Transcription
12/17/2021Participating in the WebinarAll attendees will be muted andwill remain in Listen Only Mode.Type your questions here sothat the moderator can seethem. Not all questions will beanswered but we will get toas many as possible.1How to Receive CME and MOC PointsLIVE VIRTUAL GRAND ROUNDS WEBINARACG will send a link to a CME & MOC evaluation to allattendees on the live webinar.ABIM Board Certified physicians need to complete their MOC activities by December 31,2021 in order for the MOC points to count toward any MOC requirements that are due bythe end of the year. No MOC credit may be awarded after March 1, 2022 for this activity.2American College of Gastroenterology1
12/17/2021MOC QUESTIONIf you plan to claim MOC Points for thisactivity, you will be asked to: Please listspecific changes you will make in yourpractice as a result of the information youreceived from this activity.Include specific strategies or changes that you plan to implement.THESE ANSWERS WILL BE REVIEWED.3ACG Virtual Grand RoundsJoin us for upcoming Virtual Grand Rounds!Week 1, 2022Management of Pancreatic PseudocystsMohit Girotra, MDJanuary 6, 2022 at Noon EasternWeek 2, 2022Chronic Constipation: More Than Just Bowel MovementsKyle Staller, MD, MPHJanuary 13, 2022 at Noon EasternVisit gi.org/ACGVGR to Register4American College of Gastroenterology2
12/17/2021Disclosures:Speaker:Miguel D. Regueiro, MD, FACGAdvisory Boards and Consultant for AbbVie, ALFASIGMA, S.p.A., Allergan, Amgen, Bristol Meyer Squibb (BMS), Celgene,Genentech, Gilead, Janssen, Lilly, Miraca Labs, Pfizer, Prometheus, Salix, Seres, Takeda, UCB, TARGET Pharma Solutions;CME Companies: CME Outfitters, Cornerstones, GI Health Foundation (GiHF), Imedex, MJH Life Sciences, Remedy;Educational Grants: AbbVie, BMS, Celgene, Genentech, Gilead, Janssen, Pfizer, Takeda, UCB; Royalties: Wolters KluwerHealth as Author/Editor of UpToDate.Moderator:Jami Kinnucan, MDAdvisory Board: AbbVie, Janssen, Pfizer; Consultant: Hemp CW.*All of the relevant financial relationships listed for these individuals have been mitigated5Positioning IBD AdvancedTherapies: Today & TomorrowMiguel Regueiro, MD, FACG, AGAFChair, Department of Gastroenterology, Hepatology, &NutritionVice Chair, Digestive Diseases and Surgery InstituteThe Pier C. and Renee A. Borra Family Endowed Chairin Gastroenterology and HepatologyProfessor of Medicine, Lerner College of MedicineCleveland Clinic6American College of Gastroenterology3
12/17/2021The IBD Therapy Landscape: personalizing thechoice of biologic or small moleculeS1P Longest history IV and SQ options Rapid onset of action Best with IM (SONIC) Immunogenicity Joints/perianal disease Infection risk Lymphoma risk (withIM) IV then SQ Fast onset of action Efficacy in anti-TNFnaïve and failure Low immunogenicity Psoriasis Excellent safety profile Will there be higherefficacy with anti-IL23? zumab)Non‐protein‐based therapyRapid Onset of ActionApproved for MS (Ozanimod)Lymphocyte suppressionElevation of LFTs initially (rare)Firstdose heart rate decrease JAK inhibitorsAnti-IL12/23(Ustekimumab)Macularedema in non‐selective S1Ps (Tofacitinib)No first dose observation or ophthalmologic testingrequired (Ozanimod in MS)Adapted from Click B, Regueiro M. IBDj 2019 IV (soon SQ also) Little slower Better results in antiTNF-naive patients Low