Transcription
001 ca0112 Corneal Atlas ah.indd 112/20/11 3:42 PM
Ernest Bowling, OD, FAAO, is in private practice in Gadsden, AL, and is associate clinicaleditor of Review of Cornea & Contact Lenses.E-mail him at drbowling@windstream.net.Table of ContentsBacterial . 4Viral .5Acanthamoeba Keratitis . 7Jeffrey Sonsino, OD, FAAO, is an assistantprofessor at Vanderbilt Eye Institute in Nashville,TN. He is a candidate for Diplomate in ContactLenses of the American Academy of Optometry,chair of the American Optometric Association’sAnterior Segment Committee and chief editor ofthe Contact Lens Section Newsletter.Fungal . 8Epithelial . 9Bowman’s . 10Joseph P. Shovlin, OD, FAAO, is in privatepractice in Scranton, PA, associate clinical editor of Review of Optometry and clinical editorof Review of Cornea and Contact Lenses.E-mail him at jpshovlin@gmail.com.Stroma . 11Endothelium . 14Degenerations . 16Mechanical . 17Christine W. Sindt, OD, FAAO, is Director ofContact Lens Service and Associate ClinicalProfessor at the University of Iowa Hospitalsand Clinics, Iowa City, IA, immediate past Chairof the AOA Contact Lens and Cornea Council,a monthly columnist for Review of Corneaand Contact Lenses, co-clinical editor forReview of Optometry, and photo editor for theCorneal Atlas. E-mail her at christine-sindt@uiowa.edu.59Chemical . 19Inflammatory . 21141721REVIEW OF OPTOMETRY001 ca0112 Corneal Atlas FINAL.indd 3January 201231/6/12 4:30 PM
BacterialEtiologyMicrobial keratitis is the most visually devastating complication associated with contactlens wear. While even daily wear of contactlenses carries an increased risk for infection,extended or overnight contact lens wear isthe greatest risk factor for infectious keratitisin patients choosing to wear contact lenses.1Microbial contamination of CL storage casesis a great risk for gram-negative bacterial infection among soft CL wearers.2 Many bacteriahave been identified in contact lens relatedmicrobial keratitis, with the most commonorganisms cultured from bacterial ulcersbeing Staphylococcus, Streptococcus, Pseudomonasand Moraxella.3 The gram-negative rodPseudomonas aeruginosa is commonly associated with microbial keratitis in soft contact lenswear but a higher incidence of gram-positiveorganisms than gram-negative organisms arerecovered by culture from infections associated with contact lens wear.4,5 It is importantto remember that the organisms Neisseriagonorrhoeae, Listeria, Corynebacterium andHaemophilus aegypticus do not require damage to the cornea and may invade directlythrough intact corneal epithelium.6PresentationPatients with microbial keratitis presentwith symptoms including decreased vision,photophobia, moderate to severe ocularpain, redness, swelling and discharge. Onslit lamp examination, the critical finding isa focal white opacity in the corneal stromawith an overlying corneal epithelial defectthat stains with fluorescein.3 Additionalfindings include diffuse epithelial edema,stromal infiltration surrounding the ulceration, and mucopurulent exudation. Ananterior chamber reaction and hypopyonmay be present. It is important to documentthe depth and location of the epithelialdefect and stromal infiltration. The anteriorchamber should be evaluated for cells andflare and examined for a hypopyon, and theintraocular pressure should be checked.Staph. marginal keratitisBacterial ulcerBacterial infectionMuch has been made regarding cultureand sensitivity testing in cases of microbialkeratitis. In general, consider cultures in ulcersgreater than 1mm to 2mm, defects in thevisual axis, ulcers unresponsive to initial therapy, or if an unusual organism is suspected.Remember that just