Transcription
Financing SuicidePrevention in HealthCare SystemsBest Practices and Recommendations
This publication may be copied, reproduced, and distributed provided the copyright notice,author credit, and SPRC’s website address (sprc.org) are included. For additional rights, such asadapting or excerpting a portion of the material for publication, please submit a request on theContact Us page of www.sprc.org.Additional copies of this publication can be downloaded g-suicide-care. 2019 Education Development Center, Inc. All rights reserved.Suggested citation: Suicide Prevention Resource Center. (2019). Financing suicide prevention inhealth care systems: Best practices and recommendations. Waltham, MA: EducationDevelopment Center, Inc.ii
ContentsAcknowledgments . 2Executive Summary . 3Introduction. 5Section 1: Survey Results for Financing Suicide Prevention Care . 7Sources of Funding for Suicide Prevention Activities . 7Procedure Codes Used to Support Reimbursement . 8Obtaining and Diversifying Funding .11Care Components .12Barriers to Implementation .13Section 2: Practice Implications . 15Billing and Workflow Redesign .15Leveraging Recently Introduced Procedure Codes and Services.16Transitional Care Management Services .17Chronic Care Management Services .17General Behavioral Health Integration Services .18Collaborative Care Services .19Staff Training.19Section 3: Policy Implications . 21Certified Community Behavioral Health Clinics .21Health Homes .22Recommendations for Medicaid Changes .23Recommended State Legislation for Mental Health Services .23Conclusion . 24References . 25Appendix A - Funding Sources to Support Suicide Prevention Services . 27Appendix B - Financing Suicide Prevention in Health Care Systems . 33
AcknowledgmentsFinancing Suicide Prevention in Health Care Systems: Best Practices and Recommendationswas developed by The National Council for Behavioral Health and the Suicide PreventionResource Center (SPRC) at Education Development Center, Inc. (EDC). The National Council forBehavioral Health’s participation in producing this publication was funded by SPRC. SPRC issupported by a grant from the U.S. Department of Health and Human Services (HHS), SubstanceAbuse and Mental Health Services Administration (SAMHSA), Center for Mental Health Services(CMHS), under Grant No. 5U79SM062297.The views, opinions, and content expressed in this product do not necessarily reflect the views,opinions, or policies of CMHS, SAMHSA, or HHS.The following people contributed their time and expertise to the development of this resource:The National Council for Behavioral Health:Megan Dormon, MPHShannon Mace, JD, MPHNina Marshall, MSWRobyn Martin, PhD, MSS, MLSPOlivia Masini, MSW, LCSWFlannery Peterson, MPH, PMPAaron Surma, MSWSuicide Prevention Resource Center:Colleen Carr, MPHAdam Chu, MPHJulie Goldstein Grumet, PhDTerresa Humphries-Wadsworth, PhDVirna Little, PsyD, LCSW-r, MBA, CCM, SAPJennifer Myers, MA, LPCCarolyn O’Brien, MSW, LCSWLaurie Rosenblum, MPH2
Executive SummaryThe United States is facing a suicide epidemic that directly affects more than 44,000 individualsand families each year.1 Effective services and treatment are available to prevent suicide;however, providers face financial barriers to implementing suicide prevention services.The National Council for Behavioral Health and the Suicide Prevention Resource Center, atEducation Development Center, have collected quantitative and qualitative data from providersand subject matter experts to assess best practices, challenges, and opportunities related tofinancing suicide prevention services.2 The data informs practice and policy recommendationsfor health care systems and policymakers to improve access to effective suicide preventionservices nationwide.Findings from this data reveal that organizations delivering suicide prevention services use adiverse array of funding streams to fund individual components, leaning on different payersources (Medicaid, Medicare, commercial insurance, state and federal grants, and philanthropy,among others) to support provision of individual services. Findings also demonstrate that whileeach service component had a funding stream to support it, there were stark differences amongproviders regarding the ability to individually finance a comprehensive array of suicideprevention services, and many reported that their funders do not support reimbursement forspecific services.Together, these findings suggest opportunities at the provider and policy levels to enhanceaccess to critically necessary suicide prevention