Transcription
Health Home Series:Patient-Centered MedicalHome andMeaningful UsePresenters:Christine Stroebel, MPH, PCIP/NYC REACHNatalie Fuentes, MPH, PCIP/NYC REACHAlan Silver, MD, MPH/IPROMarch 27, 2012, 2:00 – 4:30PMPrimary CareInformation Project1
Learning ObjectivesBy the end of the workshop, participants will be able to:1. Describe the difference between Patient-Centered MedicalHomes (PCMH) and Health Homes (HH) and how they arealigned.2. Identify the main areas of PCMH alignment with MeaningfulUse (MU).3. Describe Stage 1 Meaningful Use and summarize keychanges of Stage 2.4. Access resources for further information and technicalassistance.Primary CareInformation Project2
AgendaAlignment of HH, PCMH and MUPCMHMeaningful UseResourcesPrimary CareInformation Project3
PCMH and Health Homes AlignmentPatient-Centered Medical HomeA model for care that seeks to strengthen the physician-patientrelationship by replacing episodic care with coordinated care. Thephysician-led care team is responsible for coordinating all of theindividual's health care needs, and arranges for appropriate care withother qualified physicians and support services.Health HomeA model of service delivery expands on the PCMH model to buildlinkages to other community and social supports, and to enhancecoordination of medical and behavioral health care, with the mainfocus on the needs of persons with multiple chronic illnesses orsignificant behavioral conditions.Primary CareInformation Project4
PCMH and Health Homes AlignmentHealth Homes and PCMHRequire health information technology to coordinate patient caree.g., patient portal, provider-to-provider portal, RHIOHealth Homes:1. attest to participation in a RHIO/Qualified Entity,2. exchange of interoperable clinical information, certifiedEHRs,3. clinical decision support, and4. follow statewide policy guidance for interoperable HIE by 18months of program initiation.Primary CareInformation Project5
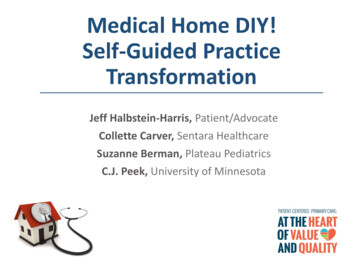
PCMH and Health Homes AlignmentHealth Homes(6 core services)Comprehensive caremanagementPCMH 2011 StandardsMeaningful Use/HIT - selected examplesStandard 1Enhance Access/ContinuityStandard 2Identify and manage patient populationsStandard 3Plan and manage careStandard 6Measure and improve performanceSearchable electronic systemStandard 4Provide self-care and community resourcesStandard 5Track and coordinate careStandard 6Measure and improve performanceProvider-to-provider portalStandard 5Track and coordinate careStandard 6Measure and improve performanceTransition of care summaryPatient and family supportStandard 4Provide self-care and community resourcesStandard 6Measure and improve performanceProvide patients with access to their health informationReferral to community andsocial support servicesStandard 4Provide self-care and community resourcesUsing EHR technology for patient-specific resourcesUse of HIT to link servicesStandards 1 – 6P2P; RHIO; Using EHR technology for patient-specificresourcesCare coordination andhealth promotionTransitional care, includingfollow-up carePrimary CareInformation ProjectCPOE; ePrescribingClinical decision support systems; Active medication list;medication allergy list; up-to-date problem listRHIOElectronic system for patient reminders for preventive orfollow up careMedication reconciliation between care settingsRHIO6
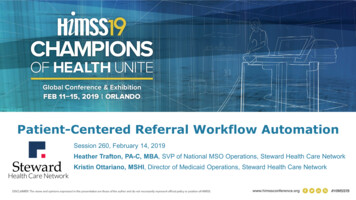
Meaningful Use &NCQA PCMH 2011Core SetMenu SetMeaningfulUse Objectives15 core objectives5 of 10menu set objectivesClinicalQuality Metrics3 core metrics, or3 alternate core metrics3 of 38menu set metrics All fifteen core objectives map to NCQA PCMH 2011 scoring All ten menu objectives map to NCQA PCMH 2011 scoring Depending upon a practice’s choice of NCQA clinicalconditions, preventive & chronic services- many of the MUquality metrics will fulfill NCQA PCMH 2011 requirements7Primary CareInformation Project7
AgendaAlignment of HH, PCMH, and MUPatient-Centered Medical HomeMeaningful UseResourcesPrimary CareInformation Project8