approximately 40% ofcorneal cultures indentify causative pathogens. For this reason, culturing the contactlens and contact lens storage case in additionto scraping the corneal ulcer can aid in identifying the causative organism.7Ulcers need to be considered infectiousuntil proven otherwise. Therapy begins withimmediate, intensive, aggressive treatmentwith fourth generation fluoroquinoloneswhile awaiting lab results. Dosage is every30 minutes for the first six hours, followedby hourly administration around the clockuntil improvement is noted. The applicationof fourth-generation fluoroquinolones inthe treatment of corneal ulcers is an off-labeluse of these medications, but routinely performed. Also, no difference in efficacy withthe use of fourth-generation fluoroquinolonemonotherapy when compared with combination therapy of fortified antibiotics has beennoted.8 Cycloplegic drops are valuable forpatient comfort and to prevent synechiae formation in accompanying iritis.AVOID STEROIDS! Especially initially.Corticosteroid treatment resulted in a statistically significant delay in corneal re-epithelialization and steroid use did not translateto a significant difference in visual acuity orinfiltrate/scar size.9 Infectious keratitis mayworsen with topical steroid use, especiallywhen caused by fungus, atypical Mycobacteriaor Pseudomonas. Once the cornea has re- epithelialized and the causative organism hasdemonstrated sensitivity to the antibiotic(usually after 72 hours of treatment), a steroidmay be added to the therapeutic regimen tocontrol persistent inflammation and reducetissue damage. However, the results of thesteroids in corneal ulcers trial (SCUT) studyshowed that adjunctive topical corticosteroid did not improve three-month vision inpatients with bacterial corneal ulcers.10 Thepatient with an infectious keratitis needs tobe followed daily, with careful monitoring ofthe findings. The antibiotic regimen shouldBacterial infectionBacterial keratitisTreatment4 January 2012 REVIEW OF OPTOMETRY001 ca0112 Corneal Atlas FINAL.indd 41/6/12 4:31 PM
be reduced depending on the response, butshould never be tapered below the minimumdose (usually q.i.d. to t.i.d) to prevent thepossibility of bacterial resistance.ICD-9 Codes 370.00 Corneal ulcer, unspecified 370.01 Marginal corneal ulcer 370.02 Ring corneal ulcer 370.03 Central corneal ulcer 370.04 Hypopyon ulcer 370.05 Mycotic corneal ulcer 370.06 Perforated corneal ulcer 371.00 Corneal opacity/scar,unspecified (upon resolution)References1. Keay L, Stapleton F, Schein O. Epidemiology of con- tactlens related inflammation and microbial keratitis: A 20-yearperspective. Eye Cont Lens 2007; 33: 346-353.2. Bharathi MJ, Ramakrishnan R, et al. Ulcerative keratitisassociated with contact lens wear. Indian J Ophthalmol 2007;55: 64-67.3. Ehlers JP, Shah CP, eds. The Wills Eye Manual: Office andEmergency Room Diagnosis and Treatment of Eye 5th ed.Philadelphia: Lippincott Williams & Wilkins, 2008: 62-66.4. Green M, Apel A, Stapleton F. Risk factors and causativeorganisms in microbial keratitis. Cornea 2008; 27: 22-27.5. Jeng BH, McLeod SD. Microbial keratitis. Br J Ophthalmol2003; 87: 805–806.6. Reed WP, Williams RC. Bacterial adherence: First step inpathogenesis of certain infections. J Chronic Dis 1978; 31:67.7. Das S, Sheorey H, Taylor HR, et al. Association betweencultures of contact lens and corneal scraping in contact lensBacterial keratitisrelated microbial keratitis. Arch Ophthalmol 2007; 125: 11821185.8. Shah VM, Tandon R, Satpathy G, et al. Randomized clinical study for comparative evaluation of fourth-generationfluoroquinolones with the combination of fortified antibioticsin the treatment