Transcription
Neoadjuvant Treatment of BreastCancerKaren A GelmonClinical Professor Medicine, UBCMedical Oncologist, BC CancerAgency
Conflicts or Am I a PharmaceuticalCompany Slut? Advisory Boards– Roche, GSK, sanofi aventis, Genetech, Array,Lilly, Novartis, AstraZeneca, Pfizer, Research Funding– Roche, GSK, AstraZeneca
Neoadjuvant Chemotherapy Systemic therapy given prior to surgery– Operable– Locally Advanced Breast Cancer (LABC)– Medically unstable patients Cytotoxic chemotherapy Hormonal therapy– Studies of AI vs Tamoxifen Presurgical/window studies– New agents, end point of tissue analysis
What are the indications for Neoadjuvant therapy?GoalOperableInoperable Improve surgical options Deliver adequate“adjuvant” chemotherapy Provide in vivo antitumour assessment Assess surrogate biologicendpoints for response &survival
Evolution of Modern Adjuvant Chemotherapy –1975 -20091970s 1980s1990s 2000sSeminal First Step 1975– CMF p.o.Transition Era 1980 -1990– AC, FAC3rd Generation Regimens 1990 -2000– Epirubicin Combinations: CEF/FEC– Questions of Dose– Sequential taxanes: AC T– Combinations taxane: TAC– Which Taxane and Which SchedulePredictive Era 2000 – Addition of Trastuzumab– Do ER tumors benefit from chemo– Are Anthracyclines Necessary?– Who benefits from Taxanes– Other biologics – antiangiogenics etc
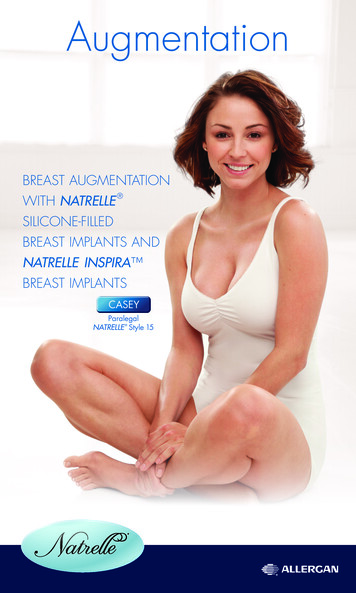
Operable Breast Cancer: NSABP B-18Operable Breast Cancer StratificationAgeClinical Tumor SizeClinical Nodal StatusOperationAC x 4 TAM if 50 yrs.AC x 4 TAM if 50 yrsNo difference in DFSand OSOperationLumpectomy Rates60% vs 68%Preop ACcCRpCR36%13%
Neoadjuvant therapy - Operable Breast Cancer Clinical response predicts overall survival Pathologic response predicts overall survivalB-18 DFS by responseB-18 OS by cPRcNRP 0.000054682P 0.0008468Wolmark N: CDC, 2000
Neoadjuvant Chemo – NON LABC Benefits– Assessment of responseto chemo– Time for consideration ofsurgical options ?BRCA etc– BCS in borderlinesituations Risks– Lack of knowledge ofaxilla unless SNLD isdone prior– Delays surgery which inmany cases may be themost important treatment– Clinical CR not usually aPathological CR– No delay in chemo– Will the patient have thesurgery?
Reminder of LABC LABC––––10 -15% of all new Breast CancersHigher incidence of HER2 , young women, PABCLABC, Inflammatory BCSometimes neglected, sometimes just aggressive Prognosis is poor––––local recurrencesystemic relapseoverall survival15 yr OS 20% IBC, 40% NIBC
Challenges/Objectives in theNeoadjuvantly treated Breast Cancer Surgical oncologyWho to send forpreoperativetherapy?Role of breastconservationRole of SLN surgerySurgery on relapse Medical oncologyWhat drugs to give forpreoperative therapy?How can we improveresponse rates?What to give onrelapse? Radiation oncologyCombined chemo-rads?Role of breastconservationRadiotherapy forinoperable/progressivedisease despite NATRadiotherapy onrelapse
Measuring Benefit from Neoadjuvanttherapy Does response predict for overallsurvival? What is clinical CR? What is pathological CR? Does it affect surgical outcomes?
