Transcription
Feasibility, Acceptability, and PreliminaryImpact of the Cornerstone MentoringProgramAndrea Cole, PhD, MSW & Michelle Munson, PhD, MSWNew York University Silver School of Social WorkShelly Ben-David, PhD, MSWUniversity of British Columbia School of Social WorkBeth Sapiro, ABD, MSWRutgers University School of Social WorkJames Railey, ABD, MSW & Victoria Stanhope, PhD, MSWNew York University Silver School of Social Work
Funding SupportsR34-MH102525-01A1 (PI: Michelle Munson PhD, Co-I:Victoria Stanhope, Mary McKay, Steven Marcus, JamesJaccard)
Outline1. Introduce the Cornerstone Program, whichincludes youth mentoring2. Results related to acceptability, feasibility, andpracticality of the mentoring component in amental health outpatient setting3. Preliminary results on the impact of Cornerstoneintervention for transition age youth (TAY)
Background: Transition Age Youth (16 – 21) High lifetime prevalence rates of mental disorders amongTAY (Kessler et al., 2009) Even higher prevalence among system youth and formersystem youth (McMillen et al., 2005) Utilization of behavioral health care is lower among youngadults relative to children and older adults (Institute ofMedicine, 2014)
Background: Mentoring Moderate effectiveness for improving academic and mentalhealth outcomes for TAY with mental health conditions(Munson & Railey, 2017). Few mentoring programs exist in mental health settings None recruit mentors who have lived experience withmental illness and recovery.
Cornerstone ngGroup WorkIn-Vivo
What is Cornerstone Mentoring Program?MentorPeerNo LivedExperienceLived ExperienceOlder, wise, & trustedguideSame age, status orabilityMentor Training, 1:1 Match,Weekly Activities, 1-year, CloseMonitoringTraining Varies, No 1:1 Match,Variation in Dose & DurationCommunity: Non-clinical serviceClinic: “Form of mental health care”Mentorship, Role Modeling, Emotional Support,Fun and Companionship“Perhaps Mentorship”, Emotional Support,Hope, Education, AdvocacyYouth MentoringDuBois & Karcher, 2013Peer SupportDavidson et al., 2006
Recovery Role Model Mentors
MethodsData Collection Pre-intervention interviews on the manual and protocols In-person individual interviews In-person group meetings Survey responses from national leaders in the field Post-intervention interviews on implementationParticipants 67 pre-intervention multidisciplinary expert interviews 23 case summaries by mentors 10 post-intervention stakeholder interviews (TFs, RRMs, clinicaladministrators, state officials, research administrators)
MethodsMeasuresDeveloped an interview protocol on common implementation strategydomains (Powell et al., 2012)Analysis Strategy Thematic analysis utilizing constant comparison Multiple coders analyzed the data until saturation was met
Results: Acceptability of Mentoring“She responded extremely well to mentoring. She told me thatI was the first person that she trusted . I had a very strongconnection and I really care for her. I found her resiliencyinspiring.”“That’s one thing I did with the youth was tell them I’m intherapy, it’s okay, it’s really great. They really appreciated it.”“I think that the mentors are able to connect with the clientson a different level. They can share their personal experiences,and just listening to my clients . They felt like there wassomeone that they could relate to, some of their experienceswere normalized.”
Results: Acceptability of In Vivo Mentoring“You know specifically for me, I went out to one of the youthshomes when she had disappeared for quite a while and the factthat I went and found her when she went off the grid seemedvery powerful”“So I think the best thing about Cornerstone is that you arereaching children – by having the ability to go outside and doextra services and home visits God forbid, have to go to thehospital or meet with caseworkers or school workers. I thinkthe client feels the difference. I think they really feel that youcare about that them.”
Results: Feasibility of MentoringRole requirements1)2)3)4)use of mental health services as needed,Identifies as living in recovery,functioning well in terms of life domains (housing, employment)obtained a high school diploma or GED.Training Relational & engagement skillsWho trains: “I think it should be done by former mentors who have had therapy.”Boundaries (contact with mentors when clinic is closed?)Management of crises in the community