of bacterial corneal ulcers. Cornea 2010; 29:751-757.9. Srinivasan M, Lalitha P, Mahalakshmi R,et al.Corticosteroids for Bacterial Corneal Ulcers. Br J Ophthalmol2009; 93(2):198-202.10. Srinivasan M, Mascarenhas J, Rajaraman R, et al.Corticosteroids for Bacterial Keratitis: The Steroids for CornealUlcers Trial (SCUT). Arch Ophthalmol 2011 Oct 10. [Epubahead of print].Viral InfectionsADENOVIRAL KERATOCONJUNCTIVITISEtiologyAdenoviruses produce the most commonviral conjunctival infections.1 The conditionis quite contagious and is transmitted readilyin respiratory and ocular secretions, eye droppers and mascara bottles, and contaminatedswimming pools. The incubation period isusually five to 12 days, and the clinical illnessis present from five to 15 days. Most casesof viral conjunctivitis resolve spontaneously,without sequelae, within days to weeks.There are four forms of adenoviralconjunctivitis: Follicular conjunctivitis,pharyngoconjunctival fever, epidemic keratoconjunctivitis (EKC) and acute hemorrhagicconjunctivitis.2 Follicular conjunctivitis isthe mildest form of adenoviral conjunctivitis. Pharyngoconjunctival fever is the mostcommon ocular adenoviral infection and ischaracterized by a combination of pharyngitis, fever, and conjunctivitis. EKC is a moresevere form of conjunctivitis and typicallylasts for seven to 21days. EKC can affect thecornea with coarse keratitis and sub-epithelialinfiltrates (SEIs). SEIs may last for months,affecting visual acuity. Acute hemorrhagicconjunctivitis produces a severe, painful follicular con- junctivitis with the developmentof tiny subconjunctival hemorrhages.may be swollen. Inferior palpebral conjunctival follicles are seen. Pinpoint subconjunctival hemorrhages and membrane formationover the palpebral conjunctiva are occasionally seen. In some cases multiple, focal infiltrates in the cornea anterior to mid-stromamay be seen. A pre-auricular lymphadenopathy is present. A rapid, in-office immunodiagnostic test using antigen detection is available for adenovirus conjunctivitis. In a studyof 186 patients with acute conjunctivitis, thistest had a sensitivity of 88% to 89% and aspecificity of 91% to 94%.3TreatmentPalliative therapy is often sufficient formost cases of adenoviral conjunctivitis: coldcompresses, artificial tears and topical decongestants/antihistamines. 5% Betadine isnow available as an FDA-approved productwhich can be used “off-label” to treat EKC.This agent has minimal toxicity when usedproperly and followed by saline irrigation.In vitro, povidone iodine is effective againstHERPES SIMPLEX KERATITISEtiologyThe herpes simplex virus (HSV) is theleading cause of vision loss in the UnitedStates. Keratitis caused by HSV is also themost common cause of cornea-derived blindness in developed nations.4 The HSV is aDNA virus that resides latent in the trigeminal ganglion, only to resurrect during periodsof intense stress, illness, irritation and phototoxic exposure. The disease can be present assuperficial lesions, neurotrophic disease, orwith deep stromal involvement.PresentationPresentationIn general, viral infections present withredness, irritation, itching, foreign body sensation, tearing and photophobia. The condition starts in one eye and then progressesto the other a few days later. Signs includeconjunctival injection and swelling. The lidsadenovirus as well as many other infectiousagents. Topical steroids are indicated whenthe visual axis is involved or membraneor pseudo-membrane formation is noted.Patients should discontinue contact lenswear. Avoid the use of topical and oral antibiotic or antiviral agents as these will nothelp resolution and may promote antibioticresistance. Patients