Transcription
2017Utah Medicaid & CHIPAnnual ReportState Fiscal Year 2017: July 2016 - June 2017
Utah Annual Report ofMedicaid & CHIPState Fiscal Year 2017Joseph K. Miner, MDExecutive Director, Utah Department of HealthNate Checketts, MPADeputy Director, Utah Department of HealthDirector, Division of Medicaid and Health FinancingEric Grant, MBADirector, Bureau of Financial ServicesPrepared By:Bureau of Financial ServicesDivision of Medicaid and Health FinancingUtah Department of HealthBox 143104Salt Lake City, UT 84114-3104Acknowledgments:Matt OhrenbergerDMHF Bureau Directors and StaffThis report can be viewed at: medicaid.utah.gov
Table of ContentsTable of ContentsiList of FiguresiiList of TablesiiiDirector’s MessageivDivision of Medicaid and Health Financing (DMHF)22017 Division Highlights2Organizational Chart4Division Overview5Division Expenditures6Medicaid8Medicaid FinanceMeans of Finance8Offsets to Medicaid Expenditures10Medicaid Consolidated Report of Expenditures and Revenues12Department of Health, Division of Medicaid and Health Financing16Department of Human Services17Department of Workforce Services18Office of the Attorney General19Office of Inspector General of Medicaid Services19University of Utah Medical Center20Medicaid Enrollment21Medicaid Benefits22Enrollment Statistics22Medicaid Delivery and Payment of Services34Providers34Managed Care38Utilization and Expenditures42Long term Services and Supports47Children’s Health Insurance Program (CHIP)i851Means of Finance52CHIP Enrollment54APPENDIX A: Federal Poverty Levels59APPENDIX B: Glossary61APPENDIX C: Waivers63TABLE OF CONTENTS
List of FiguresFigure 1: Division of Medicaid and Health Financing Expenditures SFY 20176Figure 2: Medicaid Expenditures SFY 20179Figure 3: Medicaid Program Total Revenue Sources SFY 201710Figure 4: Medicaid Consolidated Funds SFY 201712Figure 5: Average Member Months: All Categories22Figure 6: Average Members per Month: Adult Enrollees23Figure 7: Average Members per Month: Elderly Enrollees23Figure 8: Average Members per Month: Visually Impaired and People with Disabilities24Figure 9: Average Members per Month: Children Enrollees24Figure 10: Average Members per Month: Pregnant Women Enrollees25Figure 11: Average Members per Month: PCN Enrollees25Figure 12: Unduplicated Count of Medicaid Enrollees27Figure 13: Percent of Medicaid Enrollees by Category of Assistance SFY 201729Figure 14: Average Managed Care Enrollees per Month38Figure 15: Managed Care Expenditures39Figure 16: ACO Average Members per Month by Rate Category40Figure 17: ACO Weighted Average Base Rates41Figure 18: Unduplicated Hospital Care Claims43Figure 19: FFS Hospital Care Expenditures43Figure 20: Unduplicated Physician Services Claims44Figure 21: FFS Physician Services Expenditures44Figure 22: Unduplicated Pharmacy Services Claims45Figure 23: FFS Pharmacy Services Expenditures45Figure 24: Unduplicated Other Services Claims46Figure 25: FFS Other Services Expenditures46Figure 26: Unduplicated Long Term Services and Supports Claims47Figure 27: Long Term Services and Supports Expenditures47Figure 28: HCBS Waiver Expenditures49Figure 29: CHIP Enrollment54Figure 30: CHIP Enrollment by Federal Poverty Level SFY 201755Figure 31: Urban and Rural CHIP Enrollment Distribution56Figure 32: CHIP Enrollment by Age Range SFY 201756Figure 33: CHIP Enrollment by Race SFY 201757Figure 34: Income Limits for Medical Assistance & Medicaid Cost-Sharing Programs60LIST OF FIGURESii
List of TablesiiiTable 1: Division of Medicaid and Health Financing Expenditures SFY 2013 – SFY 20176Table 2: Federal Medicaid Assistance Percentages (FMAP) for Utah SFY 2007 – SFY 20177Table 3: Expenditures Offsets SFY 201710Table 4: Other Revenue Sources SFY 201712Table 5: Consolidated Medicaid Revenues SFY 201713Table 6: Consolidated Medicaid Expenditures SFY 201714Table 7: Utah Department of Health - Division of Medicaid and Health Financing15Table 8: Department of Human Services16Table 9: Department of Workforce Services17Table 10: Office of Attorney General18Table 11: Office of Inspector General18Table 12: University of Utah Medical Center19Table 13: Average Monthly Enrollment as a Percent of County Population25Table 14: Enrollment by Race, Age Group and Gender SFY 2013 – SFY 201726Table 15: Statewide Medicaid