immunogenicity Gut-selective withexcellent safety profile Only for UC, butselective JAKi for CD Oral Rapid onset of action Non-protein-basedtherapy Joints Viral infection, e.g.Herpes Zoster Blood clots in RA (notUC) Improved safety withselective JAKi7Treating IBD: Why the Urgency?Theoretical impact of early effectivetreatment on disease progressionEarly diseaseDiagnosisLate diseaseDigestive ammatory activityaSubclinicalinflammationWindow ofopportunityInflammatory activityaDigestive damageNatural course of Crohn’s disease (and UC?)Tight control andmonitoringSubclinicalEarly diseaseinflammationDiagnosisLate diseaseaAssessedby CDAI, CDEIS, and/or CRP.CDAI, Crohn’s Disease Activity Index; CDES, Crohn’s Disease Endoscopic Index Severity; CRP, C-reactive protein.Colombel JF et al. Gastroenterology. 2017;152:351‐361.8American College of Gastroenterology4
12/17/2021When to start biologics – we need to get it right ininduction!Biologics usuallystarted hereWe want them tobe HERE, beforedamage occursPariente B, et al. Inflamm Bowel Dis. 2011;17(6):1415‐229Evolving Definitions of Remission in UCClinicalRemissionBiologicRemissionMayo score 0‐1 withno bleedingPRODiarrhea 0Bleeding 0PRO 0 Endoscopy 0‐1EndoscopicRemissionMayo endoscopysubscore of 0(normal) or 1HistologicRemissionVarious indicesRobartsGeboesPRO, patient‐reported outcomes.1. Rogler G et al. World J Gastroenterol. 2013;19(43):7552‐7560. 2. Walsh AJ et al. Nature Rev Gastroenterol Hepatol. 2016;13:567‐579.10American College of Gastroenterology5
12/17/2021Treatment Strategies for UC Are Driven ByPatient Risk of Complicated DiseaseLow riskHigh riskfor colectomyfor colectomyAge 40 yearsExtensive colitisDeep ulcersCorticosteroid dependentHistory of hospitalizationHigh CRP and ESRC difficile infectionCMV infectionLimited anatomic extentMild endoscopic diseaseDassopoulos T, Scherl, E, Schwartz R, Kosinski L, Cohen C, and Regueiro M Gastroenterology.2015;149:238-245.11Risk of Colectomy in UC Dictates (first line) TherapyAGA Clinical Pathway for Initial Treatment of UCLow colectomy risk patient1 (50%) Oral 5-ASA and/or Rectal 5-ASA and/or Oral budesonide or prednisoneand/or Rectal steroidsRemissionNo remission Maintenance with oral5-ASA and/or rectal 5-ASA Taper steroid over 60 daysaAdaptedHigh colectomy risk outpatient1 (50%) Short course of steroids with initiation of thiopurineor Anti-TNF with or without thiopurines Vedolizumab with or without immunomodulator Ustekinumab2aNo remissionRemissionMaintenance options Thiopurine and tapersteroids over 60 days Anti-TNF with or withoutthiopurine Vedolizumab with orwithout thiopurine ormethotrexateOptions Anti-TNF thiopurine Thiopurine (optimize6-TGN concentrations) Vedolizumab immunomodulator Tofacitiniba Proctocolectomyfrom AGA Clinical Pathway.15-ASA, 5-aminosalicylate; TGN, thioguanine nucleotide.1. Dassopoulos T, Scherl, E, Schwartz R, Kosinski L, Cohen C, and Regueiro M Gastroenterology. 2015;149:238-245.2. Sands BE et al. N Engl J Med. 2019;381(13):1201-1214.12American College of Gastroenterology6
