Transcription
Nutritional Epidemiology LectureTopic 8EPIDEMIOLOGI KVA(Vitamin A DeficiencyEpidemiology)Azrimaidaliza, SKM, MKMPublic Health Science Program Study-Majoring Nutrition Public HealthMedical Faculty Andalas UniversityPadang - West Sumatera
PREFACEKurang Vitamin A (KVA) merupakan salahsatu masalah gizi kurang yang masihdihadapi oleh negara-negara berkembangtermasuk Indonesian KVA à suatu keadaan, ditandairendahnya kadar Vitamin A dalam jaringanpenyimpanan (hati) & melemahnyakemampuan adaptasi terhadap gelap &sangat rendahnya konsumsi/masukkankarotin dari Vitamin A (WHO, 1976)n
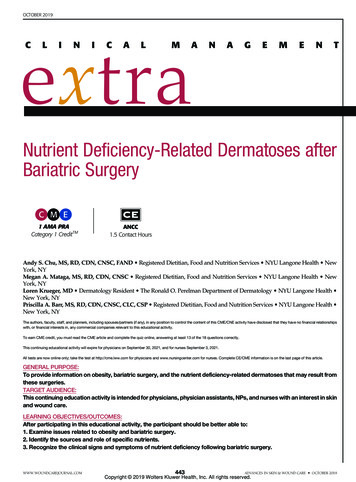
MAP OF VITAMIN A DEFICIENCY (VAD)IN THE WORLD.1Figure 1. Countries categorized by degree of public health importance of Vitamin A deficiency,April 1995, WHO
MAP OF VITAMIN A DEFICIENCYIN THE WORLD.2Source : KP West J Nutr. 2002 in Keith P. West, Jr., Professor Center for Human Nutrition Johns HopkinsBloomberg School of Public Health Baltimore, Maryland, April 16th, 2007
DATA WHOn Setiaptahun à 3-10 juta anakmenderita xeroftalmia dan 250.000– 500.000 anak menjadi butaà menyebabkan dediferensiasi;keratinisasi sel epitel, perubahannafsu makan; xerofthalmia
Source : KP West J Nutr. 2002 in Keith P. West, Jr., Professor Center for Human Nutrition Johns HopkinsBloomberg School of Public Health Baltimore, Maryland, April 16th, 2007
Source : KP West J Nutr. 2002 in Keith P. West, Jr., Professor Center for Human Nutrition Johns HopkinsBloomberg School of Public Health Baltimore, Maryland, April 16th, 2007
BESARAN MASALAH KVA DI DUNIA
MATERNAL VITAMIN ADEFICIENCY IN THE WORLDnMaternal Vitamin ADeficiency : 10% of womendevelopnight blindness inlatter half ofpregnancy in poorlynourished SouthAsian populations
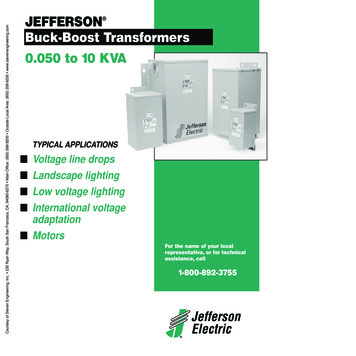
Maternal night blindness VA Deficiency(that can directly affect mother & infant)n40-day male India infant with keratomalacia (X3B),unable to open eyes 3 days after birth. Eyes respondedto VA treatment. Mother had history of night blindnessthroughout pregnancy.Source : M Gupta et al Indian J Pediatr 2005;72:881 Keith P. West, Jr., Professor Center for Human Nutrition JohnsHopkins Bloomberg School of Public Health Baltimore, Maryland, April 16th, 2007
PERKEMBANGAN KVADI INDONESIAA nutrition survey conducted in Indonesiain early 1970s à the prevalence of VADwas very high.n Indonesia à one of the first developingcountries to identify that high levels ofsevere VAD constituted a serious publichealth problem & began to implementprograms to eliminate the problem sincethe 1970s (HKI, 2000).n
CONTINUED Since 1970s-1990s, Indonesia embarkedon a nation-wide vitamin A interventionprogram by providing high-dose vitamin Acapsule twice a year to almost all underfive children.n Within 2 decades, the program àsuccessfully reduced the clinicalprevalence of VAD (xeropthalmia) to0,33% in 1992, a level in which VAD wasno longer considered as a public healthproblem.n