Enrollment Composition28Table 16: Medicaid Enrollment Composition by County29Table 17: Number of Participating Fee For Service Providers by Category of Service33Table 18: Reimbursement to Fee For Service Providers by Category of Service35Table 19: Behavioral Health Average Monthly Enrollment by County41Table 20: Nursing Home Expenditures by Locality47Table 21: HCBS Waiver Expenditures49Table 22: Long Term Services and Supports Expenditure Comparison49Table 23: CHIP Sources of Funding SFY 2013 - SFY 201751Table 24: CHIP Expenditures SFY 2013 -SFY 201752Table 25: Unduplicated CHIP Enrollment by Fiscal Year, Location, and FPL54Table 26: CHIP Enrollment by Age Range and Race56Table 27: HHS Poverty Levels58Table 28: United States vs Utah Federal Poverty Level Comparison58LIST OF TABLES
Utah Department of HealthJoseph K. Miner, M.D.Executive DirectorState of UtahGARY R. HERBERTGovernorSPENCER J. COXDivision of Medicaid and Health FinancingNate CheckettsDeputy Director, Utah Department of HealthDirector, Division of Medicaid and Health FinancingLieutenant GovernorDecember 29, 2017Dear Utahns:I am pleased to issue the 2017 Medicaid and CHIP Annual Report of the Utah Department of Health (Department).This report illustrates the Division of Medicaid and Health Financing (Division) activities for the most recent statefiscal year (July 2016 to June 2017). It provides an overview of the continual efforts by committed state employeesand stakeholders to ensure that Utah’s most vulnerable populations remain the focus of the program.During the state fiscal year (SFY) 2017, the Division worked to align its initiatives with the Department’s StrategicPlan – Healthiest People, Optimize Medicaid, and A Great Organization. The Division’s strategic plan, goals, andmetrics build on the areas of emphasis established in the Department’s plan. Ultimately, this integrated approach willhelp the Department achieve its overarching vision of Utahns enjoying the best health possible while living andthriving in healthy and safe communities.Medicaid implemented the following areas of emphasis: Healthiest People - The Division has taken several approaches to promoting health and preventing injury ordisease among Medicaid members. Many of these endeavors to improve care coordination and access to careare carried out in coordination with Medicaid Accountable Care Organizations (ACOs). Currently,approximately 90 percent of Medicaid enrollees receive services through the ACOs. Optimize Medicaid – To better meet the needs of the state and its citizens, the Division submitted an 1115waiver to the Centers for Medicare and Medicaid Services (CMS) as directed by the Legislature in House Bill437 (2016). This recently approved waiver targets vulnerable populations in the state – the chronicallyhomeless, those involved in the justice system, and others with behavioral health issues. This targetedexpansion is part of a multi-agency effort to help these individuals get the treatment they need, get back ontheir feet, and contribute to society in a meaningful way. A Great Organization – As stewards of a taxpayer funded program, the Division has refocused efforts toprovide excellent customer service by improving staff training, improving processes, and developingperformance measures to better evaluate timeliness, responsiveness and accuracy. For example, in SFY 2017,Division customer service representatives answered more than 184,033 calls from Medicaid clients andproviders. We are working on developing meaning measures for wait times and call satisfaction.I hope you will find this report to be a helpful tool in understanding the critical role that Utah Medicaid and theChildren’s Health Insurance Program (CHIP) serve in communities across the state. Through all of the initiatives, theDivision and its staff maintain focus on the needs of our members and the vital role accessible healthcare is to eachenrolled individual and family. The Department and Division look forward to the continued cooperation with theGovernor’s Office, the Utah State Legislature, the provider community, and you.Sincerely,Nate CheckettsDeputy Director, Utah Department of HealthDirector, Division of Medicaid and Health Financing288 North 1460 West Salt Lake City, UtahMailing Address: P.O. Box 143101 Salt Lake City, Utah 84114-3101Telephone (801) 538-6689 Facsimile (801) 538-6478 www.health.utah.gov