Patient Centered Medical HomePatient Centered NATION OF CARE“There is a clear consensus that primary care needs to be at the center of a reformed US health caresystem. The Patient-centered Medical Home (PCMH) has emerged as the key strategy for the redesign ofprimary care. The PCMH model builds upon the core concepts of primary care that include accessible,accountable, coordinated, comprehensive, and continuous care in a healing physician-patient relationshipover time. Added to these basic primary care concepts are features that improve quality of care, improvepatient centeredness, organize care across teams, and reform the payment system to support thisenhanced model of primary care.” 2010 Annals of Family Medicine, Inc.Primary CareInformation Project9doi: 10.1370/afm.10879
What is the Patient-Centered Medical Home (PCMH)?First described by American Academyof Pediatrics in 1967 in the context ofcoordinating care for children withspecial needsA medical home is a health caredelivery system that: Encourages patients to be activeparticipants in their own health andwell-being Is overseen by a personal physicianwho leads a medical team thatcoordinates all aspects of thepatient’s preventive-, acute-, andchronic-care needsPrimary CareInformation ProjectJoint Principles*Key Elements of a Medical Home Personal clinician Clinician-directed medical practice Whole-person orientation Care is coordinated & integrated Quality & safety are hallmarks Enhanced access Payment reform*Adopted March 2007 by American Academy ofFamily Practice (AAFP), American College ofPhysicians (ACP), American Academy of Pediatrics(AAP), and American Osteopathic Association (AOA)10
PCMH 2011 Goals1.Increase patient-centeredness2.Align the requirements with processes that improvequality and eliminate waste3.Increase the emphasis on patient feedback4.Enhance the use of clinical performance measureresults5.Integrate behaviors affecting health, mental health andsubstance abuse6.Enhance coordination of carePrimary CareInformation Project11
Variations on Description and Measurement*Assessment entitiesinclude:AAAHCAAFPCMSJoint CommissionNCQAURACVarious state departmentsof health Other NCQA is the mostrelevant to New York Focus mainly on structure(policies, procedures,technical capability) andprocess Tell us what you do, showus how you do it Clinical focus on three selfselected conditions &practice-defined group ofhigh-risk patients*Burton, RA, Devers KJ, Berensen RA, Patient-Centered Medical HomeRecognition Tools: A Comparison of Ten Surveys’ Content & OperationalDetails. Urban Institute, May 2011Primary CareInformation Project12
NCQA PCMH 2011 StructureAchievement levelsLevel 1: 35-59 points; Must-pass elements 6 of 6, with performance of at least 50%Level 2: 60-84 points; Must-pass elements 6 of 6, with performance of at least 50%Level 3: 85-100; Must-pass elements 6 of 6, with performance of at least 50%IT requirementsSteps for evaluation Basic: Requires electronic practice managementIntermediate: Requires EHR or e-prescribingAdvanced: Requires interoperable IT capabilities1.Practice conducts self-scoring assessment2.Practice completes on-line Survey Tool3.NCQA evaluates all data and documents & provides score4.At least 5% of practices receive additional, onsite audit by NCQA5.NCQA provides final information to the practice6.NCQA reports information on the practice, the providers and level of performance to NCQA & data users(health plans & physician directories) for practices that pass a levelPricing charged byNCQAInitial fee Survey Tool license - 80Initial Application fee Primary CareInformation Project 450- 2700 for 1-6 non-sponsored provider 360- 2700 for 1-6 sponsored providers13
Standard 1:Enhance Access and ContinuityIntent of StandardCorresponding Meaningful Use Measures Access during Office Hours (must pass)Core 12: Electronic Copy of Health Information Requires availability of advice afterCore 13: Clinical Visit Summaryhours*Menu 5: Timely Electronic Access to Health Electronic access to health information Culturally and Linguistically AppropriateInformationServices Team-based care; trained staffPrimary CareInformation Project14
