Transcription
The Evolving EPCS Landscape: 2016A Prescription for Stopping Opioid AbuseAn Industry Report Analyzing E-Prescribing Trends and Data from 2015Corporate Headquarters9420 Key West Ave., Suite 101Rockville, MD 20850Toll Free (866) 263-6511sales@drfirst.com West Coast Office916 E. Baseline Rd, Suite 202Mesa, AZ 85204(602) 466-7547www.drfirst.com 2016 DrFirst Corporation. All rights reserved. blog.drfirst.com
The Evolving EPCS Landscape: 2016A Prescription for Stopping Opioid AbuseAn Industry Report Analyzing Prescribing Trends and Data from 2015Table of ContentsChallenges Facing E-Prescribing - The Problem1The State of EPCS Adoption2EPCS Enablement in Retail Pharmacies2EPCS Adoption by Physicians4Why Are Physicians Slow to Adopt EPCS?4The Role of PDMP Interoperability7Key Benefits of E-Prescribing8New York's I-STOP Law8About DrFirst9Practical Powerful Innovation
The opioid addiction crisis has captured the nation’s attention as legislators, law enforcement officialsand healthcare leaders debate solutions to reduce unnecessary or excessive opioid prescriptions, fraud,abuse, overdose deaths, doctor shopping, and drug diversion.Electronic prescribing is one important technology that may prove invaluable in helping to mitigate thiscrisis. While the U.S. Drug Enforcement Administration (DEA) authorized the use of e-prescribing ofcontrolled substances (EPCS) in 2010, U.S. states were slower to adopt. However, state-level legalizationin all 50 states and the District of Columbia was achieved in 2015, putting protocols in place to allow EPCSto help stem drug abuse and misuse.Further, on March 27, 2016, New York will become the first state in the union to enforce a law requiringthat all medications – legend drugs and controlled substances – be prescribed electronically.This industry briefing highlights EPCS trends and advances in 2015, including the contrasting realities ofrapidly increasing EPCS enablement on the part of pharmacies and the disproportionately low rate ofEPCS adoption among the nation’s doctors.E-prescribing – the direct digital transfer of patient prescriptions from provider topharmacy – is a long-accepted practice that has proven to help reduce prescriptionmisuse and enhance patient safety. Nationally, most doctors (70 percent or more,according to the Office of the National Coordinator for Health Information Technology)already transmit most prescriptions electronically. The unfortunate twist is that most ofthose doctors are only e-prescribing non-controlled substances, known as “legenddrugs.” Conversely, electronic prescribing of controlled substances (Schedule II – Vdrugs as defined by DEA) is only used by about 5 percent of doctors nationwide at thistime. And of course, it is the misuse of controlled substances that is driving the epidemicof prescription drug abuse.With pressure mounting on law enforcement, legislators and healthcare providers tostem prescription drug abuse, we envision EPCS, prescription drug monitoring programsand other best practices may finally become mainstream.The State of EPCS AdoptionRetail pharmacies and some practitioners are increasingly embracing EPCS to helpaddress the prescription drug abuse crisis. EPCS eliminates the risk of forged or alteredpaper prescriptions and sets up important safeguards against fraud, “doctor shopping,”Challenges Facing E-Prescribing – The ProblemMore than 15 million people in the U.S. abuse prescription drugs regularly and 52 million Americans over theage of 12 have used prescription drugs non-medically in their lifetime. Accordingly, the U.S. Centers for DiseaseControl has declared prescription painkiller abuse a national “crisis,” and warns that people who takeprescription painkillers can become addicted with just one prescription. Each day, 44 people in the UnitedStates die from an overdose of a prescription painkiller. In 2010, more Americans died from pharmaceuticaldrug overdoses (38,329) from either