services through different financing strategies.To address the financial barriers affecting the delivery of comprehensive suicide preventionservices, providers can improve reimbursement opportunities by taking the following actions: Ensure workflows are aligned to maximize the use of existing and sometimesunderutilized procedure codesDiversify funding streamsSeek contracts with payers that specifically include suicide prevention servicesBecome actively involved in state-level decision-making on delivery systems andpayment policiesPolicymakers can increase funding for suicide prevention by taking these steps: Expand Medicaid services to include Health Homes and Certified Community BehavioralHealth ClinicsRequire managed care organizations, by way of state contracts, to ensure provision ofthe array of servicesCenters for Disease Control and Prevention, National Center for Injury Prevention and Control. (2017). Web-basedinjury statistics query and reporting system (WISQARS). Retrieved from www.cdc.gov/injury/wisqars2 These data include 161 responses to a survey conducted in 2016 with a convenience sample.13
Fund staff awareness and gatekeeper training3Fund clinical training in suicide careExpand presumptive eligibility criteria to include risk of suicideWith quality practices and a strategic approach to reimbursement for providing effective suicideprevention care, health systems and policymakers can positively impact the lives of countlessindividuals at risk for suicide.For more information on training options appropriate for clinical and non-clinical staff see the Suicide Care TrainingOptions resource available at: -training-options34
IntroductionSuicide is a preventable occurrence that affects individuals across all races and genders andhas been steadily increasing since 2000 (Stone et al., 2017). 2000–2015: The overall suicide rate increased by 28 percent, while the suicide rateamong individuals aged 34 to 64 years rose by 35 percent. Within this age group, thesuicide rate of women increased by 53 percent, and the suicide rate of men increased by29 percent (Stone et al., 2017).2003–2008: The suicide rate for veterans and other military personnel nearly doubled(Stone et al., 2017).2015: More than 44,000 individuals in the United States died by suicide, making it the10th leading cause of death. For individuals 15 to 34 years of age, suicide was thesecond leading cause of death and the third leading cause of death among youth aged10 to 14 years (Centers for Disease Control and Prevention [CDC], 2017).In addition to the immense toll that suicide has on families and communities, the burden onsociety and across health systems is also significant. The annual cost of deaths by suicide in2013, including medical costs and loss of work, was 50.8 billion, representing nearly a quarterof all costs associated with injury-related deaths (Florence et al., 2015). The mean medical andwork-loss cost per suicide was 1.2 million. In Indiana alone, the cost of suicide was estimatedto be an average of 1,184,944 per suicide death in 2010 (Goodpaster, 2015).Over the last decade, research has emerged that supports the use of programs with evidence ofeffectiveness for the prevention, identification, and treatment of suicidal behaviors (Table 1).Table 1. Examples of programs with evidence of effectivenessNameDefinitionCollaborative Assessmentand Management ofSuicidality (CAMS)CAMS is a philosophy of clinical care and a therapeutic framework in whichthe patient and provider work together to assess suicide risk and managetreatment. The Suicide Status Form (SSF) guides assessment andtreatment and is developed collaboratively between the patient andprovider throughout the course of therapy.4Cognitive Therapy forSuicide Prevention (CT-SP)CT-SP is a cognitive-behavioral psychotherapy designed to treat patientswho have thoughts of suicide or who have made a suicide attempt. CT-SPteaches patients to use alternative ways of thinking and behaving duringsuicidal crises.5Dialectical BehavioralTherapy (DBT)DBT provides clients with new skills to manage painful emotions anddecrease conflict in relationships. DBT specifically focuses on providingtherapeutic skills in four key areas: (1) mindfulness, (2) distress tolerance,(3) emotion regulation, and (4) interpersonal effectiveness.6CAMS Care. (2018). About Cams. Retrieved from https://cams-care.com/about-cams/Uniformed Services University. (2019). Cognitive therapy for suicidal patients (CT-SP). Retrieved e-Therapy-for-Suicidal-Patients-CT-SP456Behavioral Tech. (n.d.). What is dialectical behavioral therapy (DBT)? Retrieved ectical-behavior-therapy-dbt/5