with adenoviral conjunctivitis need to understand that the conditionis highly contagious and should be informedof appropriate measures to reduce the risk ofspreading the infection to their other eye orto other people.Viral infectionPatients with HSV infection present withrapid onset unilateral pain and redness,watering and light sensitivity. Diagnosis ofHSV infection is primarily based on clinicalfindings. The disease starts as a punctuateepithelial keratitis, coalescing into the classicbranching epithelial ulceration with terminal end bulbs within 24 to 48 hours.5 TheREVIEW OF OPTOMETRY001 ca0112 Corneal Atlas FINAL.indd 5January 201251/6/12 4:31 PM
dendrites stain with rose bengal or lissaminegreen. Corneal sensitivity may be decreased.The neurotrophic form of HSV disease ischaracterized by areas of intense punctatechange or epithelial denudement, and canresult in corneal scarring. Deep stromallesions appear as a round, fluid filled circle.Scarring can develop in later stages with lossof stromal thickness and corneal thinning.TreatmentTreatment of active HSV keratitis consistsof topical trifluridine 1% solution every oneto two hours until no sign of active infection(lack of dendrite patterns), then five timesa day for an additional seven to 10 days.6Zirgan (ganciclovir) ophthalmic gel 0.15% isindicated for the treatment of acute herpetickeratitis. The recommended dosing regimenfor Zirgan is one drop in the affected eyefive times per day (approximately every threehours while awake) until the corneal ulcerheals, and then one drop three times per dayfor seven days.7Topical acyclovir 3% ointment (no longercommercially available, but can be obtainedfrom specialized compounding pharmacies)used five times a day as an alternative inpatients with a known sensitivity to the abovemedications.Oral antivirals are gaining use in the treatment of epithelial disease. Acyclovir 400mgfive times a day is the most common oraldosage. Alternatively, oral valacyclovir (valtrex), a prodrug of acyclovir, can be given500mg three times a day. Since these drugsare cleared through the kidneys, it is criticallyimportant for the patient with renal diseasethat the patient’s nephrologist or primary carephysician and/or pharmacist be consultedregarding dosing. For a patient on long-termoral antiviral therapy for recurrent disease,check creatinine levels to insure there is nokidney damage. Normal levels of serum creatinine are approximately 0.8mg to 1.4mg perdeciliter in adults.Finally, consider oral antiviral prophylaxis.Oral antiviral prophylaxis has been associatedwith a decreased risk of recurrence of epithelial keratitis, stromal keratitis, conjunctivitis,and blepharitis due to HSV.8HERPES ZOSTER OPHTHALMICUSEtiologyHerpes Zoster Ophthalmicus (HZO) isa recurrent infection of the varicella zoster(chickenpox) virus in the ophthalmic divisionof the trigeminal dermatome, most oftenaffecting the nasociliary branch. HZO canaffect any of the ocular and adnexal tissues.One in four people will contract herpes zosterin their lifetime, with this risk rising markedlyafter 50 years of age, especially in very elderlyindividuals.9 Ophthalmic herpes zoster represents 10% to 20% of all zoster cases.10PresentationHZO usually begins as an influenza-likeillness characterized by fatigue, malaise, nausea and mild fever accompanied by progressive pain and skin hyperesthesia. A diffuseerythematous or maculopapular rash appearsover a single dermatome three to five dayslater. The skin of the forehead and uppereyelid is commonly affected and strictlyobeys the midline with involvement of oneor more branches of the ophthalmic division of the trigeminal nerve. Involvement