division of medicaid & health financingDivision HighlightsHealth Care ReformlSubmitted an amendment to Utah’s 1115 Demonstration Waiver on July 1, 2016 to request a targetedadult expansion for individuals from 0 to 5 percent of the federal poverty level (FPL).lSubmitted an amendment to Utah’s 1115 Demonstration Waiver that would allow individualsbetween the ages of 22 and 64 to be Medicaid eligible when residing in a residential treatmentfacility with 17 or more beds. This amendment also allows the state to pay for residential treatmentfor substance use disorders for any eligible Medicaid member in a facility with 17 or more beds.lThe State amended its original 1115 waiver submission to request additional flexibility with thetransition to a new federal administration in 2017. The amendment provisions included enrollmentlimits, a work requirement, lifetime eligibility limitations and higher non-emergent emergencyroom co-payments. The revised waiver amendments were submitted to CMS on August 15, 2017.Provider Reimbursement Information System for Medicaid (PRISM)lImplemented the third release in a multi-year project to replace the current Medicaid ManagementInformation System (MMIS). Release 3 focused on the Provider Enrollment component of PRISM,providing the ability for providers to complete enrollment and make changes online. Release 3also implemented eMIPP which supports the provider health information technology incentivesprogram. Existing provider records were converted from the legacy MMIS to PRISM to ease thetransition.lDecided to use the Michigan Cloud model for completing the MMIS replacement. The State isworking with its MMIS replacement vendor, CNSI, to adopt the State of Michigan’s claims paymentsystem for Utah Medicaid claims.New Waivers and ProgramslOpened enrollment in May 2017 for the Medically Complex Children’s Waiver (MCCW). This programserves children with disabilities and complex medical conditions by providing them access torespite services, as well as traditional Medicaid services. This third enrollment opportunity addedan additional 235 children to the program with a total of 576 children served.lCreated a Medicaid Statewide Housing Coordinator position in accordance with Senate Bill 88from the 2017 Legislative Session. The position will assist Medicaid members receiving Long TermServices and Supports to receive services in home and community-based settings rather than infacilities. The position works with housing authorities, municipalities, counties and other agenciesand stakeholders to identify existing housing options and develop new community-based settingsfor Medicaid members.Customer Service and EducationlAnswered more than 184,033 calls from Medicaid clients and providers by Medicaid customerservice representatives.lProcessed more than 5.5 million claims.lReceived 189,863 calls through AccessNow, an automated eligibility line for providers to verifywhether their patients are enrolled in Medicaid.lReceived 133,620 calls in the Health Program Representative Unit related to managed care.lProvided program and plan education to 126,218 Medicaid members, 12,273 PCN members and14,588 CHIP members.2dIVISION HIGHLIGHTS
Service Delivery and PaymentlSubmitted Access Review Monitoring Plan to CMS. Federal law requires state Medicaid programsto establish methods and procedures to ensure that Medicaid members can access services tothe same extent as the general population in the same geographic area (i.e., the “equal accessprovision”). The law requires state Medicaid programs to develop an access review monitoringplan for services not provided through managed care plans. DOH submitted this plan to CMS onSeptember 30, 2016.lSent 3,095 letters to providers who have actively billed Medicaid in the past two years as part ofthe provider enrollment re-credentialing effort. In 2011, new federal regulations required Medicaidproviders to recredential with the Medicaid agency on a regular basis. Medicaid has mailed letters,made calls, and worked with health plans to ensure providers were aware of this requirement.Medicaid continues to work with providers who did not complete the recredentialing to help themsubmit the necessary