Transcription
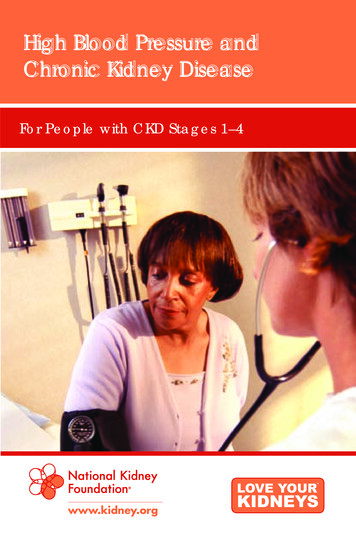
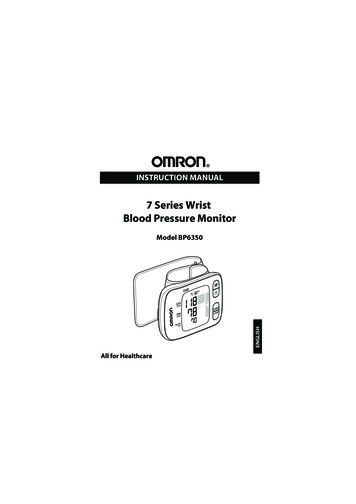
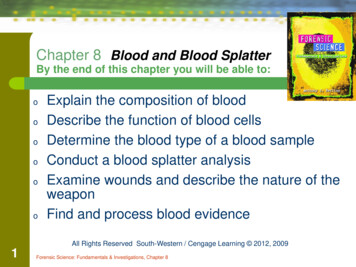
TODAY’S TECHNICIANPeer ReviewedBlood Pressure Monitoring from aNursing PerspectivePART 2: BLOOD PRESSUREMONITORING TECHNIQUESLila K. Sierra, CVT, VTS (ECC), and Emily Savino, BA, CVT, VTS (ECC)University of PennsylvaniaSystemic arterial blood pressure is created by thepumping action of the heart, circulating arterialblood volume, and the smooth muscle tone ofblood vessel walls.Arterial blood pressure is essential for adequateperfusion of tissues, delivering oxygen for energydemands. The ability to measure and monitorblood pressure trends provides important dataabout patient cardiovascular status and may helpdefine approach to treatment.Part 1 of this article series—Overview of BloodPressure Monitoring (January/February 2015issue)—discussed terms associated with bloodpressure measurement, indications for measurement,and normal and abnormal blood pressure values. Thissecond article describes types of blood pressuremonitors and provides step-by-step instructions onperforming blood pressure measurement.MONITORING TECHNIQUESArterial blood pressure can be measured in 2 ways:1. Direct arterial blood pressure (DABP)monitoring—considered the gold standard—uses anarterial catheter connected to a pressure transducer.This system allows continuous monitoring ofpatient systolic, diastolic, and mean arterial pressure(SAP, DAP, and MAP, respectively)1-3 and alsosimplifies collection of samples for arterial bloodgas analysis. However, DABP monitoring is notused as frequently as other methods because anarterial catheter must be placed.2. Indirect arterial blood pressure (IABP)monitoring relies on noninvasive detection ofarterial blood flow or vessel wall movement ina peripheral artery and provides intermittentmeasurements of arterial blood pressure.IABP monitoring is the most frequentlyused technique in clinical practice; the mostcommonly used indirect methods are Dopplerultrasonography and oscillometric bloodpressure monitoring. To obtain an IABPreading, a cuff is inflated over an artery untilarterial blood flow is occluded.1Normal arterial blood pressure values for adultdogs and cats are listed in Table 1.INDIRECT BLOOD PRESSUREMONITORING: Doppler UltrasonographyDoppler technology uses 10 MHz ultrasound wavesto detect blood flow in a peripheral artery (Figure1), which is then made audible via the probe/crystaland a speaker.1The Doppler technique does not provide ameasurement of MAPor DAP in smallanimals.1,4,5 Whilesome studies havereported that Dopplerreadings may moreclosely reflect MAPthan SAP in cats,1,3the most recent studyTABLE 1.Normal Arterial Blood Pressure Values in Adult Dogs & Cats4BLOOD PRESSURE VALUESDOGSCATSSystolic arterial pressure90 to 140 mm Hg80 to 140 mm HgDiastolic arterial pressure50 to 80 mm Hg55 to 75 mm HgMean arterial pressure60 to 100 mm Hg60 to 100 mm HgFIGURE 1. Doppler ultrasonographic bloodpressure measurement.tvpjournal.com March/April 2015 TODAY’S VETERINARY PRACTICE93
