Transcription
JONAVolume 39, Number 11, pp 485-493Copyright B 2009 Wolters Kluwer Health Lippincott Williams & WilkinsTHE JOURNAL OF NURSING ADMINISTRATIONNurse and Nurse Assistant Perceptionsof Missed Nursing CareWhat Does It Tell Us About Teamwork?Beatrice J. Kalisch, PhDMissed nursing care is a pervasive problem in acutecare hospitals as is dysfunctional nursing teamwork.Given that teamwork has a significant impact onhealthcare quality and patient safety, the authorreports findings from a study that examined differences in perceptions between RNs and nursing assistants as to the extent of missed nursing care andthe reasons for missing that care. Study findingspoint to a lack of essential elements of teamwork (ie,closed-looped communication, leadership, team orientation, trust, and shared mental models). Theauthor analyzes what this reveals about teamworkbetween these 2 groups of nursing personnel whowork side by side caring for the same patients andoffers specific interventions.tient care that is omitted or significantly delayed,4and in patient safety language, they are errors ofomission (as opposed to errors of commission). Aparallel body of literature suggests that there areproblems with the working relationships of RNs andNAs.5-16 Mather and Bakas11 identified the lack ofteamwork as a barrier to appropriate continence carefor nursing home patients. This study also documented a perception that RNs do not listen to NAsor include them in planning care. In interviews with13 RNs and 9 NAs in an acute care hospital, Potterand Grant13 identified lack of trust and respect in theRN-NA relationships, validating findings by otherinvestigators.5,14-16Nursing care in acute care hospital settings is usuallyorganized into teams of nursing personnel thatinclude RNs, LPNs, and nursing attendants (NAs).A team is defined as 2 of more individuals who areinterdependent and share a common purpose.1 Thegroup of staff members on acute care patient careunits meets this definition of a team.In any nursing care environment, the potential fornecessary clinical care to be omitted exists. Previousresearch findings suggest that missed nursing careoccurs frequently in acute care hospitals.2,3 Missednursing care is defined as any aspect of required pa-Previous StudiesAuthor Affiliation: Chair, Nursing Business and Health Systems,Titus Professor, University of Michigan, Ann Arbor, Michigan.Correspondence: University of Michigan School of Nursing,400 N Ingalls St, Ann Arbor, MI 48109 (bkalisch@umich.edu).Funding: This study was funded by the Michigan Center forHealth Intervention, University of Michigan School of Nursing,National Institutes of HealthYNational Institute for NursingResearch (P30 NR009000) and by the Blue Cross Blue ShieldFoundation of Michigan.Missed Nursing CareWhile the phenomena of missed nursing care hasundoubtedly existed before now, the concept hasonly recently been recognized and studied. Kalisch2conducted a qualitative study using focus groups toexamine the types of care being missed in acute carehospitals and found 9 areas of missed care (ambulation, turning, delayed or missed feedings, patientteaching, discharge planning, emotional support,hygiene, intake and output documentation, andsurveillance) and 7 reasons for missing nursing care(too few staff, poor use of existing staff resources,time required for the intervention, poor teamwork,ineffective delegation, habit, and denial).There have been studies of specific aspects ofnursing care being missed such as failure to ambulate17-21 and turn patients, inattention to the nutritional status of patients,22 not washing hands, notadministering intravenous site care, and the failure toJONA Vol. 39, No. 11 November 2009Copyright @ 2009 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.485
administer ordered medications.23-25 However, theoverall concept of missed care has not received attention until recently. To quantify the amount and typeof care missed, the MISSCARE Survey was developed and tested for its psychometric properties.26The MISSCARE Survey asks respondents their perceptions of which elements of care are being missed(and their frequency), as well as the reasons why thiscare is being missed.Using the MISSCARE Survey, a study of RNs (n 459) in 3 Midwestern hospitals revealed a significantamount of missed careV40% assessments and 70%interventions, basic care, and planning.3 The amountof care being missed was further substantiated in asecond study using the MISSCARE Survey. Certainelements of nursing care, including ambulation andmouth care, were among the most frequently missedin both studies. Patient assessment at each shift, glucose monitoring, focused reassessments, and vital signswere among the least missed elements of care in bothstudies. Reasons