information which would allow the program to reinstate their enrollment.lEstablished lower opioid limits. The Medicaid claims processing system is now restricting firsttime opioid prescriptions to no more than a 7-day supply and is able to determine whether aMedicaid member has had a prescription for the same opioid in the past 60 days. Additionally,under new policy set by the Drug Utilization Review Board, members will be allowed a 3-monthauthorization to transition to lower opioid doses or have to obtain a prior authorization to remainon the higher doses.lAdded psychotropic drugs to the preferred drug list (PDL). In total, the PDL generated annualizedsavings of approximately 65.8 million in total funds ( 19.3 million in General Fund).lSubmitted 21 State Plan Amendments and 48 State Administrative Rules.lObtained federal approval to renew the accountable care organization (ACO) and pre-paid mentalhealth plan (PMHP) 1915(b) waivers.lBegan processing the Electronic Health Records Incentive Payments through the agency’s neweMIPP system.DIVISION HIGHLIGHTS3
Mission StatementThe mission of the Division of Medicaid and Health Financing is to provideaccess to quality, cost effective health care for eligible Utahns.Organizational ChartDivision DirectorOperations DirectorBureau ofCoverage andReimbursementPolicyAssistant DivisionDirectorBureau ofEligibility PolicyBureau ofMedicaidOperationsBureau ofManagedHealth CareBureau ofAuthorization andCommunityBased ServicesBureau entServicesPublicInformation4Assistant DivisionDirectorDIVISION ORGANIZATIONPRISMProjectAdministrativeHearings
Division OverviewThe Utah Department of Health (DOH), Division of Medicaid and Health Financing (DMHF) administersMedicaid and the Children’s Health Insurance Program (CHIP) to provide medical, dental and behavioralhealth services to needy individuals and families throughout the state. DOH is designated as Utah’sSingle State Agency for Medicaid.The administration of Medicaid and CHIP is accomplished through the Division Director’s office andsix bureaus. The Division Director administers and coordinates the program responsibilities delegatedto develop, maintain, and administer the Medicaid program in compliance with Title XIX of the SocialSecurity Act and CHIP in compliance with Title XXI of the Act, the laws of the state of Utah, and theappropriated budget. The Director’s office manages and coordinates staff training and development,legacy Medicaid Management Information System (MMIS) projects, the MMIS replacement project,SharePoint workflows, security policies and procedures, the oversight of the state’s 1115 Primary CareNetwork Demonstration Waiver, as well as Affordable Care Act (ACA) reform initiatives. In addition,each bureau has the following responsibilities:BUREAU OF FINANCIAL SERVICESThe objectives and responsibilities of this bureau include monitoring, coordinating, and facilitating theDivision’s efforts to operate economical and cost-effective medical assistance programs. The bureauis responsible for coordinating and monitoring federally mandated financial control systems, includingmonitoring of the Medicaid, CHIP, Utah’s Premium Partnership for Health Insurance (UPP), andPrimary Care Network (PCN) programs. The bureau also performs budget forecasting and preparation,development of appropriation requests and legislative presentations, monitoring of medical assistanceprograms, administration of expenditures, and federal reporting. The bureau also collects providerassessments for hospitals, nursing facilities, and ambulance service providers.BUREAU OF MANAGED HEALTH CAREThe primary responsibility of this bureau is to administer all managed care federal waivers and contractsfor both Medicaid and CHIP. In addition, the bureau is responsible for staff that provide education andassistance to Medicaid and CHIP members regarding selection of managed care plans and appropriateuse of Medicaid and CHIP benefits. This bureau also monitors the performance and quality of servicesprovided by managed care organizations on behalf of Medicaid and CHIP. Managed care includesphysical, behavioral, and dental health services. In addition, the bureau is responsible for the earlyperiodic screening, diagnosis, and treatment (EPSDT) program that provides well-child health