ofthe tip of the nose (Hutchinson’s sign) hasbeen thought to be a clinical predictor ofocular involvement. Although patients witha positive Hutchinson’s sign have twice theincidence of ocular involvement, one thirdof patients without the sign develop ocularmanifestations.11 HZO conjunctivitis is acommon ocular finding and the conjunctivaappears swollen and injected, with occasional vesicles and petechial hemorrhages.Herpes zoster keratitis manifests in five basicclinical forms: Epithelial keratitis (acute or chronic).Multiple, fine, raised intraepithelial lesionslocated paracentrally or at the limbus, whichstain mildly with fluorescein but intenselywith rose Bengal. Nummular stromal keratitis. Multiple,fine, granular infiltrates in the anterior corneal stroma. Disciform keratitis. A central, well- defined,disc-shaped area of diffuse stromal edemawithout vascularization. Corneal edema withanterior chamber inflammation. Limbal vascular keratitis. Limbal-vesselingrowth and stromal edema. May be associated with adjacent episcleral or scleralinflammation. Neurotrophic keratitis. An inferior, ovalepithelial defect with rolled edges. Can leadto corneal perforation.HZO can cause either a nongranulomatous or granulomatous anterior uveitis withkeratic precipitates and posterior synechiae.The diagnosis of herpes zoster disease is generally based on clinical findings.TreatmentAll patients with ophthalmic zoster,irrespective of age or severity of symptoms,should be prescribed oral antiviral drugs atthe first sign of disease. Patients with HZOare treated with oral acyclovir (800mg, fivetimes daily) for seven to 10 days. Early treatment with acyclovir (within 72 hours afterrash onset) reduces the percentage of eyedisorders in ophthalmic zoster patients from50% down to 20% to 30% and also lessensacute pain.12 Famciclovir 500mg three timesdaily for seven days or valacyclovir 1,000mgthree times daily are alternatives to acyclovir.In general, the dosages for HZO are twicethat for HSV infections. Palliative therapyincluding cool compresses, mechanicalcleansing of the involved skin and topicalantibiotic ointment without steroid are helpful in treating skin lesions. Epithelial defectsassociated with HZO keratitis may be treatedwith nonpreserved artificial tears, eye ointments, punctal occlusion, pressure patching,or therapeutic soft contact lenses. Topicalsteroids are useful in the management of keratouveitis, interstitial keratitis, anterior stromalinfiltrates, and dis-iform keratitis. Topicalcycloplegics prevent ciliary spasm associatedwith herpes zoster inflammatory disease.Aqueous suppressants and topical corticosteroids should be used to treat glaucoma associated with HZ disease. Consider zostavaxvaccine for your patients over 60 years of age.In the landmark Shingles Prevention Study,the live attenuated Varicella Zoster Virus vaccine reduced the risk of developing shinglesby 51%.13ICD-9 Codes 372.00 Unspecified conjunctivitis 372.02 Acute follicular conjunctivitis 372.03 Other mucopurulentconjunctivitis 372.04 Pseudomembranousconjunctivitis 372.11 Simple chronic conjunctivitis 077.1 Epidemic keratoconjunctivitis 077.3 Adenoviral (acute follicular)References1. Gordon, JS; Aoki, K; Kinchington, PR. Adenovirus keratoconjunctivitis. In: Pepose JS, Holland GN, Wilhelmus KR, eds.Ocular Infection and Immunity. St. Louis: Mosby;1996. pp.877–94.2. Yanoff M, Duker JS, eds. Ophthalmology, 3rd ed. MarylandHeights, MO, Elsevier, 2009.3. Sambursky R, Tauber S, Schirra F, et al. The RPSadeno detector for diagnosing adenoviral conjunctivitis.Ophthalmology 2006;113:1758-64.4. Guess S, Stone DU, Chodosh J. Evidence-based treatmentof herpes simplex