Standard 2:Identify and Manage Patient PopulationsIntent of StandardCorresponding Meaningful Use Measures Practice has searchable electronic system:Electronic systems have searchablefields for demographic and clinicaldata; (not chart review) Patients receive comprehensive healthassessments Use data for population management(must pass) Identify patients who needservicesPrimary CareInformation ProjectCore 4:Core 5:Core 6:Core 7:Core 8:Core 9:Menu 3:Race/ethnicity/preferred languageMaintain up to date problem listActive medication listActive medication allergy listRecord vital signsRecord Smoking StatusGenerate lists of patients by specificconditionMenu 4: Send reminders for preventive/follow-upcare15
Standard 3:Plan and Manage CareIntent of StandardPracticeimplements evidence-based Correspondingguidelines Meaningful Use Measures Practice implements evidence-basedguidelines High-risk patients identified Care team performs care managementthrough pre-visit planning, developingplan and treatment goalsPrimary CareInformation ProjectCore 1: CPOECore 2: drug-drug, drug-allergy interactionchecksCore 3: eRxCore 6: Maintain active medication listCore 10: Use clinical decision supportMenu 1: Drug formulary checksMenu 7: Perform medication reconciliationbetween care settings16
Standard 4:Provide Self-Care Support and Community ResourcesIntent of StandardCorresponding Meaningful Use Measures Develop and document self-managementplans/goalsMenu 6: Use EHR to identify patient-specificeducation resources Provide self-care tools and support topatients Practice identifies and refers patients tocommunity resourcesPrimary CareInformation Project17
Standard 5:Track and Coordinate CareOverview of 2011 Standards Track, flag and follow up on labs andimaging results Track and follow-up on referrals Coordinate care received at hospitalsand other facilities/care transitionsMeaningful Use MeasuresCore 14: Capability to exchange key clinicalinformationMenu 2: Incorporate clinical lab test results intoEHR as structured dataMenu 7: Medication reconciliation performedfor patients coming from other caresettings or providerMenu 8: Provide summary of care record forpatients referred or transitioned toanother provider or settingPrimary CareInformation Project18
Standard 6:Measure and Improve PerformanceIntent of StandardCorresponding Meaningful Use Measures Core 11: Report clinical quality measures to CMS Measure preventive, chronic, andacute care; utilization affecting costs;patient experience and reportperformanceUse and monitor effectiveness ofquality improvement processMenu 9: Capability to submit electronic data toimmunization registriesMenu 10: Submit electronic syndromic surveillancedata to public health agenciesReport performancePrimary CareInformation Project19
New York State Medicaid Incentives for NCQA PCMH titutional providers) (Professionalproviders)Managed Care1* 5.50per visit 7.00per visit 2.00pmpm2 11.25per visit 14.25per visit 4.00pmpm3 16.75per visit 21.25per visit 6.00pmpmAlso Medicare and a number of NYS commercial insurance pilots**provide additional dollars to clinicians who attain NCQA PCMHrecognition. Current range is 2 to 7 per member, per month.*Medicaid payments for level 1 will end December 2012** Burke G. The Patient-Centered Medical Home: Taking a Model to Scale in New York State. 2011. United HospitalFundPrimary CareInformation Project20
Patient Centered Medical HomesPCIP practices258 sites recognizedLevel 1: 194Level 2: 1Level 3: 63PCMH Status4Pending NCQAEvaluation63Recognition Level 1 4 pending NCQA evaluation(anticipated level 3)1Recognition Level 2Recognition Level 3 194Approximately 1 million cared forat these sitesPrimary CareInformation Project212
AgendaAlignment of HH, PCMH, and MUPatient-Centered Medical HomeMeaningful UseResourcesPrimary CareInformation Project22
Overview of Meaningful UseThe American Recovery and Reinvestment Act (ARRA) authorizes CMS to offer financialincentives to physician & hospital providers who demonstrate “meaningful use” of anelectronic health record (EHR).Meaningful Use is using a certified EHR technology to:1) Improve quality, safety, efficiency, and reduce health disparities2) Engage patients and families in their care3) Improve care coordination4) Improve population and public health5) All the while maintaining privacy & securityPrimary CareInformation Project23