car crashes (22,134) or firearms (31,672).1Opioid overdose deaths more than tripled between 1990 and 2010. The amount of prescription painkillersprescribed and sold in the U.S. has nearly quadrupled since 1999, yet there has been no overall change in theamount of pain reported. Drug overdoses are now the leading cause of death from injury in the U.S., withnearly 44,000 overdose deaths annually.21 1. www.cdc.gov/drugoverdose/epidemic2. www.cdc.gov/drugoverdoseoverprescribing and improper dispensing of medications due to misinterpretedhandwriting.Because of its value as an important clinical tool, EPCS was first made legal on a federallevel in 2010, under the DEA’s interim final ruling (IFR) legislation. However, EPCS is alsosubject to state legal requirements, and it was not until 2015 that the last of the states inthe U.S. legalized EPCS.EPCS Enablement in Retail PharmaciesRetail pharmacies exhibited accelerated adoption of the technology necessary tofacilitate controlled substance e-prescribing in 2015. Eighty-two percent of U.S. retailpharmacies are now EPCS-enabled, a 21 percent increase over 2014. Further, almost allstates have at least 60 percent of pharmacies EPCS-enabled, and more than half of allstates have more than 80 percent of retail pharmacies ready and able to receive andprocess EPCS orders.33. Pharmacy data from DrFirst’s Rcopia e-prescribing system, CY 2014 CY 2015. All EPCS pharmacy data in this report refers to retail pharmaciesthat are electronically enabled. 2
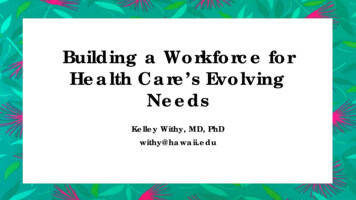
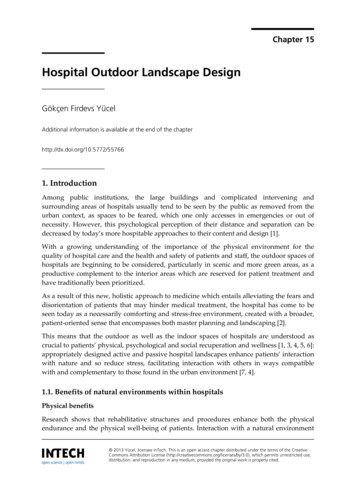
This rapid expansion is driven in part by the increase in EPCS enablement by largestudies on the ratio of prescriptions for narcotic analgesics and medications for narcotic withdrawalnational chains, such as CVS, Walgreens and supermarket-based pharmacies. It’s alsomay provide valuable insight into the safety of these medications.due to increased recognition among pharmacy executives that EPCS is now legal intheir state.EPCS Adoption by PhysiciansGrowth in EPCS-enabled pharmacies nationwide has been followed by an even more dramatic increaseFive states – Massachusetts, Michigan, Oklahoma, Rhode Island and New York – nowin the use of EPCS technology by physicians, albeit across a very narrow subset of prescribers.have 90 percent or more of their pharmacies EPCS-enabled. Among this group,Massachusetts (90 percent pharmacy-enabled for EPCS) was the first state to pursueDrFirst provides EPCS functionality to more than 250 electronic health record (EHR) and hospitalEPCS as a result of collaboration between the Agency for Healthcare Research andinformation system (HIS) vendors, as well as to thousands more medical practices and physiciansQuality (AHRQ), the Department of Public Health in Massachusetts, Brandeis University,nationwide. Nationally across our customer base, providers notched a 274 percent increase in totalEmdeon and DrFirst, who together successfully implemented the three-year EPCS pilotvolume of EPCS prescriptions transmitted in 2015 versus prior year. Not surprisingly, providers in Newin western Massachusetts which lead to EPCS being legalized at the federal level inYork state increased EPCS prescription volume nearly 3,225 percent over the same period. Removing2010. And in March 2016, New York (96 percent pharmacy-enabled for EPCS) willNew York’s growth from the national figures shows that the balance of the country’s users increasedbecome the first state to enforce a legal mandate that all medications – legend drugstheir use of EPCS by 204 percent over the prior year. Clearly, this represents substantial growth in EPCSand controlled substances – must be prescribed electronically.by those who have adopted the technology.Also noteworthy are states well behind the EPCS-enabled curve in 2014 that madeHowever, EPCS is not widely adopted by doctors. On average, just five percent of all U.S. practitionerssignificant course