PREVALENSI KVA DIINDONESIANo. Klasifikasi1.2.3.X1B Bercak bitotX2/X3 Xerosis kornea/keratomalasiaXS Parut korneaTahun197819921,327,718,00,3300
CONTINUED Ø Sejaktahun 1992à Indonesia bebas xeropthalmiaà 60 ribu anak balita disertai gejalabercak bitot(X-1b : Prevalensi 0,33%)(SUVITA,1992)Tidak merupakan masalah kesmas
CONTINUED à Namun masih dijumpai 10 jutaanak balita menderita KVA subklinis (50% balita : serum retinol 20 µg/100 ml)n 1992 à Tidak ada data nasionalprevalensi KVA
CONTINUED n Tingginyaproporsi balita denganserum retinol 20 mcg/100 ml àberisiko tinggi u/ terjadinyaxeropthalmia & me tingkatkekebalan tubuh à mudah terserangpenyakit infeksikapsul vitamin A dosis tinggi
CONTINUED n Tahun1998à Survei HKI daerah kumuhperkotaan à masalah KVAmuncul kembalin What is the current magnitude of VADprevalence in Indonesia is difficult tospeculate.
CONTINUED n DiIndonesia à ada laporan lisan daribeberapa propinsià timbul kembali kasus-kasusxerophthalmiaà di NTB ditemukan kasus stadiumX3 à anak menjadi buta
KLASIFIKASI KVA (Xeroftalmia)XNX1AX1BX2X3AX3BXSXF: Buta Senja: Xerosis konjungtiva: Bercak bitot: Xerosis kornea: Ulkus kornea dengan xerosis: Keratomalasia: Xeroftalmia scars: Xeroftalmia fundus
Sumber : Depkes RI & HKI, 2002
WHO Xerophthalmia Classification (1982)(Sommer & Davidson. J Nutr 2002)nnnnnXNX1BX2X3XSNight blindnessBitot’s spotsCorneal xerosis orCorneal ulceration/KeratomalaciaCorneal scarringSerum retinol( .70 umol/L/20 ug/dL)*WHO minimum criteria for public health significance( 1%) *( 0.5%)( 0.01%)( 0.05%)( 15%)
Continued Plasma Vit.A 0,35 µmol/l (10 µg/dl)Plasma Vit.A 20 µg/dlà rawan terhadappenyakit infeksi & me mortalitasn Liver Vit.A 5 µg/gn: 5%: 5%
Sumber : Depkes RI & HKI, 2002
CAUSES OF NIGHTBLIND WOMENSource : Christian et al: Int J Epidemiol 1998; Eur J Clin Nutr 1998; Am J Clin Nutr 1998; Soc Sci Med 1998; Am JEpidemiol 2000; J Nutr 2002; Katz et al, J Nutr 1995; Semba et al 2003
PENYEBAB KVAEXPOSUREOUTCOMEASUPANVITAMIN A KVA
PENYEBAB KVA :KURANGPENGETAHUAN &KEPERCAYAANKEADAANEKONOMIASUPAN VIT. ARENDAHNAFSU MAKANHILANGKVAPELARUT VIT. ARENDAHKEPABSORBSI &UTILISASI VIT. APENYAKIT INFEKSIPENYEBAB TIDAKLANGSUNGPENYEBABLANGSUNG
CONTINUED n DeplesiVitamin A dalam tubuh àproses laman Dimulai dengan persediaan Vit. Adalam hati habis à kadar Vit. Aplasma me à disfungsi retinaà perubahan jaringan epitel
Source : KP West in Semba & Bloem 2007, Johns Hopkins Bloomberg School of Public Health Baltimore, Maryland, April16th, 2007
Sumber : Depkes RI & HKI, 2002
Sumber : Depkes RI & HKI, 2002