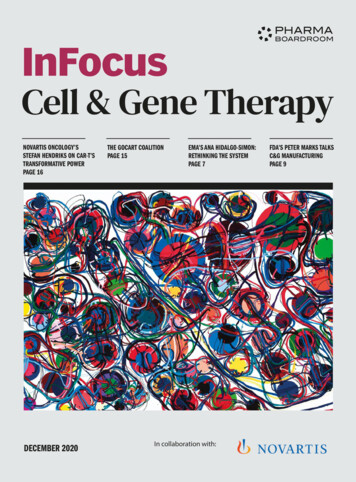
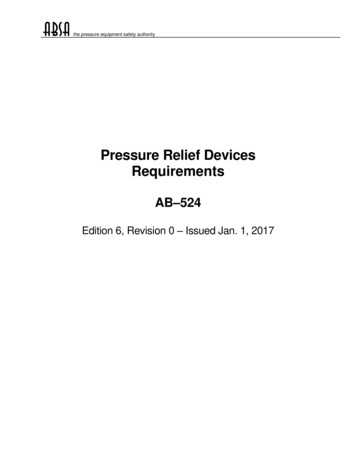
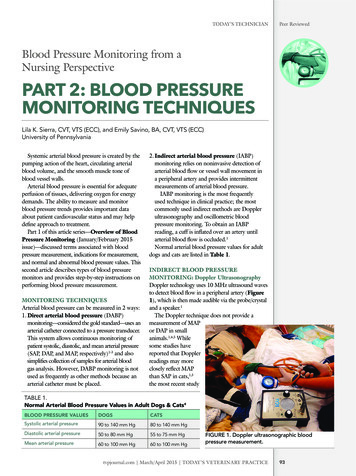
Peer ReviewedTODAY’S TECHNICIANFIGURE 2. The Doppler crystal, shown in this image, should be placed FIGURE 3. Oscillometric blood pressure monitorparallel to the artery’s blood flow.(Cardell 9401 Veterinary Monitor, midmark.com).was performed on healthy anesthetized cats.1Therefore, most clinicians consider that Dopplerreadings in awake animals estimate SAP.AdvantagesDoppler ultrasonography has several advantageswhen compared with other blood pressuremonitoring techniques; the technology is: Relatively easy to use, not requiring a great dealof expertise Affordable and readily available in most clinicalsettings Appropriate to use in patients with significanthypotension and cardiac arrhythmias1 Commonly used in small animals (cats, smalldogs, rabbits, ferrets, other exotic species).placed when pulsatile blood flow is audible.4. Connect a pressure cuff to a sphygmomanometerand place the cuff proximal to the Dopplerprobe.5. Inflate the cuff until the artery is occluded andDoppler sounds are no longer audible; thenslowly deflate the cuff, while observing thesphygmomanometer.6. Record the pressure at which the first audiblearterial pulse is heard as the SAP.7. Obtain several consecutive measurements;average the middle 3 readings, and record theaverage as the SAP. Make sure to use the samelimb and same size cuff for serial blood pressuremeasurements.Preventing Inaccurate ResultsBlood Pressure Measurement: Step by StepSeveral factors can result in erroneous readings:Table 2 lists the supplies needed for Doppler Cuff size is critically important to obtainultrasonographic blood pressure measurement.accurate Doppler readings.1,4,61. Select a peripheral artery for Doppler probe» A cuff that is too large falsely decreases theplacement; common locations include the dorsalreadingpedal artery, digital artery, andcoccygeal artery.TABLE 2.2. Clip the hair coat over theRequired Supplies for Doppler Measurementchosen artery, or wet it with Clippers or alcohol for either clipping or wetting hairalcohol, and apply ultrasound Doppler unit and sphygmomanometercoupling gel to the Doppler Ultrasound coupling gelprobe. Inflatable cuff, the width of which should be:3. Place the Doppler probe over» In dogs, 40% of the limb circumference» In cats, 30% of the limb circumferencethe artery, oriented parallel to Rubber tubing, which connects inflatable cuff and sphygmomanometerblood flow (Figure 2); the Earphones, if it is difficult to hear the Doppler signalprobe is considered correctly94TODAY’S VETERINARY PRACTICE March/April 2015 tvpjournal.com
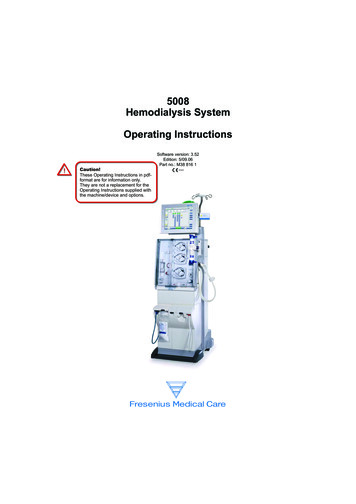
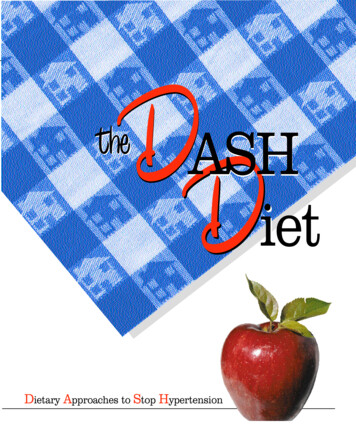