Results: PracticalityReimbursement for peer servicesUse of technology for engagement“I think one major think that worked well was having a cell phone tocommunicate with youth.”“Like texting was certainly a way to in which to access the youth”
Results: AdaptationsIntegration of mentors within the clinic and team“I think to highlight the importance of the mentor’s role where boththe caregivers and child could meet the entire team they’ll be workingwith as they represent everything as an intricate unit.”Meetings between Mentor and Transition Facilitators“Maybe there should be one on one meetings on a normal basis withthe therapist and the mentor discussing how we can work together tohelp this person.”SupervisionMore consistent and paired
Results: Outcomes for TAY (N 23)Preliminary 3-Month OutcomesAge: M 17.83Gender:Male 22% (n 5)Female 78% (n 18)Race/Ethnicity:Caucasian/White: 34% (n 8)African American/Black: 22% (n 5)Latino/Hispanic: 17% (n 4)Asian: 13% (n 3)Bi/Multiracial: 13% (n 3)
Results: Outcomes for TAY (N 23)Preliminary 3-Month OutcomesMood: 48%Anxiety: 43%Schizophrenia spectrum: 9%Medication: 52.2%Psychosis: 43% (Have you ever experienced psychosis?)Maltreatment:Physical Abuse: 21.7%Physical Neglect: 26.1%Emotional Abuse: 56.5%Sexual Abuse: 48%
Outcome MeasuresCES-D (Radloff, 1977)20-items (Range 0-60, 0 Rarely or none of the time, 5 Most or all of the time)Sample Item: I felt sad.Colorado Symptom Index (Shern et al., 1994)10-items (Range 10-60, 1 Every Day, 5 Not at all), Higher Score the fewer the symptoms)Sample Item: In the past month, how often have you heard voices, or heard or seenthings that other people didn’t think were there?Recovery Assessment Scale-Short Form (Corrigan et al., 2004)20-items (Range 20-100, 1 Strongly Disagree, 5 Strongly Agree)Sample Item: I’m hopeful about my future.Internalized Stigma11-items (Range 0-44, 0 Strongly Disagree, 4 Strongly Agree)Sample item: Teenagers my age who go to a mental health professional for theirmood and emotional difficulties are crazy
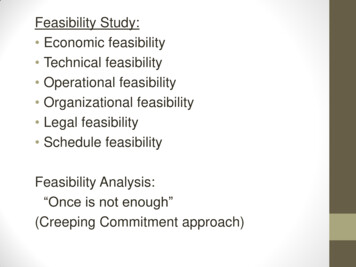
Depression302826242220Baseline3-Monthst 2.15 (df 22), p .04Time
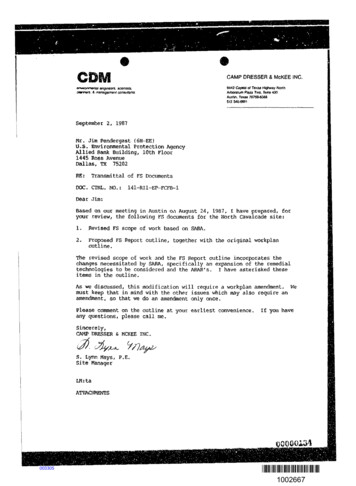
Symptoms353331292725Baseline3-Monthst 2.43 (df 22), p .02Time
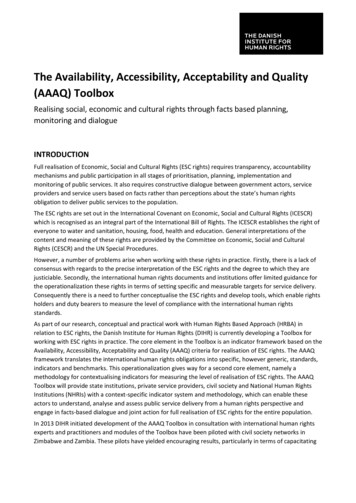
Recovery807876747270Baseline3-Monthst 1.85 (df 22), p .07Time
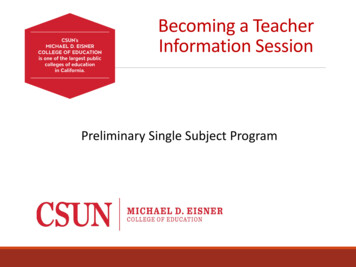
15Stigma1413121110Baseline3-MonthsTimet 1.93 (df 22), p .07
Implications for Cornerstone Mentoring in mental health outpatient programs isacceptable and feasible. There’s ways to improve the structure, supervision, training. Preliminary outcome data is trending in the direction onewould want so there’s reason to continue studying themodel.
Implications for D& I Research Data were collected as part of a Hybrid Type 2 trial,allowing for concurrent analysis of implementationand intervention data Implementation data can inform future iterationsof the intervention
Thank you!Contact Information:Michelle Munson, PhD: michelle.munson@nyu.eduAndrea Cole, PhD: arc483@nyu.edu
ReferencesDavidson, L., Chinman, M., Sells, D., & Rowe, M. (2006). Peer support among adults with seriousmental illness: a report from the field. Schizophrenia Bulletin, 32(3), 443-450.Dubois, D.L. & Karcher, M.J. (2013). Handbook of Youth Mentoring. Thousand Oaks, CA: SagePublications, Inc.Kessler, R. C., Birnbaum, H., Bromet, E., Hwang, I., Sampson, N., & Shahly, V. (2009). Age differences inmajor depression: results from the national comorbidity survey replication (NCS-R).Psychological Medicine, 40.McMillen, J.C., Zima, B.T., Scott, L.D., Auslander, W.F., & Munson, M.R. (2005). Prevalence ofpsychiatric disorders among older youths in the foster care system. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 44(1), 88-95.Munson, M.R. & Railey, J. (2016). Mentoring for Youth with Mental Health Conditions: A SystematicReview. National Mentoring Research Council.Powell, B.J., McMillen, J.C., Proctor, E.K., Carpenter, C.R., Griffey, R.T., Bunger, A.C. et al. (2012). Acompilation of strategies of implementing clinical innovations in health and mental health.Medical Care Research and Review, 69(2), 123-157.
Andrea Cole, PhD, MSW & Michelle Munson, PhD, MSW New York University Silver School of Social Work Shelly Ben-David, PhD, MSW University of British Columbia School of Social Work Beth Sapiro, ABD, MSW Rutgers University School of Social Work James Railey, ABD, MSW & Victoria Stanhope, PhD, MSW New York University Silver School of Social Work