunity Center and the Komo LearningCenter.County. I inquired about the source ofdrinking water within households andwhether the vaccine had been administeredto children in these households. I amcurrently working on statistical analysisof the data. I also worked on designinga program for rotavirus administrationwithin NAWEC’s catchment area of villagesand at the clinic. My curiosity gave meinsight into a significant issue within thelives of Ugandans that connects waterquality to illness. While be er measuresneed to be in place to ensure clean water,the implementation of the rotavirus vaccineallows for protective measures to be takenagainst diarrheal illness. I plan to return toUganda this year, so that I can continue thisproject and continue to contribute to thehealth of this community.Save the White Nile (continued from page 2)Brazil’s decision halting its Amazon River mega hydro-damshould show the World Bank and the government of Uganda anew way forward. As the equator runs through Uganda, Ugandacould concentrate on developing solar energy fields as anaffordable alternative to hydropower.Last year, the World Bank agreed to let the protected KalagalaOffset Area be flooded by Isimba’s reservoir. This unique cultural,spiritual, and biodiverse area on the Nile was created by the WorldBank and the government of Uganda in order to move forwardwith hydroelectric plans. Once gone, it will be irreplaceable.The time has come for the World Bank to stop financingcatastrophic hydro-projects and honor its original charter toli at-risk populations out of poverty, enabling them to leadhealthy and productive lives. In Uganda, they must responsiblycompensate these vulnerable populations. If the World Bankwon’t stand for the defenseless, who will?Visit .savethewhitenile.org, click on the petition, and let yourviews be known. You will be standing for the thousands that haveno voice.3
Addressing the Child Malnutrition Crisis in HaitiBy Naissa Piverger, MPH Student in the Health Promotion & Disease Prevention TrackI was born in Haiti, on a small farm where I lived with mygrandparents. I speak the languages and understand what itmeans to live below the poverty line. We had limited resourcesand lacked the necessities, but my grandmother managed tofeed us and her neighbors. Fast-forward seventeen years: myparents and I immigrated to the United States for a be er life.Unfortunately, through the years, I have had to watch, o enhelplessly and from a distance, as natural and man-madecalamities made the people in my birth country suffer. Today,Haiti is the poorest country in the Western Hemisphere. Foodis scarce and residents suffer from extremely high infant andmaternal mortality rates.A er the 2010 earthquake, I went home to visit my countryand witness the a ermath. There, I noticed a womanwith a shawl wrapped around her body, walking toward mygrandmother’s shack.I became curious andfollowed her inside. Shehad come to pick somevegetables my grandmotherhad planted in the garden.She turned around,surprised to see me. “Mygoodness! Look how tallyou’ve grown,” she said.I smiled and hugged her,noticing the small babyswaddled in the shawl.Marie is a mother of seven kids — three of whom are not herbiological children. She was taking care of them because herfriend trusted her to do so shortly a er her death. Marie confidedin me about the struggles to feed and maintain the health of herchildren. She explained that there were hundreds of women inher position — uncertain of when their next meal will be. I hadthe pleasure of meeting these women, who lived in an enclosedcorridor protected by a piece of bed sheet, functioning as thedoor. The women said they rely on the unpredictable rainyseason and never lose faith in God.According to the United States Agency for InternationalDevelopment, 22%, or 264,000 Haitian children underfive years, suffer from chronic malnutrition (stunting orlow height-for-age) and 66 percent, or 792,000 children underfive years, suffer from anemia. The country’s political instabilityand intense poverty leave the residents vulnerable to disasters.The poor infrastructure, food insecurity, natural disasters andburden of communicable infections continue to put Haitians atrisk for acute and chronic malnutrition.The mothers that I saw were clearly struggling, in a way notunlike my grandmother had, years earlier working hard to ensurethat I was fed on that small farm. The women of my homeland ofHaiti o en feel beholden to the despair of malnutrition, unsureof what more to do than hold and comfort their own children,and the children who have already lost their own mothers. Itis therefore our duty, as global public health practitioners, torecognize this long-standing issue and continue to tackle it,aiming for improvement and a well-fed