Five Pillars of Meaningful Use1. Improve quality, safety, efficiency, and reduce health disparities Provide access to comprehensive patient health data for patient’s health care team Use evidence-based order sets and CPOE Apply clinical decision support at the point of care Generate lists of patients who need care and use them to reach out to patients2. Engage patients and families Provide patients and families with timely access to data, knowledge, and tools tomake informed decisions and to manage their health3. Improve care coordination Exchange meaningful clinical information among professional health care team4. Improve population and public health Submit immunization, syndromic surveillance and reportable disease data to publichealth agencies5. Ensure privacy and security protection for personal health information Protect confidential information through policies, procedures, and technologies Provide transparency of data sharing to patientPrimary CareInformation Project24
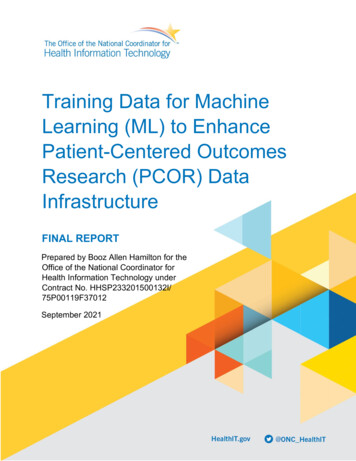
The Vision for Meaningful UseEach stage gets progressively harder to drive toward the ultimate goalThree Stages of Meaningful UseImproved qualityof careStage 3Stage 2Stage 1 520,000 providers will be eligible nationwide to apply for Meaningful Use and receiveincentivesPrimary CareInformation Project25
Stage 1 Meaningful Use MeasuresPrimary CareInformation Project26
OverviewMeaningful Use Objective Measures divided into a “core set” and a “menu set.”“Core set” has 15 measures- must do all 15“Menu set” has 10 measures- must choose 5 Must choose at least one population or public health measureAs part of the “core set,” providers will be required to report Clinical QualityMeasures to CMSNeed to report 6 quality measures 3 core (or use the alternate core quality measures) plus3 specialty measures from a set of 38 additional measuresPrimary CareInformation Project27
Stage 1 Meaningful Use MeasuresMeet all 15CORE SET Measures Submit 5 of 10MENU SET Measures28
Meaningful Use Objective MeasuresMENU SETCORE SET 15 out of 15 5 out of 1020 TOTALAt least 1 public health measureLEGEND:Primary CareInformation ProjectClinical Quality MeasurePublic Health Measure29
Clinical Quality MeasuresPrimary CareInformation Project30
Clinical Quality MeasuresPrimary CareInformation Project31
Clinical Quality MeasuresPrimary CareInformation Project32
Clinical Quality Measures (CQMs) CORE SETPrimary CareInformation Project 6 CQMsSPECIALTY33
Clinical Quality Measures (CQMs) CORE SET 6 CQMsSPECIALTY 3 out of 6LEGEND:3 out of 38Core CQMAlternate Core CQMPrimary CareInformation Project34
Additional Meaningful Use DetailsReporting Period for Meaningful Use Measures 90 days for first year of payment Entire year for subsequent yearsSwitching between Medicaid & Medicare Meaningful Use measures will be the same for Medicaid and Medicare Providers will be allowed to switch one time between the 2 programsFailing to meet criteria For Medicare, if you fail to meet criteria for a year, you lose the incentivepayment for that year For Medicaid, you can reapply the next yearPrimary CareInformation Project35
Overview of PaymentsMedicare Payments are proportional to Medicare allowed charges (75% of total of allowed Part B chargesup to a cap each year) Up to 44,000 over 5 yearsPayments increased by 10% for physicians practicing in a Health Professional Shortage AreaMust participate by 2012 to receive the maximum incentive paymentMedicaid Payments are fixed and not proportional to Medicaid billings.Up to 63,750 over 6 yearsMeet 30% Medicaid patient volume thresholdsIf pediatricians qualify at 20%, only eligible for 67% (2/3) of paymentsMust participate by 2016 to receive the maximum incentive paymentIf you are eligible for both incentives programs, you must select only one.Primary CareInformation Project36
Meaningful Use Payment: Medicare Participation in the Medicare EHR Incentive Program can begin as early as 2011 or as lateas 2014. Incentives end in 2016. Penalties for not meeting Meaningful Use begin in 2015 (1% in 2015, 2% in 2016, and 3% in2017)Primary CareInformation Project37
Meaningful Use Payment: MedicaidMedicaid EHR Incentive programs are voluntarily offered by individual states and may begin asearly as 2011 or as late as 2016. Incentives end in 2021.Primary CareInformation Project38
Stage 2 Meaningful UsePrimary CareInformation Project39
Proposed Rule for Stage 2 Meaningful UsePrimary CareInformation Project40