Additionally, health care systems have begun to employ the Zero Suicide framework(zerosuicide.com) to address suicide care. The Zero Suicide framework is defined by a systemwide, organizational commitment to safer suicide care in health and behavioral health caresystems. Using evidence-based tools, systematic practices, training, and embedded workflows,Zero Suicide fills the gaps that patients at risk for suicide often fall through. However, despitethe effective use of this framework, gaps in funding for the array of components necessary forsafer suicide care are repeatedly cited as a barrier.To better understand these financing challenges, as well as the opportunities and best practicesavailable to the field, the National Council for Behavioral Health (National Council) and theSuicide Prevention Research Center (SPRC), at Educational Development Center (EDC),collected quantitative and qualitative data from a survey of provider organizations, keyinformant interviews, and subject matter experts (SMEs) on (1) how behavioral healthorganizations currently finance suicide prevention care activities (listed in Table 2), (2)strategies being used to improve financial support, and (3) the potential steps that providersand policymakers can take to improve the financial viability of such programs.Table 2. Care components7 included in the provider surveyFinancing Care Components1. Screening for suicide risk2. Suicide risk assessment and/or risk formulation3. Safety planning4. Lethal means counseling5. Evidence-based treatments6. Warm handoff and rapid follow-up and referrals7. Follow-up contacts8. Peer-based services9. 24-hour mobile crisis team10. Crisis contact services11. Crisis respite services7Throughout this paper, we will use the term care components when addressing suicide prevention careactivities.6
Section 1: Survey Results for FinancingSuicide Prevention CareQualitative and quantitative data were collected in 2016 via an electronic survey of 161community behavioral health organizations and key informant interviews of representativesfrom those behavioral health organizations and policy experts. Data collected included (1) thetypes of suicide prevention care services being offered by the organizations, (2) the financingmechanisms and resources utilized to support those services, and (3) the financial barriers toproviding suicide prevention care services.Sources of Funding for Suicide Prevention ActivitiesSurvey results showed that, at an aggregate level, and except for crisis respite services,providers successfully leveraged every named funding source to support every care component.See Table 3 for a list of funding sources included in the survey. Across the board, Medicaid wasthe number one source of funding for each care component.Table 3. Funding sources included in the surveyFundingSourceBrief DescriptionMedicaidA public health insurance program funded by both federal and state governmentsand administered by states. This program primarily serves low-income individualsand families and individuals with disabilities. Eligibility requirements and scope ofservices vary by state (Centers for Medicare and Medicaid Services, 2017b).MedicareA public health insurance program funded and administered by the federalgovernment. This program primarily serves older adults and individuals withdisabilities. Unlike Medicaid, Medicare benefits do not vary by state; however,some Medicare plans (Medicare Advantage) are offered through commercialinsurance, and the benefits within those plans can vary (Centers for Medicare andMedicaid Services, 2017a).Military Funding(TRICARE)Insurance for individuals who are serving or who have served in the military andtheir family members.Private orCommercialInsurancePrivate and commercial insurance plans are commonly provided to individualsthrough employer plans, through the Affordable Care Act’s Marketplace, orthrough other private insurance providers. Benefits in these plans vary by planand are subjected to state and federal regulations.State BehavioralHealth AgencyFundingFunds distributed by state agencies using local state and county funds or fundsfrom federal mental health or substance use block grants.Self-PayClients pay for the services that they receive without the assistance of public orprivate health insurance.GrantsFunds received from foundations; research organizations; and federal, state, orcounty funders.7