B-27 Schema (n 2,411)Operable Breast CancerRandomizationAC x 4Tam X 5 YrsAC x 4Tam X 5 YrsAC x 4Tam X 5 YrsSurgeryDocetaxel x 4SurgerySurgeryDocetaxel x 4IIIIII
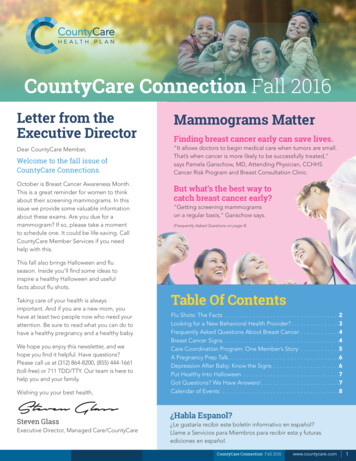
Clinical response and pathologic response are currently used as asurrogate of survival and as a tool to compare chemotherapyregimens10090% Surviving807060 TRT Non pCR pCR504001NDeaths1899 396409 31HR 0.33p 0.000123Years after Surgery45NSABP B-27: Overall Survival - pCR vs. non-pCR patients (Bear JCO 2003)
B-27Pathologic Response (pCR) in BreastNo Tumor30%Non-InvasiveP 0.00120%10%018.7%9.8%13.7%25.6%3.9%AC(1,492 pts)AC6.9%Docetaxel(718 pts)
B-27: Nodal Down-stagingRastogi P, et al. J Clin Oncol 2008;26:778-85
Breast Cancer is not ONE DiseaseBasal-likeHER-2“Normal”Luminal BLuminal ASorlie T et al, PNAS 2001
Gene expression patterns of breast carcinomasdistinguish tumour subclasses with clinicalimplicationsTherese Sørlie a,b,c, Charles M. Perou a,d, Robert Tibshirani e, Turid Aas f, Stephanie Geisler g, Hilde Johnsen b, TrevorHastie e, Michael B. Eisen h, Matt van de Rijn i, Stefanie S, Jeffrey j, Thor Thorsen k, Hanne Quist l, John C. Matese c,Patrick O. Brown m, David Botstein c, Per Eystein Lønning g, and Anne-Lise Børresen-Dale b,n
ER 65-75%All Breast CancerHER2 15-20%Basaloid 9%BRCA like 6%
What is the “standard” for Her2breast cancer in BC? Neoadjuvant– Any of our currentadjuvant protocols– Dose dense ACPaclitaxel– FEC – Doc– TAC– TC– AC– CMF– Hormones -AI LABC––––AC- DocetaxelFEC-DOCTACDose dense ACPaclitaxel– Hormones - AI
Choosing Therapy byResponsiveness not just RiskTargeted therapyUnderstanding Response PredictorsIndividualizing TherapyUnderstanding thePharmacogenomics
Case Example 66 year old woman presents with a rightbreast mass, 3.5 cm in lower inner quadranttethered to chest wall VERY anxious Treated with Letrozole 2.5 mg daily RT to breast and nodal area Mastectomy – after 4 months 1.4 cm residual disease resected Continued on letrozole with plans x 5 years
ER 65-75%All Breast CancerHER2 15-20%Basaloid 9%BRCA like 6%
Neoadjuvant Herceptin regimens exhibithigh pCR rates (16 studies, 1,226 patients)P J FEC HP J FEC HPernas et al 2007, n 33Buzdar et al 2007, n 45Lybaert et al 2006, n 25aUntch et al 2008, n 452Gianni et al 2007, n 115Untch et al 2005, n 174Coudert et al 2007, n 70Limentani et al 2007, n 31Tripathy et al 2007, n 28Antón et al 2007, n 26Marty et al 2007, n 30Harris et al 2003, n 40Hurley et al 2002, n 48Kelly et al 2006, n 37Burstein et al 2003, n 40Bines et al 2003, n 32X D HEC H J D H XJ HAP J P J CMF H (including IBC)EC J P HD HD V H (including IBC)P X HMy P HEC J D HV H (including IBC)D cisplatin H (including IBC)AC J P H (including IBC)P H (including IBC)D H0aX1020304050pCR (%)6070was given either concurrently or sequentially with D HEC, epirubicin, cyclophosphamide; FEC, 5-fluorouracil, epirubicin, cyclophosphamideMy, Myocet; X, Xeloda8090100