care, theMedicaid restriction program, the School Based Skills Development program, and the Electronic HealthRecord/Health Information Technology incentive program.BUREAU OF AUTHORIZATION AND COMMUNITY-BASED SERVICESThe general responsibilities of this bureau include policy formulation, interpretation, and implementationof quality, cost-effective long term services and supports that meet the needs and preferences ofUtah’s low-income citizens. In addition, the bureau is responsible for prior authorizations of Medicaidservices not provided by managed care organizations on behalf of Medicaid members.BUREAU OF MEDICAID OPERATIONSThis bureau’s main objectives are to oversee the accurate and expeditious processing of claimssubmitted for covered services on behalf of eligible members and the training of providers regardingallowable Medicaid expenditures and billing practices. The general responsibilities include providerenrollment, processing and adjudication of medical claims, publishing all provider manuals, and beingthe single point of telephone contact for information concerning member eligibility, claims processing,and general questions about the Medicaid program.Division Overivew5
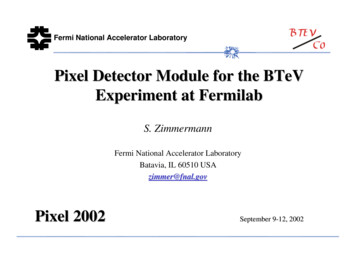
BUREAU OF COVERAGE AND REIMBURSEMENT POLICYThe general responsibilities of this bureau include benefit policy formulation, interpretation, andimplementation planning. This responsibility encompasses scope of service and reimbursement policyfor Utah’s Medicaid program. The bureau also maintains the State Plan and oversees the pharmacyprogram, which includes the Drug Utilization Review Board and the Preferred Drug List.BUREAU OF ELIGIBILITY POLICYThe primary responsibility of this bureau is to oversee eligibility determinations for Medicaid and CHIP.This includes: interpreting federal or state regulations and writing medical eligibility policy; providingtimely disability decisions based on Social Security Disability criteria; monitoring the accuracy andtimeliness of the Medicaid program by reviewing eligibility determinations under guidance from theCenters for Medicare and Medicaid Services (CMS); purchasing private health insurance plans forMedicaid members who are at high risk, which saves Medicaid program dollars; and monitoring forprogram accuracy. The bureau director also serves as the state CHIP Director.Division ExpendituresFigure 1 shows a breakdown of DMHF state fiscal year (SFY) 2017 expenditures. Medicaid mandatory,optional, and expansion services comprise 90.7 percent of total expenditures, Medicaid administrativeservices account for 4.4 percent and CHIP administration and services for 4.9 percent.Division of Medicaid and Health Financing ExpendituresSFY 2017Medicaid Optional, 985,338,300 , 35.2%Medicaid Expansion, 209,200 , 0.0%Medicaid Admin, 123,329,500 , 4.4%CHIP, 137,240,600 ,4.9%Medicaid Mandatory, 1,554,882,900 , 55.5%Figure 1Table 1 breaks down the categories in Figure 1 by expenditure types. Approximately 98 percent of theDMHF expenditures are for pass-through charges. Personnel services account for one percent of totalexpenditures. Table 1 provides a break out of these expenditures for state fiscal years (SFY) 2013 to 2017.6dIVISION EXPENDITURES
DIVISION EXPENDITURES7 2,269,946,600 72,721,800 2,450,481,100 73,725,600 199,500 0 10,400 72,829,600 684,200 1,500 400 2,376,755,500 0 0 0 0 0 0 0 0 0 0 897,518,700 0 123,000 0 12,600 897,075,700 307,400 0 0 0 1,366,362,800 86,100 4,243,800 0 15,130,800 1,339,260,400 7,592,800 33,000 15,900 0 112,874,000 0 4,586,000 0 10,374,700 81,495,400 16,357,100 21,300 39,500 0SFY 2014 2,543,770,800 103,659,600 237,300 0 5,600 102,788,100 623,200 600 4,800 2,440,111,200 0 0 0 0 0 0 0 0 0 0 927,167,600 0 234,100 0 14,000 926,542,500 377,000 0 0 0 1,396,154,000 0 4,380,200 0 8,990,300 1,375,055,600 7,666,600 36,700 24,600 0 116,789,600 0 4,719,500 0 13,106,000 81,511,000 17,378,000 15,300 59,800 0SFY 2015 2,677,081,800 128,113,800 271,000 0 8,800 127,162,000 670,800 1,200 0 2,548,968,000 0 0 0 0 0 0 0 0 0 0 956,050,200 0 186,900 0 17,600 955,096,600 742,500 5,900 700 0 1,468,789,600 0 4,148,600 0 9,006,200 1,447,759,000 7,825,900 38,100 11,800 0 124,128,200 6,700 6,459,900 1,509,600 10,647,800 87,714,600 17,738,700 21,500 29,400 0SFY 2016 2,801,000,500 137,240,600 