Procedure Codes Used to Support ReimbursementIn addition to funding sources, the survey asked respondents to identify specific procedurecodes that they used to secure reimbursement for each suicide prevention care component.Federal law requires that, with few exceptions, insurers use a common set of procedure codesto report health care services. While payers can set policies around the use of such codes (e.g.,whether to cover the service at all, reimbursement rates, eligible rendering providers, frequencyof use), definitions are supposed to hold constant for the underlying service. Procedure codesthat were included in the survey are outlined in Table 4, along with their short definitions. Inaddition, survey respondents could indicate that they paid for their service via capitatedpayments (which is generally a single payment for a combination of services), block grants, or“other.” Since many procedure codes overlap in their underlying service (e.g., 90791 for adiagnostic evaluation can include use of a screening tool, and G8431 is a code specifically fordepression screening), survey respondents could indicate the use of multiple codes for a singlecare component.Several procedure codes included in the survey were newly created in the last several years andhad varying uptake at the payer and provider levels, such as psychotherapy for crisis,transitional care management, and chronic care management services. These procedure codesare described in more detail in Section 2: Practice Implications, along with additional codes thatwere not available at the time of the survey.Table 4. Procedure codes included in the surveyCPT or HCPCSCodeDefinition90791Psychiatric diagnostic evaluation (without medical services)90792Psychiatric diagnostic evaluation (with medical services)99201-99215Office or other outpatient visit for the evaluation of a new or establishedpatient99490Chronic care management services, at least 20 minutes of clinical staff timedirected by a physician or other qualified health care professional, percalendar month8G8932Suicide risk assessed at the initial evaluationG8431Screening for depression is documented as being positive, and a follow-upplan is documentedG8510Screening for clinical depression is documented as being negative, and afollow-up plan is not required90832, 34, 37Individual psychotherapy 30, 45, and 60 minutes90839Psychotherapy for crisis, for first 60 minutes crisis code add-on for eachadditional 30 minutes8Department of Health and Human Services, Centers for Medicare and Medicaid Services. (2016).Chronic care management services. Retrieved from cCareManagement.pdf8
CPT or HCPCSCodeDefinition99495Transitional care management services with moderate medical decisioncomplexity (face-to-face within 7–14 days of discharge)999496Transitional care management services with high medical decisioncomplexity (face-to-face within 7 days of discharge)10S9484Crisis intervention mental health services, per hourS9485Crisis intervention mental health services, per diemSource: Centers for Medicare and Medicaid Services (n.d.)Table 5 shows the procedure codes reported by providers when billing for specific carecomponents, and three conclusions can be drawn from the results shown in the table.Conclusion 1: The availability of procedure codes is not a primary concern for the financing ofsuicide care prevention activities. Every care component had two or more accompanyingprocedure code(s). While both payer reimbursement policies and providers’ capacity to deliverthe underlying service impacted the ability to legitimately bill for a service, the existence (or nonexistence) of procedure codes themselves did not appear to be a primary concern.Conclusion 2: Many of the codes that providers are using for suicide prevention activities arealready in use for other behavioral health services. For instance, 90832 and other psychotherapycodes are being used to support reporting of certain evidence-based practices (EBPs). Whilethis survey does not try to answer the question of whether every EBP has an accompanyingbilling code, the survey does show that codes representing general behavioral health servicescan also support activities that are specific to suicide prevention.Conclusion 3: The survey results show that the sequencing or workflow of health care servicesmatters when it comes to successful revenue capture. Procedure codes such as 90791 and90792, which represent comprehensive psychiatric evaluations (without and with medicalservices, respectively), cannot be reported for some of the single components of suicideprevention that were named in the survey; for example, 90791 and 