Transcription
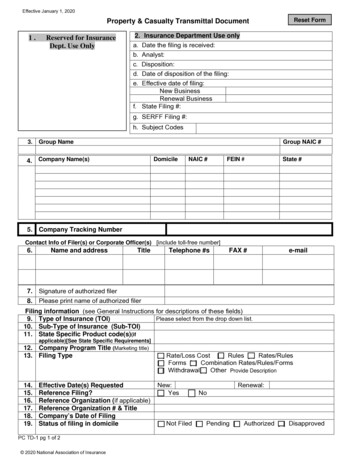
Effective January 1, 2020Reset FormProperty & Casualty Transmittal Document1.Reserved for InsuranceDept. Use Only2. Insurance Department Use onlya. Date the filing is received:b. Analyst:c. Disposition:d. Date of disposition of the filing:e. Effective date of filing:New BusinessRenewal Businessf. State Filing #:g. SERFF Filing #:h. Subject Codes3.Group NameGroup NAIC #4. Company Name(s)DomicileNAIC #FEIN #State #5. Company Tracking NumberContact Info of Filer(s) or Corporate Officer(s) [include toll-free number]6.Name and addressTitleTelephone #sFAX #e-mail7. Signature of authorized filer8. Please print name of authorized filerFiling information (see General Instructions for descriptions of these fields)Please select from the drop down list.9. Type of Insurance (TOI)10. Sub-Type of Insurance (Sub-TOI)11. State Specific Product code(s)(ifapplicable)[See State Specific Requirements]12. Company Program Title (Marketing title)13. Filing Type14.15.16.17.18.19.Effective Date(s) RequestedReference Filing?Reference Organization (if applicable)Reference Organization # & TitleCompany’s Date of FilingStatus of filing in domicilePC TD-1 pg 1 of 2 2020 National Association of Insurance[ ] Rate/Loss Cost [ ] Rules [ ] Rates/Rules[ ] Forms [ ] Combination Rates/Rules/Forms[ ] Withdrawal[ ] Other Provide DescriptionNew:[ ] Yes[ ] NoRenewal:[ ] Not Filed [ ] Pending [ ] Authorized [ ] Disapproved
Property & Casualty Transmittal Document20. This filing transmittal is part of Company Tracking #21. Filing Description [This area can be used in lieu of a cover letter or filing memorandum and is free-form text]View Complete Filing Description22.Filing Fees (Filer must provide check # and fee amount if applicable)[If a state requires you to show how you calculated your filing fees, place that calculation below]Check #:Amount:Refer to each state’s checklist for additional state specific requirements or instructions oncalculating fees.***Refer to the each state’s checklist for additional state specific requirements (i.e. # of additional copiesrequired, other state specific forms, etc.)PC TD-1 pg 2 of 2 2020 National Association of Insurance Commissioners
Effective January 1, 2020FORM FILING SCHEDULE(This form must be provided ONLY when making a filing that includes forms)(Do not refer to the body of the filing for the forms listing, unless allowed by state.)1. This filing transmittal is part of Company Tracking #2. This filing corresponds to rate/rule filing number(Company tracking number of rate/rule filing, if applicable)Form Name3. /Description/SynopsisForm #Include edition date01020304050607080910PC FFS-1 2020 National Association of Insurance CommissionersReplacementOrwithdrawn?[ ] New[ ] Replacement[ ] Withdrawn[[[[[[[[[[[[[[[[[[[[[[[[[[[] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] Withdrawn] New] Replacement] WithdrawnIf replacement,give form #it replacesPrevious statefiling number,if required by state
Effective January 1, 2020RATE/RULE FILING SCHEDULE(This form must be provided ONLY when making a filing that includes rate-related items such as Rate; Rule; Rate &Rule; Reference; Loss Cost; Loss Cost & Rule or Rate, etc.)(Do not refer to the body of the filing for the component/exhibit listing, unless allowed by state.)This filing transmittal is part of Company Tracking #This filing corresponds to form filing number(Company tracking number of form filing, if applicable)Overall Percentage Last Rate RevisionEffective Date of Last Rate RevisionFiling Method of Last FilingSERFF Tracking Number of Last FilingRate Increase%Rate DecreaseRate Neutral (0%)3. Filing Method (Prior Approval, File & Use, Flex Band, etc.)4a.Rate Change by Company (As Proposed)CompanyOverall %OverallWritten# ofWritten MaximumNameIndicated% Ratepremium policyholders premium%ChangeImpactchangeaffectedfor thisChange(where(whenfor thisfor mpanyName5a5b5c5dRate Change by Company (As Accepted) For State Use OnlyOverall %OverallWritten# ofWritten MaximumIndicated% Ratepremium policyholders premium%ChangeImpactchangeaffectedfor thisChange(whenfor thisfor thisprogramapplicable)programprogramMinimum% Change(whererequired)Minimum% Change5. Overall Rate Information (Complete for Multiple Company Filings only)COMPANY USESTATE USEOverall percentage rate indication (whenapplicable)Overall percentage rate impact for this filingEffect of Rate Filing – Written premium change forthis programEffect of Rate Filing – Number of policyholdersaffected6. Overall percentage of last rate revision7. Effective Date of last rate revisionFiling Method of Last filing8.(Prior Approval, File & Use, Flex Band, etc.)PC RRFS-1 2020 National Association of Insurance Commissioners
Effective January 1, 2020RATE/RULE FILING SCHEDULE(This form must be provided ONLY when making a filing that includes rate-related items such as Rate; Rule; Rate &Rule; Reference; Loss Cost; Loss Cost & Rule or Rate, etc.)(Do not refer to the body of the filing for the component/exhibit listing, unless allowed by state.)Rule # or Page # Submitted9. for ReviewReplacementor withdrawn?01[ ] New[ ] Replacement[ ] Withdrawn0203040506PC RRFS-1 2020 National Association of Insurance Commissioners[ ] New[ ] Replacement[ ] Withdrawn[ ] New[ ] Replacement[ ] Withdrawn[ ] New[ ] Replacement[ ] Withdrawn[ ] New[ ] Replacement[ ] Withdrawn[ ] New[ ] Replacement[ ] WithdrawnPrevious statefiling number,if required by state
This filing transmittal is part of Company Tracking # This filing corresponds to form filing number (Company tracking number of form filing, if applicable) Rate Increase Rate Decrease Rate Neutral (0%) 3. Filing Method (Prior Approval, File & Use, Flex Band, etc.) 4a. Rate Change by Company (As Proposed) Company Name .