224,400 0 5,100 136,469,400 540,100 400 1,200 2,663,759,900 209,200 0 0 0 13,700 195,500 0 0 0 0 985,338,300 0 123,200 0 19,500 983,976,200 1,207,600 11,800 0 0 1,554,882,900 0 3,000,700 0 4,252,800 1,540,747,600 6,828,200 27,300 26,300 0 123,329,500 0 5,531,500 0 11,319,100 88,087,300 18,333,900 22,800 34,900 0SFY 2017Medicaid Management Information System (MMIS) expenditures are included in the “Medicaid Mandatory” category for fiscal year2013. Prior to fiscal year 2014, MMIS expenditures were recorded in a separate line item (LKAA).TOTAL EXPENDITURESCHIP TotalCHIP 333,000 26,900 25,600 71,330,100 996,200 2,500 7,500 2,197,224,800Current ExpenseData Processing Capital ExpenditureData Processing Current ExpenseOther Charges/Pass ThroughPersonnel ServicesTravel/In StateTravel/Out of StateMedicaid Total 0 0 0 0 0 0 0 0 0 925,450,200 0 2,088,900 0 2,200 923,030,000 308,000 1,700 19,400 0 1,173,461,100 22,400 3,179,000 0 9,550,000 1,156,619,400 4,059,000 26,900 8,100( 3,700) 98,313,500 32,000 4,824,900 1,086,500 8,737,900 68,543,700 15,034,000 24,100 30,400 0SFY 2013 0Capital ExpenditureCurrent ExpenseData Processing Capital ExpenditureData Processing Current ExpenseOther Charges/Pass ThroughPersonnel ServicesTravel/In StateTravel/Out of StateTrust & Agency DisbursementsCapital ExpenditureCurrent ExpenseData Processing Capital ExpenditureData Processing Current ExpenseOther Charges/Pass ThroughPersonnel ServicesTravel/In StateTravel/Out of StateTrust & Agency DisbursementsCapital ExpenditureCurrent ExpenseData Processing Capital ExpenditureData Processing Current ExpenseOther Charges/Pass ThroughPersonnel ServicesTravel/In StateTravel/Out of StateTrust & Agency DisbursementsCapital ExpenditureCurrent ExpenseData Processing Capital ExpenditureData Processing Current ExpenseOther Charges/Pass ThroughPersonnel ServicesTravel/In StateTravel/Out of StateTrust & Agency DisbursementsExpenditure TypeTable 1: Division of Medicaid and Health Financing Expenditures SFY 2013 - SFY 2017Expansion TotalMedicaid ExpansionOptional TotalMedicaid OptionalMandatory TotalMedicaid MandatoryAdmin TotalMedicaid AdminCategory
medicaidThe Utah Department of Health (DOH), Division of Medicaid and Health Financing (DMHF) providesMedicaid funding for medical services to needy individuals and families throughout the state of Utah.Medicaid is financed by state and federal resources.Means of FinanceMedicaid was established by Title XIX of the Social Security Act in 1965. Utah implemented its Medicaidprogram in 1966 which, at the time, focused on acute and long term care. DOH is designated as theSingle State Agency responsible for making state applications to the federal government for all Medicaidfunding and Medicaid-related programs. Medicaid, a partnership program between the federal andstate governments, provides coverage for physical health, behavioral health, and dental services, aswell as long term services and supports. Eligibility for the program is based primarily on income andhousehold size. Program eligibility for aged or disabled Medicaid also considers resource levels.The Medicaid program is administered under the direction of the Centers for Medicare and MedicaidServices (CMS) within the United States Department of Health and Human Services. CMS setsrequirements that include funding, qualification, quality, and extent of medical services. CMS also hasthe responsibility to provide federal oversight of the program.Medicaid is funded by a share of both federal and state funds. This percentage of federal versus statefunding is based on the Federal Medical Assistance Percentages (FMAP), which are updated everyfederal fiscal year (FFY). The FFY runs from October 1 to September 30. The FMAP for each state rangesfrom 50 percent to 73.4 percent of program cost. The funding formula is based on each state’s latestthree year average per capita income. Table 2 is an eleven year historical list of Utah FMAP running from2007 to 2017, modified to match the state fiscal year (SFY), which runs from July 1 on one year to June30 of the following year.Table 2: Federal Medicaid Assistance Percentages (FMAP)SFY 2007– SFY 01769.98%30.02%DMHF receives approximately 65 percent of its funding from the Federal match and 35 percent fromthe State General fund, transfers, and provider assessments. During fiscal years 2009 – 2011, the federalgovernment provided a temporary increase to the FMAP as specified in the American Recovery and8Medicaid finance