90792 could not be used forscreening services alone. However, when screening services are paired with an assessment,history, treatment plan, etc., then the provider can successfully capture revenue for anencounter that includes a screening. Many survey respondents indicated that their staff did notknow how to bill for services, which is essential to being able to successfully sequence servicesin a way that is both clinically effective and compliant with billing policy.Department of Health and Human Services, Centers for Medicare and Medicaid Services. (2016, December).Transitional care management services. Retrieved from 8.pdf10 Department of Health and Human Services, Centers for Medicare and Medicaid Services. (2016, December).Transitional care management services. Retrieved from 8.pdf99
x99201-99215 Office or other outpatient visit for the evaluation of a new patientxxxxx24-hour mobile crisisxxxxCrisis contactS9485 Crisis intervention mental health services, per diemxxxxxxxxCrisis respite careS9484 Crisis intervention mental health services, per hourxxx99496 Transitional care management services with high medical decision complexity(face-to-face within 7 days of discharge)xxxxxxx99495 Transitional care management services with moderate medical decisioncomplexity (face-to-face within 7 – 14 days of discharge)xx90839 Psychotherapy for crisis, for first 60 minutes crisis code add-on for eachadditional 30 minutesxG8510 Screening for clinical depression is documented as negative, follow-up plan notrequiredxxxG8431 Screening for depression is documented as being positive and a follow-up planis documentedxxEvidence-basedtreatments90832, 34, 37 Individual psychotherapy 30, 45, and 60 minutesxxxWarm handoffsG8932 Suicide risk assessed at the initial evaluationxxFollow-up contacts99490 Chronic care management services, at least 20 minutes of clinical staff timedirected by a physician or other qualified healthcare professional, per calendar monthxScreening90792 Psychiatric diagnostic evaluation (with medical services)Suicide riskassessmentxSafety planningxLethal meanscounselingxPeer-based services90791 Psychiatric diagnostic evaluation (without medical services)CPT or HCPCS CodeComponents of Suicide Prevention CareTable 5. Current Procedural Terminology (CPT) codes reported by survey respondents forspecific suicide prevention activities10
During key informant interviews, participants named several methods they used for overcomingbilling challenges. These are offered as suggestions for practitioners, clinic managers,integrated care project directors, and billing/coding staff: Understand state-based rules and regulations regarding same-day billing, scope ofpractice laws, supervised billing, etc. The SAMHSA-HRSA Center for Integrated HealthSolutions maintains state-level billing sheets that are one resource for understandingavailable procedure codes.11Establish a director of reimbursement position to oversee all billing to ensure it is doneaccurately and appropriately for all payers as well as to identify opportunities tomaximize reimbursement and ease the burden on providers.Maximize health information technology, including electronic health records (EHRs), toease the documentation and billing burden on individual providers.Understand provider credential and licensure requirements to inform hiring practices.This includes understanding reimbursement rates and treatment limitations toaccurately conduct a cost-benefit analysis.Obtaining and Diversifying FundingIn addition to utilizing procedure codes for reimbursement, organizations are using otherfunding sources to overcome barriers to financing suicide prevention services. Key informantinterviews revealed practices that some organizations have used to address limited fundingavailability: Identifying and implementing reimbursable evidence-based practices.Advocating for the inclusion of more services into insurance programs, such asMedicaid, to address long-term sustainability issues. Some organizations reportedchallenges with long-term funding sustainability given the time-limited nature of grantfunding. Through participation on state-led coalitions and workgroups, one organizationwas advocating for greater inclusion of suicide prevention services within the state’sMedicaid Waiver.Seeking grant funding that can offer flexibility for training and services, which areotherwise non-reimbursable, and allow the organization to provide a wider range ofservices to clients.Obtaining “train the trainer” funding from local, state, and federal partners to