TODAY’S TECHNICIAN» A cuff that is too small falsely elevates thereading. Patients must be held/restrained during Dopplermeasurements; however, this handling mayincrease the animal’s blood pressure. Patient position during Doppler measurementcan contribute to inaccurate readings; ideally,patients should lie in lateral recumbency, withthe cuff positioned on the limb at the level of theright atrium.1,4 Obtaining Doppler measurements in patientswith severe peripheral vasoconstriction(hypovolemia, shock, significant hypothermia)can be difficult; therefore, accuracy of readingsin these patients can be affected by degree ofvasoconstriction.3,4to those used for Doppler blood pressuremeasurement.2. Once the device is started, the cuff automaticallyinflates to a pressure that occludes arterial bloodflow.3. As the cuff is deflated, the arterial walloscillations increase at SAP, maximize at MAP,and decrease at DAP.44. The oscillometric monitor display will shownumeric values for SAP, MAP, and DAP as wellas pulse rate.5. Compare the oscillometric pulse rate with amanually obtained pulse rate to determineaccuracy: if the rates do NOT match, it is likelythat the blood pressure readings on the monitorare inaccurate.INDIRECT BLOOD PRESSUREMONITORING: Oscillometric MeasurementOscillometric measurement (Figure 3) providesvalues for SAP, MAP, DAP, and pulse rate;therefore, this type of blood pressure monitoringprovides more information than Dopplermeasurement.1,3,4 Most oscillometric devicesmeasure the MAP; then calculate the SAP andDAP via programmed algorithms; therefore, theMAP is the most reliable reading.4Preventing Inaccurate ResultsAs discussed in the Indirect Blood PressureMonitoring: Doppler Ultrasonography section: Selection of an appropriately sized cuff is crucialto obtaining accurate values; cuff selection isoutlined in Table 2. To ensure accuracy, it is important to take severalconsecutive readings; then compare the readingsto ensure that the values are reproducible. Ideally, the same size cuff and same limb shouldbe used for all consecutive blood pressuremeasurements.AdvantagesOscillometric blood pressure measurement hasseveral advantages over Doppler methodology; the: Process is more automated, requiring lesstechnical skill; the operator simply chooses theappropriate cuff size, places it on the patient,and hits the start button Monitors can be programmed to measure bloodpressure at timed intervals (eg, Q 15 min) Automated nature of measurement helps ensurethat elevated values are less likely a result ofstressful patient handling.1,4Peer ReviewedDIRECT BLOOD PRESSUREMONITORINGIn general, DABP monitoring (Figure 4 andFigure 5, page 96) is indicated for any criticalpatient, but specific indications in the clinicalsetting include patients:DisadvantagesHowever, oscillometric techniques tend to be lessaccurate in patients:3,4 Under 5 kg With cardiac arrhythmias, significant tachycardiaor bradycardia, vasoconstriction, or hypothermia That are moving or shivering.Blood Pressure Measurement: Step by Step1. Place the cuff—attached to an oscillometricmonitor—on a distal artery; common locationsfor oscillometric cuff placement are similarFIGURE 4. Simultaneous electrocardiographyand direct arterial blood pressure readings(Escort Prism Patient Monitor, invivocorp.com)tvpjournal.com March/April 2015 TODAY’S VETERINARY PRACTICE95
