Transcription
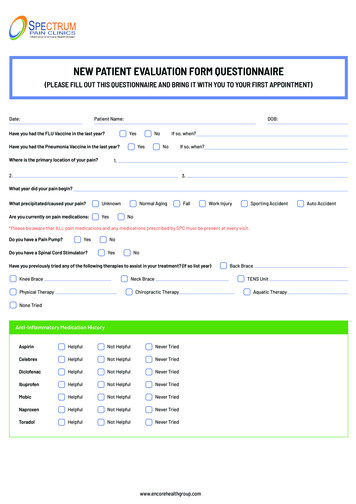
NEW PATIENT EVALUATION FORM QUESTIONNAIRE(PLEASE FILL OUT THIS QUESTIONNAIRE AND BRING IT WITH YOU TO YOUR FIRST APPOINTMENT)Date:Patient Name:Have you had the FLU Vaccine in the last year?DOB:YesHave you had the Pneumonia Vaccine in the last year?Where is the primary location of your pain?NoYesIf so, when?NoIf so, when?1.2.3.What year did your pain begin?What precipitated/caused your pain?UnknownAre you currently on pain medications:YesNormal AgingFallWork InjurySporting AccidentNo*Please be aware that ALL pain medications and any medications prescribed by SPC must be present at every visit.Do you have a Pain Pump?YesDo you have a Spinal Cord Stimulator?NoYesNoHave you previously tried any of the following therapies to assist in your treatment? (If so list year)Knee BraceNeck BracePhysical TherapyBack BraceTENS UnitChiropractic TherapyNone TriedAnti-Inflammatory Medication HistoryAspirinHelpfulNot HelpfulNever TriedCelebrexHelpfulNot HelpfulNever TriedDiclofenacHelpfulNot HelpfulNever TriedIbuprofenHelpfulNot HelpfulNever TriedMobicHelpfulNot HelpfulNever TriedNaproxenHelpfulNot HelpfulNever TriedToradolHelpfulNot HelpfulNever Triedwww.encorehealthgroup.comAquatic TherapyAuto Accident
Spectrum Pain ClinicsMuscle Relaxer Medication HistoryBaclofenHelpfulNot HelpfulNever TriedFlexerilHelpfulNot HelpfulNever TriedSomaHelpfulNot HelpfulNever TriedValiumHelpfulNot HelpfulNever TriedRobaxinHelpfulNot HelpfulNever TriedZanaflexHelpfulNot HelpfulNever TriedParafon ForteHelpfulNot HelpfulNever TriedNarcotic Medication HistoryCodeineHelpfulNot HelpfulNever TriedDuragesicHelpfulNot HelpfulNever TriedDilaudidHelpfulNot HelpfulNever TriedHydrocodoneHelpfulNot HelpfulNever TriedKadianHelpfulNot HelpfulNever TriedOpanaHelpfulNot HelpfulNever TriedBelbucaHelpfulNot HelpfulNever TriedXtampzaHelpfulNot HelpfulNever TriedOxycodoneHelpfulNot HelpfulNever TriedMorphine IRHelpfulNot HelpfulNever TriedMorphine ERHelpfulNot HelpfulNever TriedMethadoneHelpfulNot HelpfulNever TriedNucynta ERHelpfulNot HelpfulNever TriedNucyntaHelpfulNot HelpfulNever TriedButransHelpfulNot HelpfulNever TriedTramadol ERHelpfulNot HelpfulNever TriedOxycontinHelpfulNot HelpfulNever Triedwww.encorehealthgroup.com
Spectrum Pain ClinicsOther Medication HistoryCymbaltaHelpfulNot HelpfulNever TriedClonidineHelpfulNot HelpfulNever TriedAmitriptylineHelpfulNot HelpfulNever TriedKeppraHelpfulNot HelpfulNever TriedKlonopinHelpfulNot HelpfulNever TriedLidodermHelpfulNot HelpfulNever TriedNeurontinHelpfulNot HelpfulNever TriedTopamaxHelpfulNot HelpfulNever TriedZTlidoHelpfulNot HelpfulNever TriedAimovigHelpfulNot HelpfulNever TriedEmgalityHelpfulNot HelpfulNever TriedConstipation Medication HistorySennaHelpfulNot HelpfulNever TriedLactuloseHelpfulNot HelpfulNever TriedDucolaxHelpfulNot HelpfulNever TriedBiscodylHelpfulNot HelpfulNever TriedMiralaxHelpfulNot HelpfulNever TriedRelistorHelpfulNot HelpfulNever TriedMovantikHelpfulNot HelpfulNever TriedSymproicHelpfulNot HelpfulNever TriedAmitizaHelpfulNot HelpfulNever TriedPast Medical History (Please check all diseases or disorders YOU have had)MigrainesHigh Blood PressureHigh CholesterolAsthmaGallbladder orosisSpine DisorderDiabetesPlease List your Allergies:FibromyalgiaAnxietyAlcoholismArthritis OA/RACirrhosisKidney DisorderDepressionBowel DiseasePeripheral NerveAddictionNo Known Allergies NotedYesUlcersCancerStrokeSeizuresHIVIf yes, please list?www.encorehealthgroup.comCoronary ArteryHeart AttackMultiple SclerosisMuscle DisorderHead InjurySleep ApneaHiatal HerniaHeart Arrhythmia
Spectrum Pain ClinicsNoPlease List your previous surgeries: (Please include the year)YesIf yes, please list?Family History: (Please check the family members who have had the following disease/disorders)FatherFamily History of Mental DisorderGrandparentMotherFamily History of Drug abuseFamily History of Alcohol AbuseFamily History of DiabetesFamily History of HypertensionAny other notable Family History:Review of Systems: Please mark each of the following symptoms/problems that you CURRENTLY have.General:Weight LossHEENT:HeadachesRespiratory:Shortness of breathCardiology:Chest PainGastroenterology:Appetite LossGenitourinary:Painful UrinationEndocrine:Abnormal Blood SugarsVascular:Swelling in LegsMusculoskeletal:Joint PainMuscle ressionAnxietyWeight GainSinusitisFeverNight SweatsFatigueHearing LossSleep ApneaC-PapIrregular HeartbeatHigh Blood PressureChronic NauseaHeartburnBlood in UrineConstipationEnlarged ProstateEasy Bruising/BleedingNeck PainSeizuresBack PainWeakness/Numbnesswww.encorehealthgroup.com
Spectrum Pain ClinicsReview of Systems: Please mark each of the following symptoms/problems that you CURRENTLY have.Do you use MarijuanaYesWhat is your Marital Status?SingleWho resides in your home to help you?What is your Employment dDivorcedChildrenParentsSelf EmployedFriendWorks from HomeOtherWorks Part TimeWorks Full TimeWhat is your Disability Status?Short Term DisabilityLong Term DisabilityDisability Determination in processFall Risk Assessment: Are you 65 or Older?YesNo If yes, have you had any of the following occur?One Fall without injury in the past yearNo Falls in the past yearTwo or more falls with injury in the past yearwww.encorehealthgroup.comOne Fall with injury in the past yearTwo or more falls without injury in the past year
Where is the primary location of your pain? 1. 2. 3. What year did your pain begin? *Please be aware that ALL pain medications and any medications prescribed by SPC must be present at every visit. Back Brace Knee Brace Neck Brace TENS Unit Physical Therapy None Tried Chiropractic Therapy Aquatic Therapy Anti-Inflammatory Medication History