virus keratitis: a systematic review. OculSurf2007; 5(3): 240-50.5. Kahn BF, Pavan-Langston D. Clinical manifestations andtreatment modalities in herpes simplex virus of the ocularanterior segment. Int Ophthalmol Clin 2004;44:103-33.6 Ehlers JP, Shah CP, eds. The Wills Eye Manual: Office andEmergency Room Diagnosis and Treatment of Eye Disease,5th Ed. Philadelphia, PA: Lippincott, Willliams and Wilkins, 2008.7. Zirgan package insert. Bausch Lomb Pharmaceuticals.8. Young RC, Hodge DO, Liesegang TJ, et al. Incidence,recurrence, and outcomes of herpes simplex virus eye diseasein Olmsted County, Minnesota, 1976-2007: the effect of oralantiviral prophylaxis. Arch Ophthalmol 2010;128(9):1178-83.9. Johnson RW, Bouhassira D, Kassianos G ,et al. The impactof herpes zoster and post-herpetic neuralgia on quality-of-life.BMC Med 2010;8:37.10. Ragozzino MW, Melton LJ 3rd, Kurland LT, et al.Population-based study of herpes zoster and its sequelae.Medicine (Baltimore) 1982;61:310-16.11. Harding SP, Lipton JR, Wells JC. Natural history of herpeszoster ophthalmicus: predictors of postherpetic neuralgia andocular involvement. Br J Ophthalmol 1987;71:353–58.12. Cobo LM, Foulks GN, Liesegang T, et al. Oral acyclovir in the treatment of acute herpes zoster ophthalmicus.Ophthalmology 1986; 93:763-70.13. Oxman MN, Levin MJ, Johnson GR, et al. A vaccine toprevent herpes zoster and postherpetic neuralgia in olderadults. N Engl J Med 2005; 352:2271-84.6 January 2012 REVIEW OF OPTOMETRY001 ca0112 Corneal Atlas FINAL.indd 61/6/12 4:31 PM
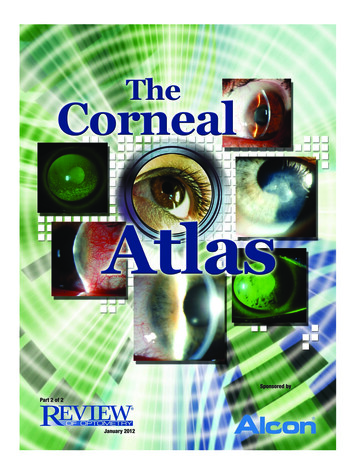
Acanthamoeba KeratitisBackgroundAcanthamoeba keratitis can be severe andvision-threatening. It was first recognized incontact lens wearers in the early 1970s, andcontact lens wear is thought to be associated with 80% of the cases.1,2 Symptomonset is greatest during the summer months.Acanthamoeba species are found in virtually every environment. These protozoa areubiquitous in the soil, dust, lakes, rivers, hottubs and salt water. They have been isolatedfrom heating, venting and air conditionerunits, humidifiers, dialysis units and contactlens paraphernalia. Acanthamoeba have beenfound in the nose and throat of healthypeople as well as those with compromisedimmune systems. Contact lens wear and poorlens hygiene are often singled out as the biggest risk factors for acanthamoeba keratitis. Thetrue incidence is not known; however, it isthought to be rare; affecting approximately1.65-2.01 per million contact lens wearers peryear in the United States.3 Although, it hasbeen reported as high as 1/30000 contact lenswearers per year outside the United States.4EtiologyThere are more than 20 different species,several of which are known to cause infections in humans, including A. culbertsoni, A.polyphaga, A. castellanii, A. healyi, (A. astronyxis), A. hatchetti and A. rhysodes. A. castellaniiis the most common amoeba associated withcorneal infec tion. The life cycle of theseorganisms is comprised of two stages, trophozoite and cystic forms. Trophozoites bind toand desquamate the corneal epithelium. Theysecrete a variety of proteases, which facilitatethe dissolution of the corneal stroma.5 Whenenvironmental conditions become unfavorable, the organism converts to a dormantcystic form, which is able to survive manyyears. These double walled cysts are highlyresistant to killing by desiccation, freeze/thaw cycles, irradiation, chlorination levelsand antimicrobial agents. Co-infection withbacteria or fungi is common, providing foodfor amoeba.PresentationAcanthamoeba keratitis presents with pain(ranging from mild foreign body sensation tosevere pain), photophobia, decreased