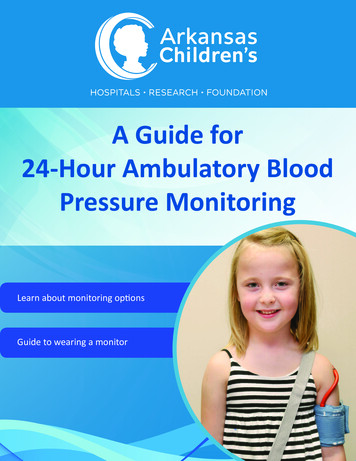
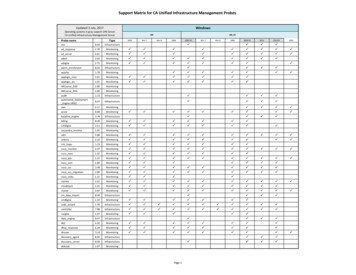
Peer ReviewedTODAY’S TECHNICIANcan be cost prohibitive, especially when not usedfrequently. Arterial catheters are invasive, and arterialaccess can be technically difficult to obtain andmaintain. Complications that can result from arterialcatheterization include bleeding from thecatheter insertion site, hematoma formation,significant hemorrhage if the system becomesdisconnected, infection, and arterial thrombosiswith possibility of necrosis of the tissues distal tothe catheter.FIGURE 5. Simultaneous electrocardiographyand direct arterial blood pressure readingsdemonstrated on a different monitor (PM-9000Vet Monitor, mindray.com). Presenting in hypovolemic or septic shock In congestive heart failure, especially whenreceiving powerful vasodilator medication forpurpose of afterload reduction Requiring vasopressors or mechanical ventilation Receiving medication for severe hypertension Demonstrating a high anesthetic risk.DABP monitoring is NOT indicated in healthy,ambulatory patients because these patients aremore likely to disconnect an arterial line, orremove the arterial catheter, increasing the risk forarterial hemorrhage.Blood Pressure Measurement: Step by StepTable 3 lists the supplies needed for DABPmeasurement (Figure 6).1. Place and secure an arterial catheter; commonsites for arterial catheterization include thedorsal pedal artery, coccygeal artery (Figures 7and 8), and medial auricular artery.1,22. Once the arterial catheter is placed and secured,connect it to the DABP monitoring system.3. At one end of the system—the end farthest awayfrom the patient—a fluid administration set isconnected to a heparinized bag of 0.9% sodiumchloride (Table 3).4. Pressurize the fluid bag to a range between 250and 300 mm Hg: the goal is to achieve a pressureAdvantagesDABP has many advantages over other methodsof blood pressure monitoring. Two of the mostimportant advantages include: “Real-time” monitoring of blood pressureand blood pressure trends, even in extremelyhypotensive patients; this up-to-the-minuteinformation about a patient’s hemodynamicstatus enables clinicians to gauge whether aspecific therapy is working or if additional,immediate intervention is necessary. Handling and restraint of the patient is usuallylimited to the initial arterial catheter placement;therefore, DABP values are less prone to falselyelevated readings related to stress of restraint andhandling.DisadvantagesHowever, DABP monitoring is not usedextensively because it has several drawbacks: The equipment necessary to monitor DABP (eg,pressure transducers, hemodynamic monitors)96FIGURE 6. DABP supplies: Transpac disposablepressure transducer (icumed.com), heparinizedsaline bag inside pressurized air bag, electroniccable to connect Transpac to monitor,transducer board (white), arterial catheter(dorsal metatarsal).TODAY’S VETERINARY PRACTICE March/April 2015 tvpjournal.com
