Transcription
The Graduate Nurse EducationDemonstration: Lessons LearnedBarbara A. Todd, DNP, CRNP, FAANP, FAANDirector, Graduate Nurse Education DemonstrationHospital University of Pennsylvania
Objectivesw Discuss the policy rationale for the GNE Projectw Discuss the lessons learned and challenges related to the projectimplementationw Discuss the formal evaluation outcomes of the GNE demonstration2
Agenda Today1Introduction – the Policy Question2Overview of the Greater Philadelphia Area GNE3CMS Evaluation Report4Lessons Learned and Next Steps3
2010: ACA GNE Demonstration Coalition of stakeholders led by AACN and AARP vigorously pursued Medicarepolicy reforms to include GNE; the GNE Demonstration resulted 200 million for 4 years (2012-16) administered by Centers for Medicare andMedicaid Services (CMS) Prior to the GNE section 5509 mandate, Medicare title XVIII funds could not beused for the clinical education training of APRN students. Although CMS paidawardee hospitals to support preceptorships and clinical education for medicalresidents, there is no established mechanism under current law for Medicare tosupport similar payments to hospitals for APRN students. The GNE demonstration represents an innovative project that allowed theopportunity to contribute to the clinical education training of APRN students4
Affordable Care Act: Graduate Nurse EducationDemonstrationw Description: Mandated under the Affordable Care Act Section 5509(a)(1)(B) Administered by Centers for Medicare and Medicaid Services (CMS) InnovationCenter Primary care transformation 5 participating hospital systems selectedw Primary Goals: Increase the provision of qualified training to APRN students– Primary care– Transitional care– Chronic care management Tests feasibility, effectiveness, cost of increasing production of APRNs throughMedicare payments to hospitals for reasonable costs of clinical APRN training5
Policy Contextw Affordable Care Act extends insurance coverage to 30 million peoplew The nation already has a shortage of primary carew Evidence shows that APRNs can provide safe, effective care, includingprimary care, but there are not enough of themw Nursing schools state a barrier to producing more APRNs is lack of clinicaltraining opportunities and preceptorsw Potential for APRNs to contribute to solving primary care shortage ifproduction could be increased to meet growing demandw Capacity of schools of nursing to expand is limited by shortage ofpreceptors and faculty; plenty of student applicantsw Medicare GNE payments to providers to offset lost of productivity ofpreceptors could help in recruitment of more preceptors6
Questions Addressed Across the Demonstration Sitesw Are current Medicare GME payment policies geared to licensed physiciansfeasible for (pre-certified APRN) degree-granting educational programs?w Will the CMS incentive to increase graduation of APRNs through payingonly for incremental students have major unintended consequences onaccess to clinical preceptors?w Does reimbursement of clinical costs of preparing APRNs result insignificant increased production, especially in primary care?w Does reimbursement result in more clinical placements and higher qualityclinical training (types of placements, student experiences and satisfaction,qualifications of preceptors)?w Do APRN graduates take positions serving populations in need:underserved, minorities, primary care?7
Demonstration Designw Medicare payments to hospitalsw Allowable costs include only clinical education (not didactic) Payments to nursing schools to increase enrollments Payments to preceptor practices to offset lost productivityw Payments based on incremental students (increase in students over predemonstration baseline)w Eligible APN incremental students: NPs all specialties, nurse anesthetists, nurse midwives, clinical nursespecialists BSN- DNP programs only (no post Master’s)w 50% of funded training must be in community settings/primary care8
Funded Hospitals: Two Models Emergedw Single hospital and its primary affiliated nursing school plus communitypartners Duke University Hospital Rush University Hospitalw Regional consortia with multiple nursing schools and hospitals, and manycommunity partners covering a geographic area Hospital University of Pennsylvania: Greater Philadelphia Region Memorial Hermann-Texas Medical Center: Texas Gulf Coast Region Honor Health: State of Arizona9
Consortia Modelw The most compelling rationale for the consortia model is urban areas with multipleschools and competition for limited community-based preceptors where centralcoordination is neededw Some schools with APRN programs are not affiliated with a hospital to facilitateMedicare fundingw Consortia model enables a large hospital with substantial financial infrastructure tomanage contracting, payment, and CMS auditing requirements for multipleinstitutions10