vision,injection, irritation, tearing and a protractedclinical course. The patient often presentswith a unilateral red eye, where the pain isdisproportionately worse than one wouldsurmise from the clinical appearance. Earlycorneal findings include irregular epithelium,punctuate epithelial erosions, microcysticedema, perilimbal injection and dendritiformAcanthamoeba keratitisEarly presentation of Acanthamoeba keratitisepithelial lesions. The dendritiform lesionsoften resemble those of herpes simplex keratitis, however, the Acanthamoeba lesions appearedematous and necrotic rather than frankulcerations.A ring infiltrate is classically thought of asthe defining sign of Acanthamoeba kerititis;however, it tends to form four to eight weeksafter onset of symptoms and is rarely thepresenting sign. Radial perineuritis (perhapsexplaining the intense pain) may be seen onslit lamp examination or confocal microscopy. Unchecked, there may be progressivecorneal thinning and risk of perforation. Upto 40% of patients may have mild to severeanterior uveitis. Scleritis has been reported inpatients with Acanthamoeba keratitis; however,the scleral inflammation was attributed to animmune-mediated response to necrotic organisms and was not believed to be the result ofactive infection.6-8Severe glaucoma has been associatedwith Acanthamoeba keratitis secondary toan inflammatory angle-closure mechanism,apparently without direct infiltration of theorganism.9TreatmentDiagnosis largely depends on the ability tovisualize the organism. Definitive diagnosis ismade by corneal scrapings. Confocal microscopy is clinically useful to quickly identifythe organism in vivo. Attempts to culture theorganism is time- consuming and expensive,often with poor yields. Polymerase ChainReaction may be beneficial for identifyingamoeba in the future.10Differential diagnosis includes herpetickeratitis, bacterial keratitis, toxic keratopathy (solution related), stem cell failure,fungal keratitis, severe dry eye and contactlens related corneal oxygen deficiency.Debridement, particularly early in the disease, will reduce the number of organismsand deprive the Acanthamoeba of its foodsupply.11 Cationic antiseptic agents, such aschlohexidine 0.02% and polyhexamethylbiguanide 0.02%, are generally consideredprimary medical treatments. Biguanidesdisrupt the phospholipid structure of cellmembranes. Aromatic diamides (Brolene)directly affect the amoebas’ nucleic acidsand are thought to have a synergisticaffect with the biguanides. There is a riskof significant corneal epithelial toxicitywith q1-2h dosing.12,13 Corticosteroids areused to treat associated uvetitis or scleritis;however, this should be done with extremecaution because trophozoite proliferationhas been observed when exposed to steroids.14 Penetrating keratoplasty (PKP) maybe necessary for tectonic or optical cornealrehabilitation. In most situations, PKP ispostponed until resolution of infection.15,16There may be residual dormant cysts in theperipheral corneal, even in a cornea thatappears quiet, which may incite infectionafter graft. After corneal transplant, protective, maintenance doses of medicationshould be used to help prevent the recurrence of the acanthamoeba infection.17Recommendations: Avoid swimming with contact lenses on. Showering in contact lenses may increaserisk of infection.15 Careful following of recommended lenscare systems.ICD-9 Codes 370.02 Ring corneal ulcer 370.40-006.8 KeratoconjunctivitisReferences:1. Jones DB, Visvesvara GS, Robinson NM.Acanthamoeba polyphaga keratitis and Acanthamoebauveitis associated with fatal meningoencephalitis.Transactions of the ophthalmological societies of theUnited Kingdom 1975, 95(2):221-232.2. Illingworth CD, Cook SD, Karabatsas CH, Easty DL.REVIEW OF OPTOMETRY001 ca0112 Corneal Atlas FINAL.indd 7January 201271/6/12 4:31 PM