12/17/2021Positioning Therapies in the Low-RiskUC PatientOral 5-ASA agents1,2Rectal 5-ASAs/corticosteroidsOral corticosteroids1,2 Mainstay of therapy in mild tomoderate UC Therapy should be optimized(dose, formulation, route andgood adherence) should beoptimized before moving toimmunosuppressants Favorable risk-benefit profile Suppositories preferred in proctitis3 Enema preferred in left-sided colitisin order to reach splenic flexure3 Combination therapy with oral 5ASA recommended in left-sided orextensive disease Rectal steroids are option as addon therapy in proctitis or left-sideddisease Rapid induction1,2 Budesonide has fewersystemic effects thanconventional steroids;consider as alternativefirst-line option forinduction Repetitive or prolongedcourses should be avoided1. Kornbluth A et al. Am J Gastroenterol. 2010;105:501‐523. 2. Hindryckx P et al. J Crohn's Colitis. 2018; 105–119. 3. Ungaro R et al. Lancet. 2017;389:1756‐177013Positioning Therapies in the High-RiskUC PatientTNF antagonists1 Rapid induction Significant maintenancebenefit, but immunogenicityand loss of response iscommonVedolizumab1,2 Slower onset of action Significant benefitin maintenance Better results in antiTNF-naïve patients LOVE trials evaluatingvedolizumab in earlyand late UCTofacitinib1-3 Rapid induction Effective in bothanti-TNF-naïve and experienced patients Infection risk may be problematic in combination therapy1 Avoid in patients atrisk for thrombosisUstekimumabIV then SQ maintenanceFast onset of actionEfficacy in anti-TNF-naïveand failure patientsExcellent safety profileLow immunogenicityGood use if concomitantpsoriasisLOVE‐UC (NCT02646657), An Open Label Phase 4 Study to Evaluate Efficacy of Early Versus Late Use of Vedolizumab in Ulcerative Colitis.Patients with early UC defined as disease duration 4 years and no other treatments than5‐ASAs and/or corticosteroids. Patients with late UC defined as active disease despite treatment with immunosuppressives (IS) and/or anti‐TNF. Patients with intolerance to IS and anti‐TNF will also be allowed in the lattergroup. Primary outcome is clinical and endoscopic remission at week 26.1. Hindryckx P et al. J Crohn's Colitis. 2018; 105–119. 2. Ungaro R et al. Lancet. 2017;389:1756‐1770. 3. Xeljanz (tofacitinib)[prescribing information]. Pfizer Inc., New York, NY:2019.14American College of Gastroenterology7
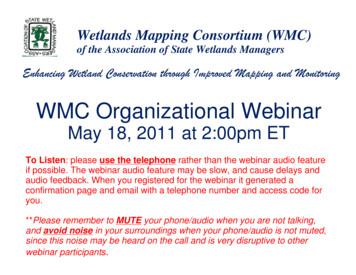
12/17/2021Systematic Review with Network Meta-Analysis:First-Line Induction Pharmacotherapy for Moderate to SevereUlcerative Colitis (caution applying systematic reviews to practice)ExperimentalStudy or subgroupEventsTotalControlEventsTotalOdds ratio(95% CI)Odds ratio(95% CI)Effect size was positivefor all treatments(compared to control)Infliximab vs placeboJiang 2015NCT01551290 ACT 1ACT 2Subtotal (95% CI)2211434141501211213339518741491211233344.12 (1.57, 10.76)2.48 (0.79, 7.77)3.15 (1.69, 5.89)8.49 (3.63, 19.88)4.22 (2.80, 6.35)2432913015090370121611130145963712.23 (1.06, 4.67)2.19 (1.14, 4.19)0.86 (0.34, 2.18)1.80 (1.18, 2.76)134571253326716692513201.99 (0.74, 5.32)3.18 (1.74, 5.79)2.81 (1.69, 4.69)30130130576764.26 (1.58, 11.52)4.26 (1.58, 11.52)56432221954179456471031.76 (0.81, 3.82)3.04 (1.03, 8.95)2.17 (1.16, 4.06)Adalimumab vs placeboULTRA 1 2011ULTRA 2 2012Suzuki 2014Subtotal (95% CI)Strongestfor vedolizumab andinfliximabGolimumab vs placeboPURSUIT Phase 2PURSUIT Phase 3Subtotal (95% CI)Vedolizumab vs placeboGEMINI 2013Subtotal (95% CI)Tofacitinib vs placeboOCTAVE 1 2016OCTAVE 2 2016Subtotal (95% CI)0.010.1Favors control110100Favors experimentalSingh S et al. Aliment Pharmacol Ther. 2018;47(2):162‐175.15Monitoring