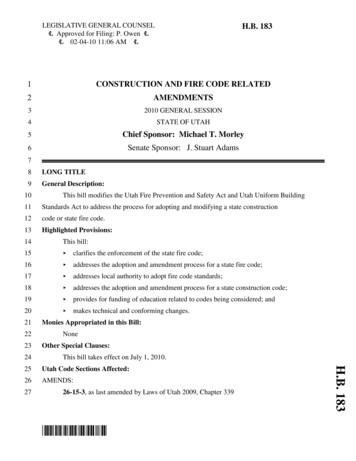
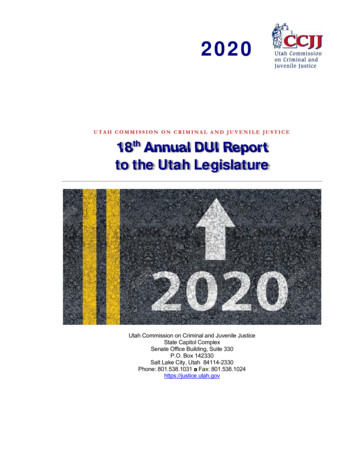
Reinvestment Act (ARRA). Those increases are not specified in Table 2. Medicaid administrative costsare generally matched at 50 percent by federal funds.Figure 2 is a breakout of Medicaid program expenditures. The largest component, “Other Charges/Pass Through,” is largely comprised of payments to providers of Medicaid services. Specifically, passthrough charges are incurred for the provision of physical health, behavioral health, dental health andhome and community-based services provided through contracted entities and administrative servicesprovided by other state agencies.Medicaid ExpendituresSFY 2017Other Charges/PassThrough, 2,613,006,500Data ProcessingCurrent Expense, 15,605,100Current Expense, 8,655,400Personnel Services, 26,369,800Travel/In State, 61,900Travel/Out of State, 61,200Figure 2DMHF’s revenues come from various fund sources, namely the State General Fund, Dedicated Credits,Restricted Revenues, Transfers and the associated Federal Funds. Transfers and most Dedicated Creditsare funds from other state agencies, local county agencies, or school districts and are often referred toas “seeded funds”, which are used to draw down federal matching funds based on the FMAP. Figure 3shows a breakout of revenue types, sources and amounts in 2017.medicaid finance9
Medicaid Program Total Revenue SourcesSFY 2017Dedicated Credits, 260,210,200 , 10%Federal Funds, 1,734,969,200 , 65%Transfers, 132,584,300 , 5%General Fund, 434,781,400 , 16%Restricted Funds, 101,214,800 , 4%Figure 3Offsets to Medicaid ExpendituresThe total cost to provide Medicaid services is decreased by the types of collections listed below.CO-PAYMENTSMedicaid members are required to pay a portion of the cost for some of the services they receive. Forexample, members pay up to 3 per prescription with a maximum of 15 per month.THIRD PARTY LIABILITYThe Office of Recovery Services (ORS) identifies commercial insurance coverage for Medicaid members. Thisinformation is used by the Division to cost avoid Medicaid expenditures. In some circumstances, federalregulations require the state to pay a claim and pursue collection from the third party insurance. ORSis responsible for coordination of benefits for fee for service (FFS) Medicaid members. ORS also pursuescollection from third parties in personal injury cases involving Medicaid members and for estate recoveryin accordance with federal regulations. Managed care organizations are responsible for coordination ofbenefits for their Medicaid members. These collections are taken into consideration in the managed carerate setting process.PHARMACY REBATESDOH negotiates supplemental rebates with manufacturers for increased offsets. In addition, the statereceives primary rebates which are negotiated by the federal government.SPENDDOWN INCOMEIf a potential Medicaid member’s income exceeds the eligibility threshold, they have the option to spenddown(or pay part of) their income in order to become eligible for Medicaid.OTHER COLLECTIONSThe Attorney General’s Office Medicaid Fraud Control Unit (MFCU) and Office of Medicaid Inspector General(OIG) are actively involved in recovering overpayments. The Division also contracts with a Recovery AuditContractor (RAC) who also identifies and recovers overpayments in order to comply with the requirementsof 42 CFR 455.10expenditure offsets
Table 3: Expenditure OffsetsSFY 2017Category Of Service and Other SourcesAmbulatory Surgical ServicesCo-Payment 500Third PartyRebatesSpenddownand OtherCollectionsTotal 306,600 0 0 307,100Attorney General/MFCU 0 0 0 54,600 54,600Autism Spectrum Disorder 0 79,300 0 0 79,300 200 35,000 0 0 35,200Chiropractic ServicesContracted Mental Health Services 0 42,600 0 0 42,600Dent
Organizational Chart 4 Division Overview 5 Division Expenditures 6 Medicaid 8 Medicaid Finance 8 . Long Term Services and Supports Expenditure Comparison 49 Table 23: CHIP Sources of Funding SFY 2013 - SFY 2017 5 1 . plan for services not provided through managed care plans. DOH submitted this plan to CMS on September 30, 2016. .