Neoadjuvant Trastuzumab Buzdar et alpCR ResultsP X 4 FEC x 426%Her2 operablebreast cancerP X 4 FEC x 4 concurrentTrastuzumab x 24 wksPlanned sample size 164Study closed after 42 pts accrued due to better thanexpected results62.5%
NOAH: the largest neoadjuvant trialin HER2-positive breast cancerHER2-negative LABC(IHC 0/1 )HER2-positive LABC(IHC 3 and / or FISH )n 115n 113n 99H ATq3w x 3ATq3w x 3ATq3w x 3H Tq3w x 4Tq3w x 4Tq3w x 4H q3w x 4 CMF q4w x 3CMFq4w x 3CMFq4w x 3Surgery followed byradiotherapyaSurgery followed byradiotherapyaSurgery followed byradiotherapyaH continued q3wto Week 52aHormonereceptor-positive patients receive adjuvant tamoxifen; LABC, locally advanced breast cancer; H,trastuzumab (8 mg/kg loading then 6 mg/kg); AT, doxorubicin (60 mg/m2), paclitaxel (150 mg/m2);T, paclitaxel (175 mg/m2); CMF, cyclophosphamide, methotrexate, fluorouracil
Neoadjuvant Herceptin significantlyimproves pCR rates in the NOAH trialpCR(%)908070Without HerceptinWith Herceptinp 0.0046050p 0.0024030201002343HER2 positive(n 228)17HER2negative(n 99)Total populationpCR, pathological complete response in the breastIBC, inflammatory breast cancer1955HER2 positive(n 62)29HER2negative(n 14)IBC populationBaselga et al 2007; Gianni et al 2007
Pathologic Complete Response (pCR)Untch M et al. EBCC 2008
pCR According to Tumour Stage**Predefined and stratifiedpCR, pathological complete responseUntch M et al. EBCC 2008
What is the “standard” Her2 in BC? Staging with MUGA or Echo Initiation of chemotherapy with– AC – dose dense or three weekly followed byDocetaxel /or paclitaxel and Herceptin x 4– FEC – followed by Docetaxel and Herceptin x 3– TCH – docetaxel/carbo/herceptin x 6– Herceptin continuing for a year Radiation and Surgery Hormonal therapy if ER/PR positive
Trials that are pending
NSABP B-40Her2 Neg 2cmTissue forBiomarkersRandomizeTissue forBiomarkersTx4AC x 4TX x 4AC x 4TG x 4AC x 4 Bevacizumab x 6SurgeryEndpoints: pCR; 20 endpoint: pCR Δ (29 38%)DFS N 1200 Started: 11-07 BevacIzumab
NSABP B-41Her2 PosOperab RleBCAC X 4Paclitaxel/wk TrastuzumabAC X 4Paclitaxel/wk LapatinibAC X 4Paclitaxel/wk Lapatinib TrastuzumabN 522; pCR Δ 22% (42 64%)SurgeryTmab
NEO-ALTTO (EGF106903)Invasive breast cancerHER2 T 2 cm(inflammatory BC excluded)LVEF 50%N 450Stratification:—T 5 cm versus T 5 cm—ER or PgR versus bothER and PgR –—N0-1 versus N 2—Conservative surgery or ellapatinibtrastuzumabpaclitaxel18 weekslapatinibSurgeryFEC 3trastuzumablapatinibtrastuzumab9 weeks34 weeks52 weeks of anti-ErbB2 therapy
GeparQuinto study:neoadjuvant Herceptin vs lapatinibHER2-positive primary breast cancer(IHC 3 or central FISH )n 594Epirubicin cyclophosphamide Herceptin q3w x 4Epirubicin cyclophosphamide q3w x4 lapatinib 1,250 mg qdDocetaxel q3w x 4 Herceptin q3w x 4Docetaxel q3w x 4 lapatinib 1,250 mg qdSurgeryHerceptin q3w until Week 52Docetaxel 75 mg/m2 q3w x 4; epirubicin 90 mg/m2 cyclophosphamide 600 mg/m2 q3w x 4; Herceptin8 mg/kg loading dose followed by 6 mg/kg q3w for 12 months; lapatinib 1,250 mg/day for 24 weeks