Primary CareInformation Project41
Primary CareInformation Project42
Primary CareInformation Project43
The Vision for Meaningful UseEach stage gets progressively harder to drive toward the ultimate goalThree Stages of Meaningful UseImproved qualityof careStage 3Stage 2Stage 1 520,000 providers will be eligible nationwide to apply for Meaningful Use and receiveincentivesPrimary CareInformation Project44
In Summary1. Health Homes, PCMH, and Meaningful Use align for improving: patient outcomes patient experience cost containment2. Health IT is a required component of all three programs.3. Additional resources are available from: NYC REACH NYeC IPROPrimary CareInformation Project45
AgendaAlignment of HH, PCMH, and Meaningful UsePatient-Centered Medical HomeMeaningful UseResourcesPrimary CareInformation Project46
NYC REACH Member Resources Resource Library: www.nycreach.org/members/resourcelibrary password protected Medicaid MU Registration Assistance: http://www.nycreach.org/request PCIP Newsletters NYC REACH Digest Emails Webinars and Group Trainings: http://emrtraining.eventbrite.com On the Record (online forum): http://ontherecord.ning.com/Primary CareInformation Project47
NYeC – New York eHealth Collaborative Resourceshttp://www.nyehealth.org NYS HIE Operational Plan http://nyehealth.org/images/files/File Repository16/pdf/nys hie operational plan 2010.pdf Meaningful Use ngful-use NYS Policies olicies RHIOs http://www.nyehealth.org/index.php/resources/rhios Tools http://www.nyehealth.org/index.php/resources/tools Glossary ary#page h 5 FAQ http://www.nyehealth.org/index.php/resources/faq Links http://www.nyehealth.org/index.php/resources/links Events http://www.nyehealth.org/index.php/events Regional Extension Centerhttp://www.nyehealth.org/rec/ Newsletter Primary CareInformation Project48
Some IPRO-Suggested PCMH Links Agency for Healthcare Research and Policy PCMH Resource ommunity/pcmh home/1483 American Academy of Family ership/initiatives/pcmh.html American Academy of Pediatrics: http://www.medicalhomeinfo.org andhttp://www.pediatricmedhome American College of Physicians: http://www.acponline.org/running practice/pcmh/help.htm Center for Medical Home Improvement: http://www.medicalhomeimprovement.org/index.html Community Care of North Carolina: /pcmh-central1/2011-pcmh-resources/ Emisolutions-TransforMed: ed/ IPRO: http://www.ipro.org/index/patient-centered-medical National Committee for Quality Assurance: http://www.ncqa.org/tabid/1302/Default.aspx Patient-Centered Primary Care Collaborative: http://pcpcc.net/ Primary Care Development Corporation: http://pcdcny.org/ Safety Net Medical Home Initiative: ry CareInformation Project49
Meaningful Use ResourcesFederal/State Websites CMS: http://www.cms.gov/EHRIncentivePrograms/30 Meaningful Use.asp ONC Website: http://www.healthit.hhs.gov NYState MU Medicaid Website: https://www.emedny.org/meipass/apply.aspx Certified Health IT Product List Website: http://onc-chpl.force.com/ehrcertVendors Meaningful Use Curriculum Meaningful Use Dashboards/ReportsPrimary CareInformation Project50
Presenter contact informationChristine Stroebel, MPHDirector of Quality ImprovementPrimary Care Information Project/NYC REACHcstroebel@health.nyc.govNatalie Fuentes, MPHClinical Quality ManagerPrimary Care Information Project/NYC REACHnfuentes@health.nyc.govAlan Silver, MD, MPHMedical DirectorIPROasilver@ipro.orgPrimary CareInformation Project51
HH Implementation Session 5: Care CoordinationPresenters:Sara Butterfield, IPROJoseph Twardy, VNS of Schenectady & Saratoga CountiesDate & Time:Wednesday April 11,2012 2:30 pm eastern timeRegistration Link:https://cc.readytalk.com/r/ksfp878hrtzqAll training sessions ( recordings and registrations) will be madeavailable on the Medicaid website.http://www.health.ny.gov/health care/medicaid/program/medicaid healthhomes/ohitt ehr webinars.htmPrimary CareInformation Project52
Meaningful Use Presenters: Christine Stroebel, MPH, PCIP/NYC REACH . Require health information technology to coordinate patient care e.g., patient portal, provider-to-provider portal, RHIO Health Homes: . quality metrics will fulfill NCQA PCMH 2011 requirements Core Set Menu Set Meaningful Use Objectives 15 core objectives 5 of 10 menu set .