CONTINUED n Bayiprematur à Cadangan Vit.Adalam hati rendahn Konsumsi alkohol & m’derita sakitliver à hati rusak à tidak mampumenyimpan banyak Vit. An Obat-2an yang merubah absorpsilemak menghambat absorpsi Vit. A
CONTINUED n Penderitadiare kronik, Chron’sdisease atau tidak cukup pankreas &kondisi malabsorpsi lemakn Di USA à KVA terjadi pada penderitasindrom malabsorpsi lemak/diet ketatspt anorexia nervosan Intake Zn tidak adekuat à simptomKVA krn Zn dibutuhkan u/ p’gunaanVit.A secara efisien
PENENTUAN KADAR VIT.An Apabilaterdapat kelainan mata àkadar vitamin A serum ( 5 µg/100ml) & kadar RBP ( 20 µg/100 ml)sudah sangat rendahn Konsentrasi Vit.A dalam hati àindikasi yang baik u/ menentukanstatus Vit.A
CONTINUED n Biopsihati à tindakan yangmengandung risiko bahayan Penentuan kadar Vit. A jaringantidak mudah dilakukann Konsentrasi Vit.A penderita KEPrendah 15 µg/gram jaringanhepar (Pujiadji, 1989)
BATASAN & INTERPRETASI PEMERIKSAANKADAR VITAMIN A DALAM DARAHUMUR (TAHUN)Semua UmurDEFISIENSI 10 µg/dlMARGIN10-20 µg/dlCUKUP 20 µg/dl
DAMPAK KVA PADA BALITAn1diantara 2 (48,1%) dari balita ygmenderita KVA à menderita anemiakurang zat besi(SKRT, 2001)n Anak-2 yang KVA pada derajatsedang berisiko tinggi untukmengalami gangguan pertumbuhan(Hadi et. al., 2000),
CONTINUED n Disamping itu à menderitabeberapa penyakit infeksiseperti campak & diaren KVA bertanggung-jawabterhadap 23% kematian anakbalita di seluruh dunia(Beaton, 1997)
EVALUASI PROGRAMPENANGGULANGAN KVAn Konsumsisayur & buah berwarnaà sangat penting, agar tidaktergantung pada kapsul Vitamin An Kasus xeropthalmia à p’yuluhankons. sayur & buah tidak efektif &cakupan kapsul Vitamin 80% àlaporan bbrp propinsi (NTB, Sumsel) th2000 & me morbiditas pada balita
Vitamin A Intake of Children 12-59 months ofage in Rural West Sumatera (Survey HKI, 2003)n Dietaryintake of vitamin A àimportant indicator of whether or nota chronic problem of VAD is likely toexist & indicates the need forinterventions to control VAD.n The severest forms of VAD à interms of clinical symptoms, whichinclude night blindness, ulceration ofthe cornea & full blindness.
CONTINUED .n 70%of children was estimatedblinded by VAD will die within theyear, & mortality rates 3-26% havebeen observed among children withcorneal disease.n Long before eye damage can beobserved, other body functions areimpaired
CONTINUED .n Thisincludes immune function, whichleads to increased morbidity &mortality, often even before theclinical eye signs of VAD have beenobserved.
Data Collection MethodnnnThe 24-hour Vitamin A Semi-Quantitative(VASQ) method developed by HKI was used toassess total VA intake for a 20% sub sample ofhouseholds.Mothers were asked to recall everything theirchild ate or drank in the last 24 hours, & detailsabout portion sizes & cooking methods wererecorded.Vitamin A intake was estimated based on portionsize and vitamin A content of the food.