Neosphere study:neoadjuvant Herceptin pertuzumabHER2-positive LABC and large stage II breast cancer (n 400)Herceptin docetaxelq3w x 4Herceptin docetaxel pertuzumabq3w x 4Herceptin pertuzumabq3w x 4Pertuzumab docetaxelq3w x 4SurgerySurgerySurgerySurgeryFEC q3w x 3Herceptin q3wuntil Week 52FEC q3w x 3Herceptin q3wuntil Week 52Herceptin docetaxelq3w x 4FEC q3w x 3Herceptin q3wuntil Week 52FEC q3w x 3Herceptin q3wuntil Week 52
But is chemotherapy the answerto all the questions in LABC?
Our most successful therapies target selfsufficiency in growth signalsGrowth Factor Estrogen/ER HER2Therapy SERMs, AIs,oophorectomy,fulvestrant Trastuzumab– Lapatinib
How effective is Neoadjuvant Chemotherapyin ER Breast Cancer Chemotherapy is less effective in ER disease vsER- disease (but doesn’t mean some patientsdon’t benefit) Doe Luminal A benefit vs luminal B or others? Other predictive markers needed for taxanesensitivity? Other new agents?
Phase III SWOG 8814 (TBCI 0100)Postmenopausal, N , ER RANDOMIZEtamoxifen x 5 yrs(n 361)n 1477CAF x 6, with CAF x 6, thentamoxifenconcurrent tam(n 550)(n 566)Superior Disease-Free Survival(DFS) and Overall Survival (OS)over 10 YearsAlbain, et al. Breast Cancer Res Treat 2007
Disease-Free Survival by Treatment1.00No benefit toCAF over time iflow RS (n 146)Disease-free survival0.500.250.75Low risk (RS 18)Tamoxifen (n 55, 15 events)CAF-T(n 91, 26 events)0.00Strong benefitif high RSStratified log-rank p 0.97 at 10 years0246810Years since registration0.251.00Stratified log-rank p 0.033 at 10 years0246Years since registration80.750.50Stratified log-rank p 0.48 at 10 yearsTamoxifenCAF-T0.00Tamoxifen (n 47, 26 events)CAF-T(n 71, 28 events)Intermediate risk (RS 18-30)0.250.500.75Disease-free survivalHigh risk (RS 31)0.00Disease-free survival1.00Disease-Free Survival by Treatment Disease-Free Survival by Treatmen10024(n 46, 22 events)(n 57, 20 events)6Years since registration810
No DFS Benefit from CAF if Central IHC is BothHER2 Negative and ER Level High* (n 142)HER2 Positive or ER Allred 70.00Tamoxifen (n 57, 20 events)CAF-T(n 85, 30 events)0246810Stratified log-rank p 0.011 at 10 yearsTamoxifen (n 73, 36 events)CAF-T(n 112, 39 events)0.00Stratified log-rank p 0.81 at 10 yearsDisease-free survival0.750.250.501.00Disease-free survival0.250.500.751.00HER2 Negative and ER Allred 7-80Years since registration*Test for Interaction p 0.0522468Years since registration10
Surely neoadjuvant chemotherapy is the best? Semiglazov et al. PASCO 2004– neoadjuvant treatment in women aged 70 with ER breast cancer Doxorubicin and Paclitaxel (q3 weeks, 4 cycles) (n 60) 3 months treatment with anastrozole or exemestane (n 59) There was a trend towards more breast conservation in the AI arms.chemotherapy anastrozoleexemestanepathological 7.4%CRs3.3%6.8%overallclinical RRs75%81%76%
Challenges in the Management of LABCWhat are the response rates like inthe real world?ClinicalPathological
Challenges in the Management of LABCShould patients with LABC have alumpectomy if good response tochemotherapy?