in UCStratify according to risk of relapseLow risk Remission 1 yearStable maintenance therapyEndoscopic healingHistologic healingSmoking habitGood adherence to therapyAge 50 years Clinic visit 6-12 months Calprotectin 3-6 months CRP 3-6 months (if elevated during flare) Endoscopy if symptoms or abnormal biomarkersHigh risk Flare within 1 yearRecent change in maintenance therapyPersistent endoscopic lesionsPersistent neutrophil infiltration in biopsyRecent smoking cessationLow adherence to therapyAge 50 years Clinic visit 3-4 months Calprotectin 2-3 months CRP 2-3 months (if elevated during flare) Endoscopy if symptoms or abnormal biomarkersPanes J et al. Gastroenterology. 2017;152:362-373.16American College of Gastroenterology8
12/17/2021Evolving Definitions of Remission in CDClinicalRemissionCDAI 150HBI 5PRODiarrhea 0Pain 0BiologicRemissionPRO Endoscopy andCross S score 4SES‐CD ce of ulcersCDAI, Crohn’s Disease Activity Index; CDEIS, Crohn’s Disease Endoscopic Index of Severity; HBI, Harvey-Bradshaw Index; PRO, patient-reported outcomes; SES-CD,Simple Endoscopic Score.1. Rogler G et al. World J Gastroenterol. 2013;19(43):7552-7560. 2. Walsh AJ et al. Nature Rev Gastroenterol Hepatol. 2016;13:567-579.17Treatment Strategies for CD Are Driven ByPatient Risk of Complicated DiseaseLow riskfor rapid progression 30 years old at initial diagnosisLimited anatomic involvementNo perianal and/or severe rectal diseaseSuperficial ulcersNo prior surgical resectionNo stricturing and/or penetrating patternHigh riskfor rapid progression 30 years old at initial diagnosisExtensive anatomic involvementPerianal and/or severe rectal diseaseDeep ulcersPrior surgical resectionStricturing and/or penetrating patternSandborn WJ. Gastroenterology. 2014;147:702-705.18American College of Gastroenterology9
12/17/2021Stratifying Treatment Based on Crohn’s Disease SeverityRiskAGA Clinical Pathway for Initial Treatment of Crohn’s DiseaseLow-riska patient1 ( 20%)Ileum and/or proximal colon,none to minimal symptomsOptions Budesonide 9 mg/day with orwithout AZA Tapering course of prednisonewith or without AZADiffuse or left colon,none to minimal symptomsModerate/high-riska patient1 ( 80%)Options Anti-TNF monotherapy over no therapyor thiopurine monotherapy Anti-TNF thiopurine over thiopurinemonotherapy or anti-TNF monotherapy Methotrexate for patients who do not toleratepurine analog in combination with anti-TNF Vedolizumab Ustekinumab2bOptions Tapering course of prednisonewith or without AZAAZA azathioprine.aRisk based on age at initial diagnosis ( 30 years vs 30 years); anatomic involvement (limited vs extensive); presence or absence of perianal and/or severe rectaldisease; ulcers (superficial vs deep); history of prior resection, and stricturing and/or penetrating behavior.bAdapted from AGA Clinical Pathway.11. Sandborn WJ. Gastroenterology. 2014;147:702-705. 2. Feagan BG et al. New Engl J Med. 2016. 375: 1946-1960.19Positioning Therapies in the Low-RiskCD PatientThiopurines1,2 Not effective in inducing short-termremission Effective in steroid-sparing andmaintaining steroid-induced remissionOral corticosteroids1,2 Rapid induction, used primarily as a “bridge”during disease flares to achieve symptom controluntil immunomodulators and/or biologics achievemucosal healing1 CIR-budesonide induces remission andminimizes systemic exposure, but is less effectivethan conventional oral corticosteroids1 Repetitive or prolonged courses should beavoidedCIR, controlled ileal release.1. Lichtenstein GR et al. Am J Gastroenterol. 2018;113:481‐517. 2. Sandborn WJ. Gastroenterology. 2014;147:702-705. 3. Hindryckx P et al. J Crohn's Colitis. 2018; 105–119.20American College of Gastroenterology10