19 Universities and Schools of Nursingw Duke Universityw Arizona State Universityw Rush Universityw University of Arizonaw Grand Canyon Universityw Thomas Jefferson Universityw Temple Universityw Northern Arizonaw University of Pennsylvaniaw Drexel Universityw LaSalle Universityw Villanova Universityw Gwynedd Mercy Universityw Neumann Universityw Texas Woman’s Universityw University of Texas Health SciencesCenter, Houstonw University of Texas Medical Branch,Galvestonw Widener Universityw Prairie View A&M11
Greater Philadelphia GNE Goalsw Provide Medicare beneficiaries with improved access to health careprovider services by significantly increasing the number of APRNseducated in the Greater Philadelphia Regionw Create an efficient partnership collaborative, replicable, networking modelbetween hospitals, regional nursing schools and clinical partnersw Allows monitoring, collection and information exchange (‘best practices,”etc.) through coordinated communication between regional health caresystems, nursing programs, and clinical partners12
Pennsylvania Healthcare Landscapew Pennsylvania1 251 licensed hospitals– 1.5 million hospital admissions– 31 million ambulatory visits– 6.2 million ER visits Projected shortage of 55,000 physicians through 2020 across all specialtiesw Philadelphia Region 5 Medical schools 9 Schools of nursing with APRN programs 8 Physician assistant programs Thousands of students1 Source: Pennsylvania Department of Health13
HUP GNE APRN ProgramsSONNPCNSCRNAüüUniversity ofPennsylvaniaüThomas enerüüTempleüGwyneddüNeumannüCNMüüü14
15Demonstration Clinical FootprintCommunity Healthcare Partnerships across the Greater Philadelphiaarea and beyond with over 2000 clinical training Partnerships including:ü Hospital and university based partnersü Community Clinicsü Federally Qualified Health Centersü Nurse Managed Centersü Retail clinicsü Private Practices415
Early Challengesw Incremental Payment Methodologyw Contractsw Primary care definitionw Increasing clinical training capacityw Concern of sustainability after 2018w SON and clinical practice site resistance16
Strategies to Increase Clinical Capacityw Guiding principles: Increasing continuity of clinical experience Decrease fragmentation of clinical experience Development of new preceptor relationships Site with capacity to accept additional students Increase access to nurse managed clinics and FQHCs Retail clinics IPE opportunities NP Facilitator Model GOAL: INCREASE CLINICAL TRAINING CAPACITY– Scarcity to abundance?17
18Increasing Clinical Capacity Strategy Recruit facilitiesthat have noAPRNs orstudents Explain benefitsFacilities with noAPRN or studentsStudents inTraining Place studentswith facilities Facilities seebenefit andhire APRNFacilities haveAPRNs18
GNE Enrollment: Greater Philadelphia96.4 % increase inenrollment eDY-1DY-2DY-319
GNE Graduates: Greater Philadelphia91% increase ingraduates -620
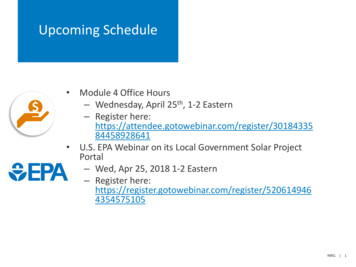
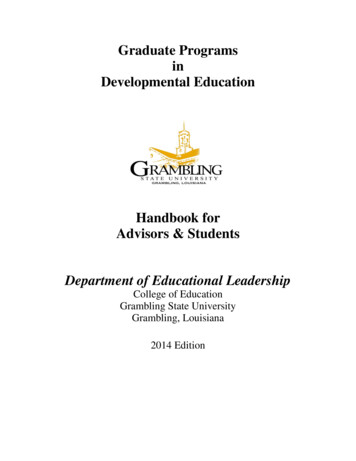
GNE APRN Graduates by Role (Baseline to 068619 131067 1610017 141119517 1412268413 219 220BaselineDY1DY2NPDY3CRNADY4CNSDY5DY6CNM21
GNE Alumni Survey (DY-5)w 25% of students are being employed at sites where they did clinicaltrainingw 50% of students first position in state of PAw 21% from under represented minority groups22
GNE Evaluation Report*A final evaluation report including findingsfor the complete 6-year demonstrationexperience will be available in the fall of201923
GNE Evaluation Research Questionsw How was the GNE demonstration projected implemented andoperationalized? What are the network characteristics and demonstration operationprocesses? How does the demonstration influence precepted clinical educationplacements and the placement processes? What notable successes and challenges do networks experience? What are the networks’ plan for sustainability?w How effective was the GNE Demonstration project in increasinggrowth in the APRN workforce? What is the effect on APRN growth overall? What is the effect on APRN enrollment and graduation by specialty? Is the demonstration associated with spillover effects to nonparticipating SONs?w What is the total cost of the GNE project overall?Source: Evaluation of the GNE Demonstration Project: Report to Congress.U.S. Department of Health and Human Services, May 201824