for missing care were also similar inthe 2 studies. Labor resources, such as adequacy ofstaffing, were the most prevalent reason for missedcare, followed by material resources such as havingmedications and equipment available when neededand finally communication and teamwork (Kalisch BJ,Tschannen D, Lee H. Missed nursing care: a report oftwo studies; unpublished report).3Nursing TeamworkFew studies have examined the working relationshipbetween RNs and NAs. There are mixed findings asto the opinion of RNs about the quality of work of theNAs, with a few studies showing a positive evaluation27 but most reporting concern about the qualityand performance of the NA as well as their trainingand lack of trust in their performance.5,6,9,10,12 It hasbeen reported that RNs do not always trust thecompetency level of NAs and thus fear delegatingto them.10 Salmond,14 in her study of 53 hospitals,found a dichotomy in that 43% of RNs felt thatNAs are not able to determine patient problems,whereas 90% of the NAs stated that they wereadequately prepared for their job.A qualitative study was conducted that appliedSalas and colleagues’28 theory of teamwork to test itsapplicability to inpatient nursing teams. The framework of Salas et al28 explaining teamwork postulates5 core components: (1) team leadership (direction,structure, and support provided by one or moremembers of the team), (2) team orientation (ie, teamfunctioning, goals and success is more importantthan the individual’s), (3) backup behavior (ie, teammembers moving in to help one another or providefeedback when needed), (4) mutual performance486monitoring, and (5) adaptability; and 3 coordinatingmechanisms: (1) shared mental models (ie, mutualconceptualizations of team tasks, roles, strengths/weaknesses, processes, and strategies to attain goalsby all team members), (2) closed-loop communication (active information exchange in which the receiver verifies receipt and the sender verifies that theintended message was received), and (3) mutual trust.Each of the 8 elements of the model of Salas et alwas found to be applicable to the team functioningof nursing teams in acute care inpatient units.In another study,29 a survey instrument, theNursing Teamwork Survey (NTS), was developedand tested for its psychometric properties with morethan 1,700 nursing staff members in 2 hospitals.The NTS was designed specifically to capture thelevels of teamwork among nursing teams in acutecare hospital units. The exploratory and confirmatory factor analyses yielded 5 subscales (ie, leadership, team orientation, shared mental models, trust,and backup) from the NTS data that match 5 of the8 components of the Salas et al model.Study QuestionsThe purpose of this study was to compare RNs’ versusNAs’ perceptions of elements of missed care andreasons for missing care and assess how they explainedselected issues underlying teamwork between NAs andRNs. The specific questions are as follows: How do the amount and elements of missednursing care vary between RNs and NAs? How do the reasons given for missing nurs-ing care vary between RNs and NAs? How do these findings (missed care and rea-sons) shed light on the dynamics of teamwork between RNs and NAs?MethodA mixed-method approach was applied to this study.Stage 1 of data collection and analysis involved conducting a survey of RNs and NAs. In the secondstage, focus groups were conducted with RNs andNAs to gain insight into the survey results.Sample and SettingThe sample population for stage 1 included the nursing staff employed and providing direct patient careon 18 units in 1 hospital. The sample included RNs(n 633) and NAs (n 121). Because there were only8 LPNs who completed the survey, they wereexcluded from this analysis because of insufficientsample size. The response rate was 52%.JONA Vol. 39, No. 11 November 2009Copyright @ 2009 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
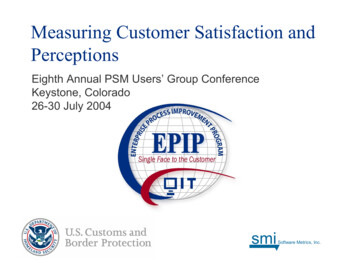
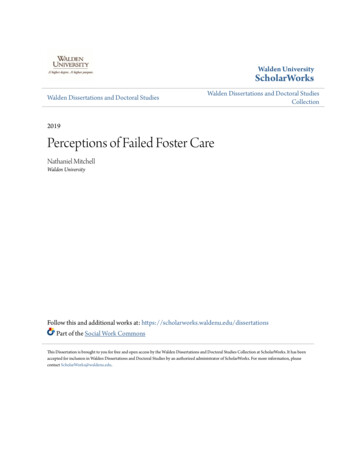
In stage 2, 2 focus groups with RNs and 2 withNAs were conducted in separate sessions in the samefacility used in stage 1. The focus group interviewsused a semistructured design. The focus groupquestions centered on the survey results, asking forinterpretation of the results and its potential impacton nursing teamwork.InstrumentThe MISSCARE Survey was used to quantify and explain missed nursing care. In addition to perceptionsof missed nursing care and reasons for missedcare, demographic information (education, experience,sex), questions about work schedules (shift, hoursworked), and satisfaction (with job and role) wereincluded. The MISSCARE Survey is divided into 2parts: part A asks nurses to identify how frequentlythe elements of nursing care are missed (eg, ambulation, turning, patient