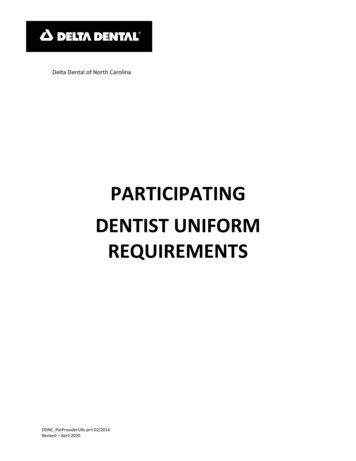
12/17/2021Positioning Therapies in the High-RiskCD PatientTNF antagonists1Ustekinumab1,2Thiopurines1,2 Option for patients whohave failedcorticosteroids,immunomodulators, oranti-TNF inhibitors Favorable safety profile Combination withanti-TNF inhibitorsrecommended, withcareful assessmentof risk-benefit inindividual patientsVedolizumab1,2 Rapid induction Significant maintenancebenefit, butimmunogenicity and lossof response is common Only biologic with provenefficacy in fistulizingdisease Option for induction,with or withoutimmunomodulator Slower onset of actionrelative to anti-TNFinhibitors Favorable safety profileobserved to date1. Lichtenstein GR et al. Am J Gastroenterol. 2018;113:481‐517. 2. Hindryckx P et al. J Crohn's Colitis. 2018; 105–119.21Systematic Review with Network Meta-Analysis:First-Line Induction Pharmacotherapy for Moderate to Severe Crohn’sDisease (caution applying systematic reviews to practice)ExperimentalStudy or subgroupEventsTotalControlEventsTotalOdds ratio(95% CI)Odds ratio(95% CI)Infliximab vs placeboLemann 2006Targan 1997Subtotal (95% CI)43125727842215824825.03 (2.25, 11.22)18.40 (2.16, 156.68)6.35 (3.04, 13.28)276761490927410843.98 (1.72, 9.22)3.00 (0.46, 19.59)3.80 (1.76, 8.18)68215215532092091.36 (0.89, 2.08)1.36 (0.89, 2.08)2116115511667678501282.27 (0.91, 5.62)3.35 (1.19, 9.47)2.68 (1.35, 5.31)80200200392002002.75 (1.76, 4.32)2.75 (1.76, 4.32)Effect size waspositive for alltreatments exceptCTZ (compared tocontrol). Strongestfor infliximab andadalimumabAdalimumab vs placeboCLASSIC I 2006Watanabe 2011Subtotal (95% CI)Certolizumab pegol vs placeboSandborn 2011Subtotal (95% CI)Vedolizumab vs placeboGEMINI II 2013GEMINI II 2014Subtotal (95% CI)Ustekinumab vs placeboUNITI‐2 2016Subtotal (95% CI)0.050.2Favors control1520Favors experimentalSingh S et al. Aliment Pharmacol Ther. 2018;48:394‐409.22American College of Gastroenterology11
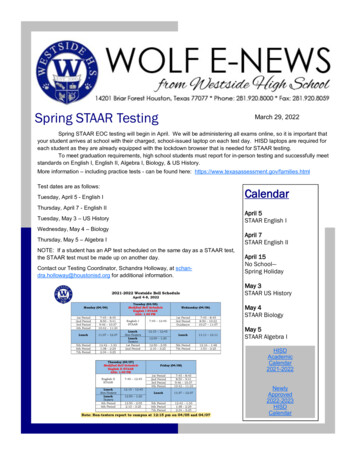
12/17/2021Systematic Review: 2nd Line Agents for Crohn’s Disease afterIFXEffect size waspositive for ADAand UST, not Vedo(compared tocontrol).Singh S et al, Aliment Pharmacol Ther 2018;48:394‐40923Monitoring in IBDLow long-term riskHigh long-term riskComplete clinical remissionBiomarker normalization at 12-16 weeksComplete clinical remissionBiomarker normalization at 12-16 weeksyesMonitor symptoms andnobiomarkers every 3-6 monthswhen alteredyesnoAfter 6 monthsEndoscopy and/orcross-sectional imagingAdapt therapy and further monitoring according to riskPanes J et al. Gastroenterology. 2017;152:362-373.24American College of Gastroenterology12