corrections over the last twelve months. These include North Dakota,are currently EPCS-enabled.4 Even in New York on the eve of its I-STOP mandate, only 27 percent ofgrowing from just 22 percent of pharmacies enabled in 2014 to 73 percent in 2015, andpractitioners are EPCS-enabled to-date.Montana rising from virtually zero enabled pharmacies in 2014 to 68 percent in 2015.Why Are Physicians Slow to Adopt EPCS?The chart illustrates prescription volume for the top controlled drugs prescribed inConsider New York a “perfect storm” of sorts as relates to EPCS adoption: legislation mandating its use,2015. Unsurprisingly, narcotic analgesics are the most prescribed controlled substancea clear need for better control of opioids to stem abuse and misuse, a majority of pharmacies able totherapeutic category.accept EPCS prescriptions, and a large body of physicians who already e-prescribe for legend drugs.Prescriptions for medicationsBack in January 2015 (leading up to the original New York I-STOP mandate deadline), our researchused for narcotic withdrawal areshowed that more than 80 percent of ambulatory EHR vendors and more than 85 percent of acute HISon the rise and corroborate avendors serving New York providers were ready to provide EPCS capability to their users. Even still,growing and serious healthproviders and interest groups pushed legislators to delay the start of the law.concern regarding the use ofnarcotic analgesics. This categoryToday with likely 90 percent of EHRs and HISs having EPCS capability, and a host of stand-alonenow represents the fourth higheste-prescribing systems widely available to providers, grumblings continue. The Medical Society of thetherapeutic category of controlledState of New York (MSSNY), in collaboration with DrFirst, surveyed MSSNY physician members aboutsubstance prescriptions. Future3 44. Surescripts data
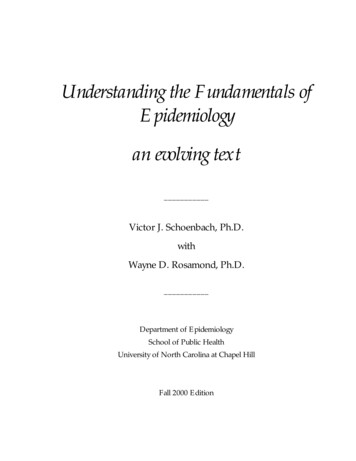
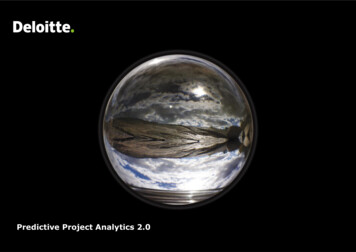
EPCS Prescriptions Sent to Retail PharmaciesIncrease from 2014 to 2015their EPCS readiness in December 2015. Among more than 900 respondents who saidthey do prescribe controlled substances, 44 percent said they were not ready for EPCS.The reasons for not being EPCS-ready are in the chart below:“The slow rate of providerWhy New York Doctors HaveNot Deployed EPCSI’m concernedabout the cost9%adoption of EPCS is surprising,given the compelling patientsafety benefits and convenienceof EPCS,” says Tom Sullivan, MD,a board-certified cardiologist andI don’t want todisrupt mypractice12%I resent themandate14%My EMR is notready37%DrFirst’s chief strategy officer. “Iexpected that once EPCS wasmade legal in all states andI don’t writemany scripts28%EPCS-enabled pharmaciesbecame prevalent, providerswould quickly adopt thisimportant tool. Clearly, moreSource: MSSNY Member E-Prescribing Survey,December 2015education is needed about thesignificant benefits of EPCS.”In addition to improved education and awareness, one of the most frequent hurdles tostarting EPCS is the prescriber identity proofing process. Prescriber identity proofing isrequired by DEA regulations. Many physicians don’t take this into account as theyprepare to adopt EPCS. For prescribers who are employed by hospitals or other largehealthcare delivery systems, as well as independent physicians on staff at hospitals, theirorganization’s credentialing office can work with the e-prescribing vendor to facilitateinstitutional identity proofing. However, for smaller practices and solo practitioners,identity proofing requires individual physician participation. While typically facilitated bythe e-prescribing services vendor, the actual identity proofing and authentication areconducted under DEA rules by independent third parties, such as Experian andSymantec that require the prescriber to correctly answer several questions to prove hisor her identity, register a token and bind it to the identity and software application.5 ecticutDistrict of naNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOklahomaOregonOhioPennsylvaniaRhode IslandSouth CarolinaSouth est 881%259%565%1,120%1,516%96%305%278%87%717%“The ID proofing and authentication process is notunduly arduous, but providers do need to allowtime for Experian or another registration authorityto verify their identity,” says Sullivan. “Over 25percent of doctors fail to answer the questionscorrectly on the first try; you’d be surprised howmany doctors get the exact amount of their homemortgage payment wrong during that process.”