assessment, teaching, dischargeplanning, etc) using a 4-point Likert scale, with anchorslabeled as rarely missed to always missed. Part B asksnurses’ perceptions of why care is being missed, usinga 4-point Likert scale, anchored from not a reason toa significant reason for why care is being missed.Validity and reliability of the tool have beenreported in detail elsewhere.26 The content validityindex was 0.89. Cronbach !’s ranged from .86 to.64. Pearson correlation coefficient on a test-retestof the same subjects yielded 0.87 on part A and 0.86on part B.ProceduresAfter securing administrative support and institutional review board approval, the first stage of datacollection involved distribution of the survey packet,which included a letter explaining the study, theMISSCARE Survey, and a return envelope, to eachstaff member. Locked boxes were placed on each unitfor return of completed surveys. The second stage ofdata collection involved recruitment of RNs and NAsfor separate focus groups. Each 60-minute focusgroup discussion was tape recorded and transcribed.Participants received a 15 gift certificate as a tokenof appreciation for their participation. Focus groupparticipants were asked to commit to confidentiality(to not quote the others in the group outside the focusgroup). They were assured of confidentiality of theircomments by the investigator and were encouragedto be as open and honest as possible.Data AnalysisPhase 1 data used the SPSS, version 16.0 (SPSS, Chicago,Illinois) for data analyses. Descriptive analyses werecomputed to summarize missed nursing care and reasons for missed care. An overall missed care scorefrom part A was computed and analyzed. This overallmissed care score is the average amount of missed careidentified for each of the elements of nursing care foreach participant. Independent-samples t tests werecompleted to establish significant differences betweenRNs and NAs on elements (part A) and reasons (partB) for missed care. The data generated in phase 2 ofthe data collection, transcribed interviews, were analyzed using NVivo by QRS International (Cambridge,MA),30 a qualitative analysis software, and by applying a grounded theory approach by which empirical data are thematically categorized by induction.31FindingsDescriptive statistics for the sample are shown inTable 1. RNs were primarily women (90.8%) betweenthe ages of 26 and 44 years (70.1%) and working fulltime (83.9%). The average RN had greater than 10years of experience (31.6%) and held a bachelor’sdegree (56.1%). Work hours included days (33.6%),nights (31.9%), evening shifts (7.6%), and rotatingshifts (26.9%). Patient care units were categorizedinto ICU (26.9%), intermediate unit (21.5%), andmedical-surgical-oncology-rehabilitation (51.7%).The NAs sampled were predominately women(83.1%), younger than 44 years (85.8%), and workingfull time (68.3%) and with the highest education being a high school diploma (58.3%). Shifts worked included days (38%), nights (20.7%), evenings (23.1%),and rotating (18.2%). Most NAs had between 6months and less than 5 years of experience (64.7%).Unit of employment included ICUs (21.7%), intermediate (25.8%), and medical-surgical-oncologyrehabilitation (52.5%).Table 1 shows that RNs and NAs were significantly different in a number of areas. The NAs hadmore men; more were younger than 25 years, with 2to 5 years of experience, with grade school as thehighest level of education, and working days andevenings. The RNs had more women, more in the26- to 34-year age bracket, more working full time,more working nights and rotating, and more whohave worked for more than 10 years. More than halfof the RNs reported having a baccalaureate degree.There was no significant difference in type of unitthey worked on.Elements of Missed CareOn the overall missed care score, RNs (mean, 1.71[SD, 0.34]) reported more missed care than NAs(mean, 1.49 [SD, 0.37]) (t752 6.35, P G .001). WhileRNs and NAs should be working together as a teamto care for patients (ambulating, turning, etc), thegeneral practice is that RNs are responsible forJONA Vol. 39, No. 11 November 2009Copyright @ 2009 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.487