Acanthamoeba keratitis: risk factors and outcome. Br JOphthalmol. 1995 Dec;79(12):1078-82.3. Schaumberg DA, Snow KK, Dana MR. The epidemicof Acanthamoeba keratitis: where do we stand? Cornea.1998 Jan;17(1):3-10. Review.4. Seal DV. Acanthamoeba keratitis update-incidence,molec- ular epidemiology and new drugs for treatment.Eye. 2003 Nov;17(8):893-905. Review. 5. InvestigativeOphthalmology & Visual Science, July 2005, Vol. 46, No. 7.6. Lee GA, Gray TB, Dart JK, et al. Acanthamoebasclero-keratitis: treatment with systemic immunosuppression. Ophthalmology. 2002;109:1178-1182. 7. GarnerA. Pathogenesis of Acanthamoeba keratitis: hypothesis based on a histological analysis of 30 cases. Br JOphthalmol. 1993;77:366-370.8. Lindquist TD, Fritsche TR, Grutzmacher RD. Scleral ectasiasecondary to Acanthamoeba keratitis. Cornea. 1990;9:74-76.9. Kelley PS, Dossey AP, Patel D, Whitson JT, HoganRN, Cavanagh HD. Secondary glaucoma associated withadvanced Acanthamoeba keratitis. Eye Contact Lens.2006 Jul;32(4):178-82.10. Laummaunwai P, Ruangjirachuporn W, Boonmars T.A simple PCR condition for detection of a single cystof Acanthamoeba species. Parasitol Res. 2011 Oct 12.[Epub ahead of print]11. Lindquist TD. Treatment of Acanthamoeba keratitis.Cornea. 1998 Jan;17(1):11-6.12. Seal D. Treatment of Acanthamoeba keratitis. ExpertRev Anti Infect Ther. 2003 Aug;1(2):205-8. Review.13. Hammersmith KM. Diagnosis and management ofAcanthamoeba keratitis. Curr Opin Ophthalmol. 2006Aug;17(4):327-31.14. McClellan K, Howard K, Niederkorn JY, Alizadeh H.Effect of steroids on Acanthamoeba cysts and trophozoites. Invest Ophthalmol Vis Sci. 2001 Nov;42(12):2885-93.15. Oldenburg, CE, Acharya NR, Tu EY, et al. PracticePatterns and Opinions in the Treatment of AcanthamoebaKeratitis. Cornea October 2011 (Epub ahead of print).16. Visvesvara GS, Stehr-Green JK. Epidemiology offree- living ameba infections. The Journal of protozoology 1990, 37(4):25S-33S.17. Joslin, CE, Tu, EY, Stayner L, Davis F. The association between Acanthamoeba keratitis and showeringwith con- tact lenses. Paper presented at the AmericanAcademy of Optometry October 22, 2008.ding yeast forms such as Candida.6,7 Fungalcultures are the gold standard for diagnosis.8Corneal scrapings and cultures may be positive in up to 90% of initial scrapings. Mostfungi grow well in blood agar or Sabourauddextrose agar as culture media. Growth usually occurs within three or four days but cantake as long as four to six weeks.9 Gram andgiemsa stains or potassium hydroxide (KOH)wet mounts are useful for identifying fungalelements. Polymerase chain reaction (PCR) isanother diagnostic tool. Results from clinicalstudies suggest that PCR is more sensitivethan culture as a diagnostic aid in ocular fungal infections and is also much faster. Resultsare known within 24 hours. However, PCRis associated with a high false-positive rate.8 Ifthere is strong suspicion of fungus and othertests are negative, biopsy may be required.B, because of its numerous toxicities, isadministered as a second-line treatment tonatamycin. Recommended dosage is 1mg/kg/day intravenously or topically in 0.15% to0.3% solution every 30 to 60 minutes. Sideeffects can include renal toxi
REVIEW OF OPTOMETRY 3January 2012 Ernest Bowling, OD, FAAO, is in private prac-tice in Gadsden, AL, and is associate clinical . Arch Ophthalmol 2011 Oct 10. [Epub ahead of print]. ICD-9 Codes † 370.00 Corneal ulcer, unspecified † 370.01 Marginal corneal ulcer † 370.02 Ring corneal ulcer † 370.03 Central corneal ulcer † 370.04 .