“Education for prescribers is key to moving theindustry from paper to electronic prescriptions forcontrolled substances,” says Peter Kaufman, MD, aboard-certified gastroenterologist who also servesas DrFirst’s chief medical officer. “For example,credible EPCS technology vendors can guidedoctors through the DEA’s requiredidentity-proofing process so that EPCS enrollmentcan be completed in just a few days. Use oftwo-factor authentication for each controlledsubstance prescription, another DEA-requirement,does add one step to the e-prescribing workflow,but it is not particularly intrusive. So at the end ofthe day, the incremental EPCS requirements,particularly for doctors who already e-prescribelegend drugs, are relatively insignificant whencompared to the patient safety benefits EPCSaffords.”Whether in New York or on a national level, manyphysicians are simply unaware that they can nowprescribe all substances electronically. Othersresist adapting to the new technology ormistakenly believe it will be costly andtime-consuming to implement. However, clearlythe technology is available and many thousands ofdoctors are making use of it. 6
“Today, most of the diversionThe Role of PDMP Interoperabilityand drug abuse comes from licensed physiciansIncreased drug information exchange among state prescription drug monitoring programs (PDMPs)acute and chronic pain problems. Pharmaceuticalwill also help speed provider adoption of EPCS. Forty-nine states (Missouri is the exception) havecompanies have manufactured more and morecreated these programs, which collect data from pharmacies on dispensed controlled substancepowerful opioid analgesics that are easy toprescriptions, digitize it and make it accessible to prescribers, pharmacies and law enforcementadminister, inexpensive and with a plentiful supply.officials.Patients can easily become addicted if not properlyNew York’s I-STOP Lawwriting legitimate prescriptions for patients withmonitored.”Nearly half (22) of states with PDMP programs in place require providers to access the state PDMPbefore prescribing painkillers, although these states laws vary widely in their specific rules,Key Benefits of E-PrescribingNew York’s Internet System for TrackingOverprescribing (I-STOP) Act takes fulleffect March 27, 2016, and is aimed atcombating the rising rates ofprescription drug abuse. The lawrequires: Mandatory PMP Queries: Medicalproviders must query the stateprescription monitoring system(PMP) and review a patient’s recentmedication history prior to writingany prescriptions for Schedule II-Vcontrolled substances. This phasebecame effective in 2013. Mandatory E-Prescribing: Allprescriptions, non-controlled orlegend drugs as well as Schedule II-Vcontrolled substances, must be sentelectronically beginning March 27,2016.enforcement and penalties. Arizona, for example, requires prescribers to query the PDMP for workercompensation cases only, but has no specific penalty for noncompliance. Kentucky mandates thatImproves Patient Safety. E-prescribing typicallyprescribers query the PDMP prior to dispensing any Schedule II controlled substance or a Scheduleenables clinical alerts to guard against drug-to-drugIII controlled substance containing hydrocodone, and threatens licensure discipline forand drug-to-allergy interactions, inappropriatenoncompliance.dosing, duplicate therapies as well as patient status,such as pregnancy