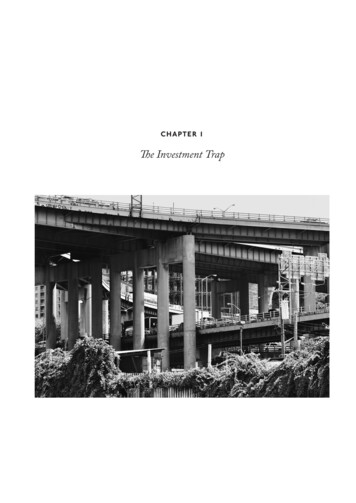
Findings:- Vitamin A intake was wellbelow the Indonesian RecommendedDaily Intake and has improved littleover time.n West Sumatra - Vitamin A intake inWest Sumatra was no more than onethird of the Recommended DailyIntake for childrenn General
Gambar. Asupan Vitamin A Anak Usia 12-59 blndi Pedesaan Sumatera BaratSumber : HKI, 2003
Vitamin A Capsule Coverage among Children6-59 Months of Age in Rural West Sumatra(Survey HKI, 2003)n Inrecognition VAD as a public healthproblem, the government of Indonesiahas set a target of 80% coverage withvitamin A capsules (VAC) amongchildren 6-59 months of age12.n All children in this group are toreceive age appropriate doses ofvitamin A twice a year.
CONTINUED .nAs there are two VA campaign distributionmonths each year (February & August),the achievement of this goal can beevaluated by estimating the level ofcoverage for each
IMPORTANCEn Supplementationwith VAC has beenshown to reduce clinical symptoms ofVAD such as xeropthalmia and toreduce morbidity, mortality, andblindness rates among children. InIndonesia, a 34% reduction inmortality was observed amongchildren supplemented with VAC
CONTINUED .nAmeta analysis of eight mortalitytrials indicated that improving VAstatus among children 6-59 monthsof age reduces all-cause mortalityby 23%
Findings:nnnGeneral - Vitamin A capsule coverage hasincreased considerably, reaching the target of80% coverage in August 02 and February 2003.West Sumatra - VAC coverage increased fromAugust 1999 to February 2002, but modestly.Highest coverage was still below 60% in bothage groups, which is much below the target of80%. No information is available for afterFebruary 2002.
Gambar. Pemberian Kapsul Vitamin A Anak Usia 6-59 blndi Pedesaan Sumatera BaratSumber : HKI, 2003
Total Vitamin A Intake among Non- PregnantMothers in Rural West SumateranLow total dietary vitamin A (VA) intakeamong populations where foodconsumption is the predominant source ofVA indicates that vitamin A deficiency islikely to exist.
Importance:n Importance:VAD has the sameconsequences for the mother as thechild.n These include increased morbidityand severity of illness, exacerbatedn anemia, and blindness and death(refer to Total Vitamin A Intakeamong Children 12-59 Months).
CONTINUED .nnnHowever, maternal deficiency has the addedconsequence of contributing to the poor healthstatus of the newborn.One study in rural Nepal found an increasedmortality rate of 63% among infants of nightblind women.Furthermore, VAD among lactating womenlowers the VA concentration of breast milk,which can lead to a VAD among breastfedinfants.
Data Collection MethodnnnThe 24- hour Vitamin A Semi- Quantitative(VASQ) method was used to assess total VAintake for a 20% sub sample of households.Mothers were asked to recall everything they ateor drank in the last 24 hours, and details aboutportion sizes and cooking methods wererecorded.Vitamin A intake was estimated based on portionsize and vitamin A content of the food
Findings:nnGeneral - Vitamin A intake among nonpregnantmothers was less than half of the IndonesianRecommended Daily Intake (even less formother that are lactating since their RDI ishigher) for every rural province in every round ofdata collection.West Sumatra – Vitamin A intake in WestSumatra was no more than 40% of theRecommended Daily Intake for non-pregnant,nonbreastfeeding women.
E-mail Contact :n Minda azri@fk.unand.ac.idn uniminda@yahoo.com
nMaternal Vitamin A Deficiency : 10% of women develop night blindness in latter half of pregnancy in poorly nourished South Asian populations. Maternal night blindness