TODAY’S TECHNICIANFIGURE 7. Patient with coccygeal arterial catheter; note that arterialcatheters should not be maintained in cats for longer than 6 to 12 hoursowing to risk for arterial thrombosis.in the fluid bag greater than the patient’s systolicpressure, which prevents back flow of arterialblood into the monitoring system.1,25. The fluid bag tubing connects to a pressuretransducer, which is connected by a cable to thephysiologic monitor, mounted on a board placedat the level of the patient’s heart. At the otherend of the transducer, semi-rigid tubing connectsto the arterial catheter’s T-set.6. Once the pressure transducer is connected to themonitor, zero it at the level of the patient’s rightatrium. Once zeroed, the pressure transducerconverts the pressure changes in the artery to anelectrical signal that is displayed on the monitoras a pressure wave form; numeric values for SAP,MAP, and DAP are also displayed.17. Flush the DABP monitoring system with heparinizedsaline before connecting it to the patient.8. Supervise patients with arterial catheters at alltimes and carefully care for the catheter: Clearly label the catheter, allowing easyidentification as arterial rather than venousand, thereby, alerting personnel NOT toadminister medications through the catheter. Rewrap the catheter, at a minimum, oncedaily; rewrap soiled catheters promptly. While the catheter is unwrapped, evaluate theinsertion site for redness, warmth, swelling,pain, or discharge; remove catheters that arepainful or oozing from the insertion site. Document when the catheter is rewrappedand note the appearance of the insertion sitein the medical record. Consider putting an E-collar on patients toPeer ReviewedFIGURE 8. Close-up image of coccygeal arterialcatheter in a cat.TABLE 3.Required Supplies for DABP Measurement Arterial catheterT-set primed with heparinized salineDABP transducer system primed with heparinized salineTransducer cablePhysiologic monitor that displays DABP wave form and numeric values for SAP,DAP, and MAP 250-mL bag of heparinized saline (1 U heparin/1 mL 0.9% sodium chloride) Pressure bag Board for stabilization of the transducerprevent access to arterial catheters. Do NOT maintain arterial catheters in cats forlonger than 6 to 12 hours1 owing to increasedrisk for arterial thrombosis.Preventing Inaccurate ResultsAlthough DABP is considered the gold standard inblood pressure monitoring, a number of situationscan cause erroneous readings, which can beprevented by: Using only semi-rigid tubing to connect thepressure transducer to the patient—the use ofcompliant tubing results in excessive damping ofthe pressure wave, causing inaccurate readings Ensuring air bubbles are not present in the system Checking the semi-rigid tubing for kinks Making sure the pressure bag is inflated to atleast 250 mm Hg Reassessing the transducer level; if thetransducer is displaced, replace it toapproximately the level of the right atrium andzero to the patient Ensuring that the arterial catheter is patent;flush the arterial catheter if needed.tvpjournal.com March/April 2015 TODAY’S VETERINARY PRACTICELearn MoreVisit TVPjournal.comand select Resourcesto read BloodPressure Monitoring:The NursingThought Process,which outlines the 5steps of the nursingprocess and how theyhelp the veterinaryteam prioritize,troubleshoot, andsolve issues relatedto blood pressuremeasurement andmonitoring beforethey become anemergency.97