12/17/2021The Evolution of theSafety Pyramid25Safety (and Access) Influences Positioning Prevention is the best way to avoid complications: vaccinations, baseline screening,careful history, and incorporate IBD checklists in your practice If an event occurs, ask questions: is it related to IBD or the medication? e.g. antiTNF & psoriasis YES, anti-TNF & PSC in UC NO anti-TNFs: common infections greatest risk, e.g. bacterial pneumonia. Rarer but alsoassociated are opportunistic infections, e.g. fungal, mycobacterial, viral. Less commonbut associated, lymphoma JAK inhibitors (Tofa): lipid increase, viral infections (zoster), NMSC, VenousThromboembolism in RA (UC?) Anti IL12/23: although no “black box”, vigilance for infections Vedolizumab: transient LFT elevation, arthralgias, non-infectious pharyngitis, C diff? Age matters: over 60 years consider monotherapy biologic and weigh the risks/benefitsof biologicsClick B, Regueiro M. IBDj 201926American College of Gastroenterology13
12/17/2021Where will selective JAKi, anti‐IL23, and S1Pbe positioned?1. Selective JAKi, anti‐IL23, and S1Ps appear to havesimilar efficacy (without head‐to‐head data) toother biologics/small molecules to date2. Better efficacy in bio‐naïve patients3. Positioning of selective JAKi and S1P will be basedon safety (and cost, access to new meds)4. The safety of anti‐IL23 appears similar to anti‐IL12/23, and equally positioned based on safety.27Safety (and Access) Influences Positioning Prevention is the best way to avoid complications: vaccinations,baseline screening, careful history, and incorporate IBD checklists inyour practice If an event occurs, ask questions: is it related to IBD or themedication? e.g. anti-TNF & psoriasis YES, anti-TNF & PSC in UC NO anti-TNFs: common infections greatest risk, e.g. bacterial pneumonia.Rarer but also associated are opportunistic infections, e.g. fungal,mycobacterial, viral. Less common but associated, lymphoma JAK inhibitors (Tofa): lipid increase, viral infections (zoster), NMSC,Venous Thromboembolism in RA (UC?), cardiovascular risk, malignancy,less AEs with selective JAKi Anti IL12/23: although no “black box”, vigilance for infections, equalsafety with anti-IL23 Vedolizumab: transient LFT elevation, arthralgias, non-infectiouspharyngitis, C diff? S1P: increased LFTs, first dose heart rate reduction, lymphopenia,macular edema (non-selective S1Ps in uveitis, diabetes)Click B, Regueiro M. IBDj 2019.Queiroz NSF, Regueiro, M. Curr Opin Gastroenterol. 201928American College of Gastroenterology14
12/17/2021The Original Safety pyramid for IBD medsSafest(Click, Regueiro IBDj 2019)VedoUSTAnti‐TNFs monoInadequateTreatment isan AdverseEventThiopurine or TOFAThiopurine/anti‐TNFscomboSTEROIDS29The Modified Safety pyramid of current IBD medsQueiroz, Regueiro Curr Opinion Gastro 2019SafestVEDO USTAnti‐TNFsmonoInadequateTreatment isan AdverseEventThiopurine or TOFAThiopurine/anti‐TNFscomboSTEROIDS30American College of Gastroenterology15
12/17/2021SafestThe New Safety Pyramid of Today*VEDO USTInadequateTreatment isan AdverseEventAnti‐TNF TOFAThiopurineThiopurine/anti‐TNFs comboSTEROIDS*These are my opinions, notbased on head to head data31SafestThe Safety Pyramid of Tomorrow*S1P?sJAKi?VEDO USTantiIL23?Anti‐TNF TOFAInadequateTreatment isan AdverseEventThiopurineThiopurine/anti‐TNFs comboSTEROIDS*These are my opinions, notbased on head‐to‐head data32American College of Gastroenterology16