population.New Course Offering: Environmental Exposures,Risk and Public HealthBy Sanjana Inala, & Venu Bangla, first-year MPH studentsIn light of Governor Andrew Cuomo’s declaration of Children’sEnvironmental Health Day on October 11th, the call forunderstanding environmental health risks is greater than ever.Open to all MPH students, MPH 0516 Environmental Exposures,Risk and Public Health in the Spring II term, will exploreoccupational and environmental exposure assessment and riskassessment — important topics for the practice of environmentalpublic health.Environmental pediatrician Lauren Zajac, MD, MPH, FAAPand exposure scientist Homero Harari, ScD, MSc, provide aninnovative approach to learning. Lectures focus on communityand occupational case studies of environmental exposures,and also include guest speakers from agencies such as theEnvironmental Protection Agency and the New York City4Department of Health. The class delves into explaining howcommon environmental exposures are identified and measured,and emphasizes the importance of communicating that riskwith communities. Students will have the opportunity to reviewcurrent and relevant exposure scenarios (such as workplacesor community pollution sources) and apply the skills learnedthrough interactive discussions and problem-based assignments.This combined instruction provides a comprehensive methodologyto study environmental health. Moreover, these skills canbe translated into a range of Applied Practice Experienceopportunities from the World Trade Center study to the New YorkCity Department of Health. Join the course to strengthen yourknowledge and understanding of the study of environmentalhealth. These skills will serve as an essential tool in any field!
The Annual Meeting of the AmericanPublic Health AssociationBy Elisabeth Brodbeck, MPH, MA, Associate Director of the Graduate Program in Public HealthThe American Public Health Association,the largest membership organizationrepresenting the public health profession,hosts its annual meeting once a yearin November. More than 13,000 APHAmembers, including faculty, students,staff, and alumni gather to share newresearch and trends in public health inover 1,000 different scientific sessions.Additionally, over 700 exhibitorsrepresent various arenas of public health,including representatives from schoolsand programs of public health. This isan opportune time to learn about bestpractices, advocate for evidence-basedpolicy, and network with peers. Ourprogram is pleased to have a growingnumber of its own students, alumni andfaculty presenting work in areas suchas the mass distribution of insecticidalnets in Uganda and the impact of activedesign in affordable housing. Two MPHstudents were also included in APHA’sStudent Leadership Institute, two full daysof programming dedicated to developingleadership skills in the field. The Programalso hosted a networking reception for allMount Sinai a endees at APHA. We hopemore of you will join us next year.For the last two years I have hadthe pleasure of serving as one of therepresentatives to the Governing Councilfor the Public Health Social Worksection. As the representative legislativebody of APHA, the Governing Councilserves to establish policies and actupon recommendations from the largerorganization’s commi ees and ExecutiveBoard. In an effort to advocate for policiesacross the public health spectrum and toaffect change at the national level, APHAreleases policy statements to guide theorganization. The Governing Council isasked to consider these policy statementsusing evidence-based and scientificmethods of evaluation and vote uponthese statements to form APHA’s policy.Additionally, one of the tasks each yearis for voting councilor members todecide the theme for future meetings.The 2019 Annual Meeting in Philadelphiawill be themed “Creating the HealthiestNation: For science. For action. Forhealth.” A er much debate and narrowingdown of ideas, we can expect the AnnualMeeting in 2020 in San Francisco totackle the themes of violence as a publichealth issue — a critically important andhistorically underrepresented area ofresearch and practice in our field. We areexcited to see the works presented onthese topics. Get those abstracts ready!In the meantime, check out what someof our students have to say about theirexperience at this year’s conference!Highlights“One aspect of APHA that I found surprising was the large number of studentswho a ended. This made me realize that you’re never too young to do research,speak at conferences, bounce ideas off of
Komo Learning Center, in the village of Lukojjo, overlooking Kayunga Road. On the other side of the road is a steel-gated door, behind it — my home for two months. This past summer I worked with NAWEC as part of my Glob