Table 1. Sample Characteristics (N 754)Sample SizeSexMaleFemaleAge, yG2526-3435-4445-5455-64Years of experiencee6 mo96 mo to e2 y92 to e5 y95 to e10 yQ10 yHighest degreeGrade/high school and GEDaAssociate degreeBachelors degreeGraduate degreeEmployment status, h/wkQ30G30Work edical-surgical-rehabilitation-oncologyRNs (n 633)NAs (n 121)56 (9.2)553 (90.8)20 (16.9)98 26168(58.3)(21.7)(13.3)(6.7)#25.547a531 (83.9)102 (16.1)82 (68.3)38 7)(18.2)1.918170 (26.9)136 (21.5)327 (51.7)26 (21.7)31 (25.8)63 (52.5)Abbreviations: GED, general education development test; NAs, nursing attendants.Values are presented as n (%).aP G .05.bP G .01.certain tasks, and NAs for others. Therefore, theelements of care in part A of the MISSCARE Surveywere categorized as RN, NA, and combined responsibilities. As can be seen in Table 2, RNs felt thatitems typically completed by the NA and thoseactivities that are shared between RNs and NAswere missed more than did the NAs felt they were.The perceptions of missed care were similar betweenRNs and NAs for only 5 (of 24) elements of care (allRN-only responsibilities) in the survey (ie, medications administered within 30 minutes before or afterscheduled time, PRN medication requests addressedwithin 15 minutes, patient assessments performed ateach shift, focused reassessments according to patientcondition, teaching patients about plans for their careafter discharge). RNs reported significantly moremissed care than NAs in all remaining elements ofcare: ambulation, mouth care, intravenous/centralline care, documentation, patient bathing or skincare, toileting patients, feeding patient while food iswarm, turning, assessing response to medications,488providing emotional support, monitoring intake andoutput, providing wound care, performing vital signs,monitoring serum glucose, and attending interdisciplinary conferences (all P G .01). RNs also identifiedmore missed responses to call lights and handwashing (both P G .05). On the other hand, NAsdid not identify any areas where they believed morecare was missed than RNs.Reasons for Missed CareAs can be noted in Table 3, staff/labor resources wereidentified as the greatest reason for missed care byboth RNs and NAs, with material resources next andcommunication last. RNs (mean, 3.19 [SD, 0.57]) feltthat labor resources were more of a cause for missingcare than did NAs (P G .01). RNs identified an unexpected rise in patient volume, urgent patient situations, and admissions and discharges more frequentlythan did NAs (P G .001). RNs and NAs did not varysignificantly on 2 reasons for missing careVlevel ofstaffing and the number of assistive personnel.JONA Vol. 39, No. 11 November 2009Copyright @ 2009 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Table 2. RNs vs. Nursing Assistants (NA): Part A Elements of Missed Nursing CareRN (n 633)Part ANursing care usually done by RN aloneAttend interdisciplinary care conferences whenever heldFull documentation of all necessary dataPatient teaching about procedures, tests, and otherdiagnostic studiesMedications administered within 30 min before or afterscheduled timeAssess effectiveness of medicationsIntravenous/central line site care and assessments accordingto hospital policyPRN medication requests acted on within 15 minWound careFocused reassessments according to patient conditionTeach patient about plans for their care after dischargePatient assessments performed at each shiftNursing care usually done by NAAmbulation 3 times per day or as orderedMouth careFeeding patient when the food is still warmTurning patient every 2 hAssist with toileting needs within 5 min of requestMonitoring intake/outputPatient bathing/skin careSetting up meals for patients who feed themselvesBedside glucose monitoring as orderedNursing care done by both of RN and NAResponse to call light is initiated within 5 minEmotion support to patient and/or familyHand washingVital signs assessed as orderedOverall missed careRNs attributed missed care to gaps in materialresources more frequently than NAs (P G .001).While RNs attributed medications, supplies, andequipment availability when needed as more of areason for missed care than did NAs (P G .05), NAsand RNs agreed (no significant difference) on theitem equipment functioning properly.Although there were no significant differencesbetween RNs’ and NAs’ ratings of communication/teamwork as a reason for missed care, a significantdifference was identified for the item stating, ‘‘Nursing assistant did not communicate that care was notdone.’’ This was identified significantly more often asa reason for missed care by RNs (P G .01). Communication breakdowns within the nursing team wascited by NAs as more of a reason for the missed carethan the RNs (P G 0.05).Focus Group ResultsThe following key findings from stage 1 of the studywere presented to the focus group participants: (1)RNs reported significantly more missed care than didNAs; (2) RNs felt that nursing care activities typically completed by the NA and shared with the NAsNA (n 121)Mean (SD)tP2.80 (0.89)1.91 (0.67)1.87 (0.70)1.89 (0.91)1.54 (0.61)1.55 (0.69)7.1255.2693.7190001.82 (0.69)1.65 (0.86)1.492.1411.77 (0.64)1.63 (0.65)1.53 (0.66)1.25 er
A mixed-method approach was applied to this study. Stage 1 of data collection and analysis involved con-ducting a survey of RNs and NAs. In the second . tio