12/17/2021The Safety pyramid of Tomorrow(my opinion, no data)SafestWith more data?VEDO USTantiIL23S1P, sJAKiAnti‐TNFs TOFAInadequateTreatment isan AdverseEventThiopurineThiopurine/anti‐TNFs comboSTEROIDS33Biologics & Small Molecules for IBD “Which One Today?” – Miguel’s Practicemany insurances require anti-TNF first (FDA note: Tofa only after antiTNF) UC severe (hospitalized or “pending” hospitalization) 1st Infliximab (up to 10mg/kg) with AZA (MTX young males) 2nd Tofa (more data needed for inpt) UC: outpatient moderate (not “impending” hospitalization) 60 years or comorbid cancer/infection: 1st Vedolizumab or UST monotherapy 60 years without comorbidity: 1st Vedolizumab or UST, 2nd Tofacitinib or antiTNF/IMM CD: one segment of bowel without fistula (with fistula or extensive IFX/IMM) 60 years or comorbid cancer/infection: Vedolizumab or Ustekinumab monotherapy 60 years without comorbidity: still 1st Vedolizumab or Ustekinumab, 2nd antiTNF/IMM Loss of response to an anti‐TNF (if antiTNF was first): Secondary LOR (immunogenicity): LOR to SQ ‐ switch to IFX/UST/Tofa(UC) Vedo.LOR to IFX – switch to Tofa (UC) or UST Vedo (note: I do not switch from IV to SQ anti‐TNF) Primary LOR (no antibodies, good levels): switch out of class to Tofa(UC) or UST Vedo Extraintestinal manifestations Secondary to bowel inflammation (peripheral arthritis, iritis, EN): any that heal inflammation Pyoderma gangrenosum, Uveitis, Central Arthritis: anti‐TNF/MTX (Ustekinumab? or Tofa?) Pregnancy – any monoclonal Ab is ok, I treat straight through pregnancy: stop MTX 3mos and Tofa 1 mos prior to conception34American College of Gastroenterology17
12/17/2021Biologics & Small Molecules for IBD “Which One” – Miguel’s Practice Today and Tomorrow?many insurances require anti-TNF first. Where will sJAKi, S1Ps, anti-IL23 be placed? UC severe (hospitalized or “pending” hospitalization) 1st Infliximab (up to 10mg/kg) with AZA (MTX young males) 2nd Tofa (more data needed for inpt) selective JAKi?,probably not S1Ps at this point – more data needed UC: outpatient moderate (not “impending” hospitalization) 60 years or comorbid cancer/infection: 1st Vedolizumab or UST monotherapy, Selective JAKi, S1P, antiIL23? 60 years without comorbidity: 1st Vedolizumab or UST or sJAKi or S1P or antiIL23, 2nd Tofacitinib or antiTNF/IMM CD: one segment of bowel without fistula (with fistula or extensive IFX/IMM) 60 years or comorbid cancer/infection: Vedolizumab or Ustekinumab monotherapy or antiIL23 or sJAKi? 60 years without comorbidity: still 1st Vedolizumab or Ustekinumab, 2nd antiTNF/IMM or antiIL23 or sJAKi Loss of response to an anti‐TNF (if antiTNF was first): Secondary LOR (immunogenicity): LOR to SQ ‐ switch to IFX/UST/Tofa(UC) Vedo or . sJAKi or antiIL23 or S1P (UC)LOR to IFX – switch to Tofa (UC) or UST Vedo (note: I do not switch from IV to SQ anti‐TNF) or sJAKi or antiIL23 orS1P (UC) Primary LOR (no antibodies, good levels): switch out of class to Tofa(UC) or UST Vedo, sJAKi or or antiIL23 or S1P Pregnancy – any monoclonal Ab is ok (antiIL23?), I treat straight through pregnancy: stop MTX 3 mos and Tofa 1 mos prior to conception, Not S1P or sJAKi yet, need more date35Questions?Speaker:Miguel D. Regueiro, MD, FACGModerator:Jami Kinnucan, MD36American College of Gastroenterology18
12/17/202137American College of Gastroenterology19
How to Receive CME and MOC Points LIVE VIRTUAL GRAND ROUNDS WEBINAR ACG will send a link to a CME & MOC evaluation to all . No MOC credit may be awarded after March 1, 2022 for this activity. 1 2 . Health as Author/Editor of UpToDate. Moderator: .