Pre-Treatment MRI of BreastCancer with Septal SpreadAfter Neo-AdjuvantChemotherapyTumour shrunk to lesservolume along septa
Pathologic Response to NeoadjuvantChemotherapy (TSRCC)StudyDefinitionpCR rate (n 117) (%)NSABPpCR in breast onlyNo microinvasive diseaseCan have DCIS10.3AberdeenpCR in breast/axillaNo microinvasive diseaseCan have DCIS8.6TSRCCpCR in breast and axillaNo microinvasive diseaseCan have DCIS8.6ChevallierpCR in breast and axillaNo microinvasive iseaseNo DCIS4.3
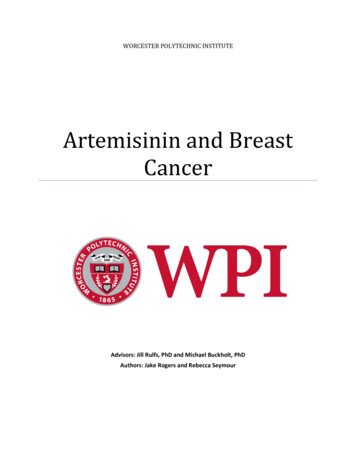
Challenges in the Management of LABCShould we treat patients with residual lymph nodeinvolvement after neoadjuvant chemotherapy withfurther adjuvant chemotherapy?
Should we treat patients with residual lymph nodeinvolvement after neoadjuvant chemotherapy with furtheradjuvant chemotherapy?100% Surviving8060 Nodal Status40 Negative 1-3 Positive 4-9 Positive 10 Positive20001NDeaths884112587 113308 107102 542345Years after SurgeryNSABP B-27: Overall Survival nodal Status; Patients without pCR 3-31-04(Bear JCO 2003)
Gepartrio PilotT 2 cmPALPATIONNCHer-2cCRRANDOMIZENX22%20%PR or CR51%TACDocetaxel 75 mg/m2Doxorubicin 50 mg/m2Cyclophosphamide 500 mg/m2pCRNXSU 3%RG TACER 7%YTAC x 628%Vinorelbine 25 mg/m2, Days 1 and 8Capecitabine 2000 mg/m2, Days 1–14G von Minckwitz ASCO Abstract #85
Systemic therapy – when more is less! LABC or neoadjuvant patients not respondingto chemotherapy––––More or different chemo is not always the answerChemo is toxicImportance of multidisciplinary teamUnique area for further study: Role of RTRole of biologicsUnderstanding chemo-resistanceResponse predictorsResponse Assessment Tools
ChallengesSurgical oncology Who to send for preoperative therapy?– In the setting of LABC – we are hoping to make surgery feasible– This is different from using NAT as the standard for ALL patients Role of breast conservation– Not common for LABC population– Can be done when feasible Role of SLN surgery– Very high rate of nodal involvement Surgery on relapse– Palliation in the setting of very poor prognosis
SummaryPreoperative vs. Postoperative– OS DFS BCSClinical and pathologic response predicts overall survivalStandard chemo is an anthracycline & taxane regimen forHER2 negative with the addition of herceptin for HER2positiveFor older HR pts consider endocrine therapyCurrently no role for more chemo for patients withresidual disease after preoperative therapy
Neoadjuvant Chemo - NON LABC Benefits - Assessment of response to chemo - Time for consideration of surgical options -?BRCA etc - BCS in borderline situations - No delay in chemo Risks - Lack of knowledge of axilla unless SNLD is done prior - Delays surgery which in many cases may be the most important treatment