National Demonstration is Successfulw It is feasible for hospitals to distribute APRN clinical training funds to multipleschools of nursing and clinical practices including community-based settingsw APRN enrollments and graduations have more than doubledw All sites met the requirement for 50% of training in community-based settingsw Participating students are from diverse backgroundsw Preliminary results suggest a substantial portion of graduates are working inprimary carew There is high demand among precepting organizations and other settings to hireAPRN graduates25
Looking Forwardw Use the success of Demonstration to inform national discussion on newMedicare GNE benefitw Health systems and community stakeholder support is criticalw Nursing school support is essential26
How effective was the GNE Demonstration project inincreasing growth in the APRN workforce?27
Total Annual APRN Student Enrollment from GNE and Non-GNESONs by YearGNE 0082009201020112012201320142015SOURCE: GNE Demonstration Evaluation Report to Congress, 2017 & AACNData28
Mean APRN Students Enrollment in GNE SONs vs. non-GNESONs Comparison 501002006200720082009201220132014201529
Annual APRN Student Graduation from GNE DemonstrationNursing 620072008200920102011201220132014SOURCE: GNE Demonstration Evaluation Report to Congress, 201730
Clinical Education Hours Completed by Incremental APRNStudents from 00000DY 2012DY 2013HospitalCommunityDY 2014TotalSOURCE: GNE Demonstration Evaluation Report to Congress, 201731
Percent of Precepted NP Clinical Hours Completed atHospital and Community Settings by Incremental StudentsEnrolled in GNE SONs by YearSOURCE: GNE Demonstration Evaluation Report to Congress, 201732
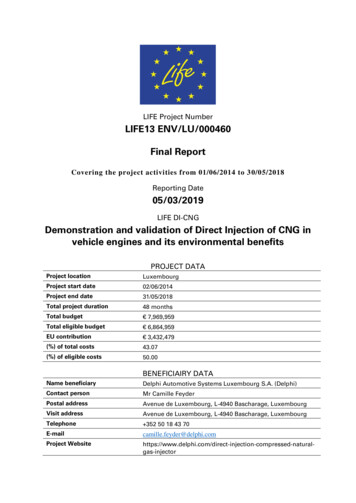
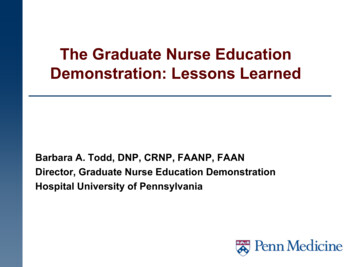
GNE Demonstration Trainingand Employment LocationsClinical Training SitesEmployment LocationsExcludes Duke Employment Locations33
How was the GNE demonstration projected implementedand operationalized?w There was wide variation with each of the 5 networks Numerous community based clinics including FQHCs, Indian HealthServices and hospital based community clinics Rural and non-rural areas Initial slow start up in Year 1 GNE infrastructure Various approaches to preceptor payment methodology Innovations34
What is the total cost of the GNE project overall?35
Successes and Challengesw Increased awareness in medical community on need for APRNsw Increased enrollment and graduatesw Implementation presented many challenges particularly related to paymentmethodologyw Concerns about sustainability “Collaboration will sustain post demonstration, but what thatcollaboration will look is yet to be determined” “Concern that sites will drop after the GNE money is gone” “Variation in preceptor incentives” “Strengthened SON’s relationships with existing clinical education sites” “Partnered with new community based clinics”36
Key Demonstration Results The five site demonstration has a national footprint in terms of training sites andlocation of graduates.Greater APRN enrollment and graduation growth in demonstration schools thancomparison schoolsMajority of clinical training in community settingsMajority of growth in APRNs in the demonstration was in nurse practitioners, who arein great demand nationally to improve access to care.The cost of clinical training of an APRN to graduation, in addition to tuition, wasestimated to be less than 30,000, a very good investment compared to the cost ofcommunity-based residency training of primary care physicians in the TeachingHealth Center demonstration of 150,000 per year.Cost per incremental APRN trained was lower as the number of nursing schools ineach demonstration hub increased.Affiliation of a school of nursing with a hospital decreases the average school ofnursing clinical training costs of APRN education.APRN graduates practice in rural and urban areas including federally qualified healthcenters, nurse-managed clinics, ambulatory medical practices, retail clinics, hospitals Preceptor development modules Workforce pipelines for regional health care37
Key Learningsw Demonstration has been complexw Post demonstration would have to be simplifiedw Clinical productivity and clinical education are colliding Increasing competition for clinical training opportunities– On line programs– Other health care professional students Demand Supply?w Workforce demands in region metw New models for APRN clinical education neededw Clinical preceptor engagement is crucialw Need to centralize clinical training rotations in a given regionw Dissemination of findings38
Questions39
between hospitals, regional nursing schools and clinical partners wAllows monitoring, collection and information exchange (‘best practices,” etc.) through coordinated communication between regional health care systems, nursing programs,