or breast-feeding. E-prescribingThere is strong indication that these requirements can be effective. One year after New York beganalso reduces common errors inherent inrequiring providers to check its online registry, the number of prescriptions for all opioids decreasedpaper-based prescribing, including illegibleby 10 percent. The largest decreases were seen in hydrocodone (down 20 percent) and codeine 5handwriting, misinterpreted abbreviations and(down 33 percent.)5unclear dosages. E-prescribing systems also offerclinical decision tools such as medicationStill, many providers are critical of PDMP use. Providers who practice near state borders, inadherence monitoring, real-time benefit checking,particular, argue that taking time to check the PDMP database impedes clinical workflow andelectronic prior authorization and other patientdoesn’t necessarily provide information about drugs prescribed for patients in adjacent states.support services that lead to better clinicalEfforts are underway at the state level to address these and other concerns. One initiative isoutcomes.spearheaded by the National Association of Boards of Pharmacy (NABP), which launched thePrescription Monitoring Program (PMP) InterConnect in 2011. InterConnect enables interoperabilitySaves Time. While controlled substances onlyand interstate data sharing among state PDMPs that participate in the program. The use of PMPrepresent about 10 percent of prescribedInterConnect to share data has grown from just a few thousand interstate transactions in 2011 tomedications, 90 percent of practitioners writemore than 1 million per month. To date, 35 states (including New York) have executed memorandaprescriptions for controlled substances. For doctorsof understanding with NABP to participate and 30 of those states are now live.6who prescribe legend drugs electronically, adoptingEPCS integrates all prescribing into a singleNew York’s I-STOP law carries severepenalties for non-compliance, includingpotential loss of license, civil penaltiesand/or criminal charges. To qualify for awaiver, New York providers must showeconomic hardship, technologicallimitations outside of their control, orother exceptional circumstances.“Twenty years ago most people who were diverting or abusing drugs were getting theirprescriptions illegally from stolen or forged and altered paper prescriptions,” Sullivan says.workflow (versus electronic for some meds andpaper for others). This streamlines workflow forprescribers and staff, and reduces waiting time forpatients when they pick up their prescriptions.7 5. PDMP Center of Excellence at Brandeis University6. National Assciation of Boards of Pharmacy 8
Drives ROI. Studies have found that e-prescribing can save a medical practice anestimated 15,769 per full-time physician, per year due to increased efficiency.Increases Security. E-prescribing provides pharmacists with the assurance that theprescription they receive is exactly what the provider originally ordered and has not beentampered with on the way to the pharmacy. Certified, audited application vendors arethe only entities that can conduct EPCS transactions to pharmacies. And becausee-prescriptions travel direct-to-pharmacy, the physician’s DEA number is not exposed tothe patient or other parties.Reduces Doctor-Shopping: E-prescribing technology can be configured with amedication history module and, in the future, access to interstate PDMP data. Thisallows providers and clinical staff to capture and view comprehensive prescriptionhistories at the point of care, reducing the likelihood of doctor shopping as well asadverse drug events.Enables Prescriber Pattern Analysis. EPCS analytics reporting can reveal variations incontrolled substance prescribing patterns among peers. This allows providers to identifyand address reasons for outl
Pharmacy data from DrFirst’s Rcopia e-prescribing system, CY 2014 - CY 2015. All EPCS pharmacy data in this report ref