Transcription
GUIDANCEREPORTELECTRONIC RECORDKEEPING GUIDANCEAND AUDIT TOOLDIGITAL RECORDKEEPING GUIDANCEFOR MIDWIVES
1GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolGUIDANCE FOR MIDWIVESRecord keeping is an essential part of midwiferypractice and maternity care. It is vital to supportsafe and effective care. All midwives shouldalready be familiar with the NMC guidance onrecord keeping within the NMC Code.1Midwives must have a clear understanding of theirresponsibilities for record keeping in line with localguidance and the NMC code of conduct. Thisincludes any entries, omissions, error correction,scribing and transcribing.The principles of good record keeping apply to alldocumentation carried out by a midwife includingpaper records, Maternity Information Systemsand Electronic Patient Record systems. The fullelectronic recording of all aspects of maternitycare is relatively new and supports the uniquemultifunction of maternity records. This multifunctionwas explored by Kirkin et al2, and includes:Partnership relationship between the womanand the midwife2. Continuity of care3. Communication between health professionals4. Improving standards of care5. Audit and clinical reviews6. Data collection7. Contribution to the research environment8. Makes midwifery work visible9. Reflection on practice and experience formidwives10. Professional expectation and demonstration ofprofessional accountability11. A narrative of experience for the womanElectronic maternity records support all thesefunctions and enhance many through their digitalfunctions such as women’s digital care records,automated processes, and data collection.Midwives must adapt their practice to make fulluse of all the digital functions within electronicmaternity records.The NMC Code doesn’t explicitly state howmidwives should keep digital recordshowever, it’sstatement on safe practice can be applied to digitalrecords like paper records to support good practice.“1.2 make sure you deliver thefundamentals of care effectively”Record keeping is a fundamental aspect ofmidwifery care. The maternity record is unique asa multidisciplinary record, carried by the womanduring her pregnancy, where she is given a newpregnancy record for each pregnancy. Informationin this record will also form the basis for thenewborn’s record when they are born.1.Digital records not only form part of the women’smedical records, but also facilitate sharing ofinformation between health professionals andwith the pregnant woman. Clear, accurate andaccessible maternity records support local safetyprocedures such as the risk governance process bymaking important aspects of maternity care easilyavailable for review. Digital maternity recordsadditionally have a secondary purpose enablingthe collection of data which is used for nationalmandatory reporting and local audits. Digitalrecords can therefore be seen as a key element ofimproving quality and safety in maternity care.1Nursing & Midwifery Council (NMC) (2018) The Code: Professional standards of practice and behaviour for nurses, midwives and nursing associates.London: Nursing & Midwifery Council.2Kerkin, B. Lennox, S. and Patterson, J. (2017) Making midwifery work visible: the multiple purposes of documentation. Women and Birth 31, 232-239.
2GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolThe NMC outlines principles of good record keeping10Keep clear and accurate records relevant to your practice. This applies to the records that arerelevant to your scope of practice. It includes but is not limited to patient records. To achieve this,you must:10.1 complete records at the time or as soon as possible after an event, recording if the notes are writtensome time after the event10.2 identify any risks or problems that have arisen and the steps taken to deal with them, so thatcolleagues who use the records have all the information they need10.3 complete records accurately and without any falsification, taking immediate and appropriateaction if you become aware that someone has not kept to these requirements10.4 attribute any entries you make in any paper or records to yourself, making sure they are clearlywritten, dated and timed, and do not include unnecessary abbreviations, jargon or speculation10.5 take all steps to make sure that records are kept securely electronicDigital records include a summary of key maternityevents, e.g. booking and birth, and will eventuallyreplace paper records entirely allowing for digitaldocumentation of all aspects of maternity care.The NMC highlights the importanceof risk in midwifery care:“8.6 share information to identifyand reduce risk”Assessing and documenting risk in an electronicrecord is essential to providing safe effectivemidwifery care. Digital tools within electronicrecords have been built to support this riskassessment process. They form an essential part ofthe risk management process to review untowardincidents and identify learning.Electronic records additionally support theappropriate sharing of a woman’s healthinformation with all healthcare providers providingher care. This easy access to all health informationallows healthcare providers to quickly risk assess awoman’s health needs and ensure they can providethe safest possible care and undertake detailedaccurate care planning. Electronic records furthersupport best practice information governance forrecord keeping ensuring that there is a clear andtransparent audit trail of who information has beenshared with.
3GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolELECTRONIC RECORD KEEPING BESTPRACTICE SUMMARYMidwives should consider the following principlesfor best practice, along side NMC Code, and localrecord keeping guidelines.To maintain these principles midwives shouldregularly undertake an audit of their owndocumentation. Maternity services should have alocalised audit tool specific to local practices andprocedures as well as the electronic system usedwithin that service.Maternity staff should, as a minimum, carry out the following checkswhen documenting: Right record/person Right place Right time (chronology) Right detail – actions and reasoning Right Login (are you logged in as yourself)Record keeping governance Midwives and MSWs must receive appropriate training for the electronic record system usedin their organisation. Each midwife or MSW is responsible for ensuring this is maintained andupdated as required when the system is updated or changed. Midwives should ensure they are up to date with their Information Governance (IG) training andare aware of how to use the electronic record to support IG Midwives and MSWs should audit their own records regularly in keeping with local guidanceand be aware of data which is collected from the electronic system to ensure they supportthis collection. Midwives should be familiar with local business continuity procedures in case of faults,cyber-attacks, or downtime
4GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolClear and organised documentation Staff are responsible for all documentation made under their login, therefore login details must notbe shared It is important that midwives and MSWs make it clear within the record when they are writing orinputting data on behalf of a colleague. The record should be checked by the midwife conductingthe care for accuracy and a note added to confirm the scribing was accurate. Student midwives should complete their own documentation and midwives should ensure theyknow the correct procedure to countersign all student entries on the system. Where an error or problem has occurred within or accessing an electronic record, the midwife orMSW accessing that record is responsible for escalating appropriately. Where unable to work ‘online’ midwives may need to update a record in an ‘offline’ setting. Itis the responsibility of the midwife to ensure the record is synced with the ‘online’ record prior tofinishing their shift/period of oncall. Midwives should be aware that digital records allow for multiple staff to be documenting andtherefore information will update in real time. Midwives should use appropriate mobile digital technology to document with the woman in herplace of care e.g. at the bedside, in her home, to maintain contemporaneous documentation andinvolve women in their care planning. Where unable to document contemporaneously midwives should ensure that they adjust theentry and assessment time of their documentation to ensure that the chronology of the record ismaintained, but clearly explain the reason for documenting retrospectivelyAccurate documentation content Tick box options should be utilised where appropriate to support data capture and for efficiency,but free text detail should be added as required for narrative e.g. actions and reasoning behinddecisions and care planning. Where a system pulls documentation into the record automatically from previously recordedinformation, it is the responsibility of the midwife to check that information is correct prior to savingthe documentation as the clinician will become responsible for everything recorded within thatsaved record.
5GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolAccurate documentation content (continued) Midwives should follow local guidance to ensure that errors made in records are corrected in atimely fashion maintaining the integrity of the record. Midwives should ensure they are aware of where other members of the multidisciplinary team aredocumenting if not within their maternity record e.g. hospital wide system. Midwives should review and update the appropriate risk assessments ensuring the current risk isclear within the record. When a staff member is unable to use the electronic record due to emergency or downtime, allpaper records should be scanned and uploaded to the electronic record for completeness. Midwives should be aware of documentation in the electronic record which will be automaticallyavailable to the woman in her digital care record. Midwives should ensure that sensitive orsafeguarding information is documented in the designated place within the electronic record to bemade available to the woman when appropriatePRINCIPLES FOR A GOODAUDIT TOOLThe maintenance of good record keepingstandards can be supported by using adocumentation audit tool.3To ensure standards are maintained for gooddocumentation4; a midwifery documentation audittool should be established within every maternityservice which allows for midwives to undertakeregular self-audits of their documentation and setsout a regular audit by peers or managers.When practice changes significantly, auditingnew practice is advised to ensure that it is wellintegrated by all midwives, expected outcomesare achieved and no adverse outcomes occur.Regular audit also supports the maintenanceof good care through continuous qualityimprovement5. When maternity services implementa new electronic record, it is important to updatethe documentation audit tool and increase thefrequency of audits to ensure standards aremaintained. Audit tools may need to be adaptedand updated as the system updates or whenconcerns are raised through the risk governanceprocess. Themes from risk governance shouldinform the local documentation audit tool used.Citation: Walker S (2012) Using self-audit to improve nurses’ record keeping. Nursing Times; 108: Online issue.3Royal College of Midwives (2016) RCM Standards for midwifery services in the UK. Royal College of Midwives.4Griffiths, P. Ddbbage, S. and Smith, A. (2013) A comprehensive audit of nursing record keeping practice. British Journal of Nursing 16(21).5
6GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolDocumentation audit tools should: Allow midwives to self evaluate their record keeping standards Be specific to electronic maternity record in your maternity service Clearly highlight minimum required documentation expected Support data collection expectations for internal and external audits and data sets Have explicit areas which identify if documentation is not of an acceptable standard Link to actions if documentation not to an acceptable standardThe use of a documentation audit tool shouldfacilitate reflection and learning from practice.Reflection on practice is an essential part ofrevalidation and is highlighted within the purposeof revalidation, “to encourage a culture of sharing,reflection and improvement”6. Therefore midwivesmay wish to use reflections on documentation auditas part of their NMC revalidation. This processallows midwives to identify areas for learning andimprovement in their individual practice.An example of a midwifery electronicdocumentation audit tool is included in theappendix and may be adapted for local usewithin your organisation.Maternity services may use documentation auditsas part of the annual appraisal process or wherethere are concerns around an individual’s practice.This standardised audit of record keeping allowsfor impartial review of the quality of midwiferydocumentation and can facilitate improvement plans.Nursing and Midwifery Council (2019) How to revalidate with the NMC: requirements for renewing your registration. London, Nursing andMidwifery Council.6
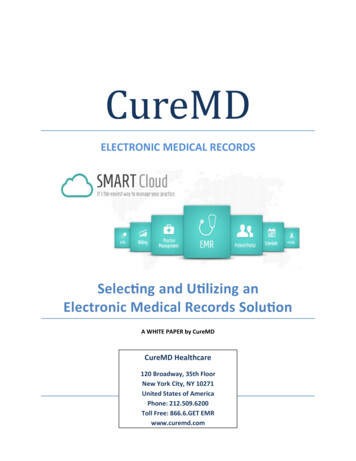
7GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolAppendix AScoring tool for documentation audit: Midwifery out-patient ante natal careUse this tool to review and audit documentation within the designated period above. Use one audit tool perrecord. Place a tick against each aspect of the documentation within one of the columns below. On the finalpage add up how many ticks appear within each column. Use this tool to reflect on the overall quality ofdocumentation and make note of any areas for improvement.Column AColumn BColumn CRisk assessment completedat Booking & detailedappropriate managementplan documented.Inaccurate Booking riskassessment. Managementplan lacking detail orinappropriate.Risk assessment not completedor lacking significant detail.No management plandocumented.Appropriate named midwife &team documented at booking.Inappropriate namedmidwife & team documentedat booking.No named midwife or teamdocumented.Management plan reviewedand updated at everyantenatal follow up withappropriate detail.Management plan reviewed& updated at most antenatalappointments. Managementplans contain appropriatedetail.Management plans notupdated or lack accuracyand detail.Assessment of anysafeguarding issuesdocumented at booking withappropriate detail. If anysocial concerns.Safeguardingdocumentation present butlacking sufficient detail.Assessment of anysafeguarding issues notdocumented at booking.EDD by scan updated followingnuchal scan appropriateupdate to management planmade if required.EDD by scan updatedbut management plan notupdated when required.Inaccurate EDD documentedor not updated from EDDby LMP.Infant feeding discussedappropriately between25-36 weeks.Some, but not all infantfeeding topics discussedbetween 25-36 weeks.No infant feeding discussionsdocumented.Only approved abbreviationsused which are recognisable.Minimal use of nonapproved abbreviations.Multiple use of non-approvedabbreviations or meaningunclear.
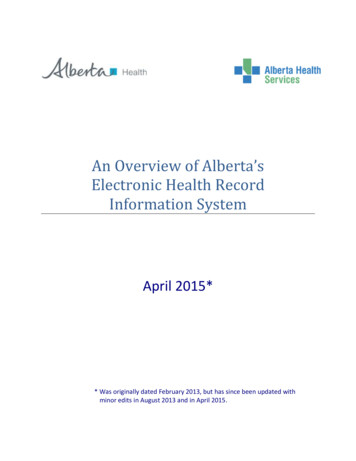
8GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolColumn AColumn BCarbon Monoxide test offeredat booking & 36 weeks. Resultsdocumented if accepted.Carbon monoxide testoffered at booking but not at36 weeks.Domestic violence screeningquestions completed atbooking, repeated at 28 &36 weeks.Column CNo documentation of carbonmonoxide testing offeredduring pregnancy.No domestic violencescreening completed duringpregnancy.VTE risk assessment completedat booking & actionedappropriately.VTE risk assessment partiallycompleted or actionsunclear.No VTE risk assessmentdocumented.Birth options discussed andany plans or preferencesclearly documented.Limited discussion of placeof birth and woman’spreferences documented forlabour and birth.No discussion aboutpreferences for place of birthor Labour and birth.Evidence of informedconsent noted throughoutdocumentation.No evidence of consentnoted throughout thedocumentation.All visits have documented: BP, SFH urinalysis Review results ofinvestigations Information shared,advice given.Minimal documentation ofcare given and further planof care.Missing documentation ofBP, SFH or urinalysis withoutexplanation.Overall, the antenatal caredocumentation demonstrates aconsistently detailed review ofpregnancy health to date, newrisks and clear action plans.Documentation occasionallyunclear or lacking detail.No evidence of a regularreview of pregnancy andhealth to date. Plan of careunclear or significantlylacking detail or regularupdates when indicated.Total:Total:Total:Mostly Column A (No Column C): Excellent!Very well doneKeep up the good workWatch out for minor errors – see below
9GUIDANCE REPORTTHE ROYAL COLLEGE OF MIDWIVESElectronic Record Keeping Guidance and Audit ToolMostly Column B (No Column C): SatisfactorySome areas for improvement required to your documentation – see belowOverall satisfactoryAny Answers in Column C: UnsatisfactorySome major areas of concernAction plan to be made with manager including regular repeat documentation auditAreas for ImprovementNamed of Midwife ReviewedName of Reviewing MidwifeDate of Review
10-18 Union StreetLondonSE1 1SZinfo@rcm.org.ukPublished: March 2021www.rcm.org.uk
GUIDANCE REPORT THE ROYAL COLLEGE OF MIDWIVES 1 Electronic Record Keeping Guidance and Audit Tool GUIDANCE FOR MIDWIVES Record keeping is an essential part of midwifery