trainorganizational staff and community partners can help sustain training efforts.Negotiating a strategic number of train-the-trainer events to minimize provider timeaway from direct services to clients (which decreases revenue).Ensuring individuals with lived experience with suicide crisis (suicide loss survivors,suicide attempt survivors, and family members), and suicide prevention providers havean active voice in informing funding, policy decision-making, and state-led suicideprevention activities. For example, individuals with lived experience can share first-handThe SAMHSA-HRSA Center for Integrated Health Solutions state billing and finance sheets can be found ing-financial-worksheets.1111
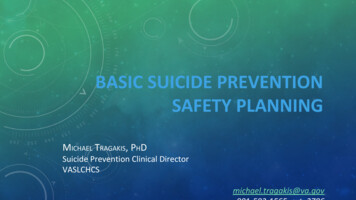
experiences with the current health care system and the need for recommendedstrategies, improvements, and supports for suicide prevention.Designating a member of the organization’s executive leadership team as a championfor suicide prevention. For example, one organization benefited from the fact that anexecutive leader was also the designated suicide prevention officer/director. This helpedto instill suicide prevention values throughout the organization as well as keep suicideprevention at the forefront of conversations regarding funding and resource allocation.Including suicide prevention-related measures and outcomes as part of the performancemeasurement in their service contracts. For example, one organization successfullyadvocated for the inclusion of suicide prevention measures within their system’sMeaningful Use program for EHR adoption.Care ComponentsFigure 1 shows the percentage of respondent organizations providing care components. At 94percent, the most common care component provided by surveyed organizations was screening.Approximately 60 percent of those that provided screening reported that they received Medicaidreimbursement, and approximately 40 percent reported that they received private or commercialinsurance reimbursement. The least common component provided is crisis respite services (25percent): 89 percent reported that they received Medicaid reimbursement, and 36 percentreported that they received private or commercial insurance reimbursement.12
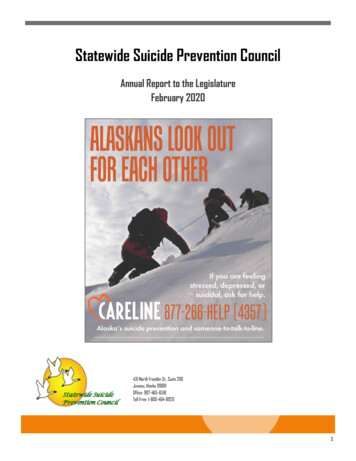
Figure 1. Percentage of respondent organizations providing care components0%20%40%100%88%Suicide Risk Assessment and/or Risk 93%Safety Planning69%Lethal Means CounselingEvidence-Based Treatments72%Warm Handoffs and Rapid Follow-Up/Referrals72%86%Follow-Up Contacts58%Peer-Based Services41%60%Crisis Contact ServicesCrisis Respite Services80%94%Screening24-Hour Mobile Crisis Team60%25%Barriers to ImplementationFinancial barriers to implementing suicide prevention services impact providers and individualsat risk of suicide in several ways, for example: If organizations do not receive funding or reimbursement for service delivery, they mustprovide services at a loss to the organization. Without sustainable funding, organizationscannot continue to offer suicide prevention support.Inadequate reimbursement rates delay access to care and result in long waiting lists forindividuals seeking care.Table 6 shows the percentage of organizations that reported very significant or moderatelysignificant barriers to implementing each of the care components. Percentages are calculatedbased on the number of organizations that responded to each question; therefore, the totalnumber of applicable respondents varies. Because organizations were permitted to select morethan one barrier for each question, the total percent for each question could exceed 100.13
Not funded by ourpayers to provide theserviceWe do not know how tobill for the serviceStaff are not trained todeliver the serviceCare ComponentStaff do not have correctlicensure/credentialingto be reimbursedTable 6. Percentage of respondent organizations reporting very significant ormoderately significant barriers to providing care afety planning5%8%8%14%Lethal means counseling7%16%10%17%Evidence-based treatments9%16%6%16%Warm handoffs/referrals9%13%16%25%Follow-up contacts8%9%19%29%Peer-based services19%15%11%30%24-hour mobile crisis team10%17%
Nina Marshall, MSW Robyn Martin, PhD, MSS, MLSP Olivia Masini, MSW, LCSW Flannery Peterson, MPH, PMP Aaron Surma, MSW . Suicide Prevention Resource Center: Colleen Carr, MPH Adam Chu, MPH Julie Goldstein Grumet, PhD Terresa Humphries-Wadsworth, PhD Virna Little, PsyD, LCSW-r, MBA, CCM, SAP Jennifer Myers, MA, LPC Carolyn O'Brien, MSW, LCSW Laurie Rosenblum, MPH . 3 . Executive Summary . The .