Peer ReviewedTODAY’S TECHNICIANIN SUMMARYVeterinary nurses play a fundamental role in patientcare. Appropriately monitoring patient blood pressure,documenting results, interpreting them, and communicatingchanges and concerns to the clinician provides all membersof the veterinary team with an opportunity to proactivelymanage potential problems.DABP direct arterial blood pressure; DAP diastolicarterial pressure; IABP indirect arterial blood pressure;MAP mean arterial pressure; SAP systolic arterialpressureReferences1. Waddell LS, Brown AJ. Hemodynamic monitoring. In Silverstein DC,Hopper K (eds): Small Animal Critical Care Medicine, 2nd ed. St.Louis: Elsevier, 2015, pp 957-9622. Cooper E, Cooper S. Direct systemic arterial blood pressuremonitoring. In Burkitt Creedon JM, Davis H (eds): AdvancedMonitoring and Procedures for Small Animal Emergency and CriticalCare. Ames, IA: Wiley-Blackwell, 2012, pp 122-133.3. Cooper E. Hypotension. In Silverstein DC, Hopper K (eds): SmallAnimal Critical Care Medicine, 2nd ed. St. Louis: Elsevier, 2015, pp46-50.4. Williamson JA, Leone S. Noninvasive arterial blood pressuremonitoring. In Burkitt Creedon JM, Davis H (eds): AdvancedMonitoring and Procedures for Small Animal Emergency and CriticalCare, Ames, IA: Wiley-Blackwell, 2012, pp 134-144.5. Caulkett NA, Cantwell SL, Houston DM. A comparision of indirectblood pressure monitoring techniques in the anesthetized cat. Vet Surg1998; 27:370.6. Monnet E. Cardiovascular monitoring. In Wingfield WE, Raffe MR(eds): The Veterinary ICU Book. Jackson, WY: Teton NewMedia, 2002,pp 265-280.LILA K. SIERRALila K. Sierra, CVT, VTS (Emergency andCritical Care) is the assistant nursingsupervisor of the intensive care unit atMatthew J. Ryan Veterinary Hospital ofUniversity of Pennsylvania. She has lecturedat state conferences and has publishedchapters in various veterinary manuals. Herpassion lies in all aspects of advanced nursingcare, including patient advocacy, innovativenursing development, and education ofprospective veterinarians and nurses.EMILY SAVINOEmily Savino, BA, CVT, VTS (Emergencyand Critical Care) is the nursing supervisorof the intensive care unit at Matthew J.Ryan Veterinary Hospital of University ofPennsylvania. She has lectured on veterinarycritical care nursing at conferences andhas published chapters in veterinary texts.She enjoys teaching new veterinary nursesthe art of “critical thinking” and working inan environment where she is learning newthings every day.(See Heartgard ad on back cover)98TODAY’S VETERINARY PRACTICE March/April 2015
TODAY'S TECHNICIAN Peer Reviewed 97 in the fl uid bag greater than the patient's systolic pressure, which prevents back fl ow of arterial blood into the monitoring system.1,2 5. The fl uid bag tubing connects to a pressure transducer, which is connected by a cable to the