Transcription
Medical Home DIY!Self-Guided PracticeTransformationJeff Halbstein-Harris, Patient/AdvocateCollette Carver, Sentara HealthcareSuzanne Berman, Plateau PediatricsC.J. Peek, University of Minnesota
Medical Home DIY! Self-Guided PracticeTransformationDescription: Many tools and resources havebeen developed to assist primary carepractitioners in leading their own qualityimprovement efforts.This session will include a panel of providersand experts who will each describe how theyacquired the necessary skills to lead their staffin transforming the practice into a patientcentered medical home (PCMH).
sFamilies Integration
Defining the medical homeThe medical home is an approach to primary care that is:Patient-CenteredSupports patients in managingdecisions and care plans.ComprehensiveWhole-person care provided by ateamCommitted to qualityand safetyMaximizes use of health IT, decisionsupport and other tools4 Source: www.ahrq.govCoordinatedCare is organized across the‘medical neighborhood’AccessibleCare is delivered with shortwaiting times, 24/7 access andextended in-person hours.
National demand for healthcare transformation.
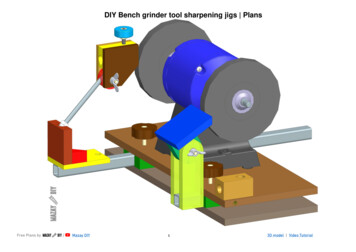
PCMH Population StratificationTargeted Patients with unstable chronicconditions, barriers to behavioral changeand or multiple co-morbiditiesMedical Home contractestablished withpopulation of focusTargeted Patients withuncomplicated chronic conditionsand preventative care needsCareCoordination:Patient/FamilyCoaching& CareCoordinationPracticeFocusSupported Self Management:Acute Care OnlyExtended CareTeam FocusScope, Intensity & Cost of ServicesTargeted Patients with highly complex conditions (Top 1%)Case ManagementFormerly within domain of payer, now within scope of care for PCMHProactive Outreach & Monitoring ServicesInformed Self Service : Education and Self Service InstructionsUsual Care: Diagnosis & Treatment Services0%Distribution of Services across the Population100%6
Population ManagementA new practice skill setProgramManagementRemote Patient ManagementIdentify and StratifyTarget PatientsEstablishGoals & Treatment PlanMonitor PatientOutcomes, Outreachand provide transitionmanagementMeasure ProgramResultsEnrollee HealthManagementServicesCoordinate Care TeamActivitiesCreate Care Action Plan
Fully engaging our patientsHow much should we expect from the mplianceComorbidityAssist withreportingoutcomes toPCPDiscoverActivateMonitorPatient ComplianceDisease Self MasteryLearning BarriersCoordinateEvaluatePrimary and Secondary PreventionSelf MonitoringAction PlansUrgent Care GuidelinesCommunication (Patient Portal)Bio-Psycho-Social HistoryGoals, Wants, NeedsEducateInsurance ExchangePrimary Care MedicalHomePatient ContractIdentify and linkresources: ReferralsTransportation, NutritionPatient Peer Groups
A patient’s perspective Me: 58 y/o male5 physicians3 chronic conditions (diabetes, Hepatitis C, RSD)Comorbidity’s: Retinopathy, autonomic neuropathyBehavioral Health: PTSD, Chronic DepressionOnset dates: Diabetes age 10, Hepatitis age 24, RSD age 55, retinopathy age 49, neuropathyage 55, PTSD age 33, chronic depression age 33.Meds 7Technology includes CAGMFunctional status: Retired SSDI due to RSD and autonomic neuropathy. Able to work at deskfor periods up to 3 hours, able to drive for up to 3 hoursSocial Status: Married 20 years, no children.Education: BS Economics , AS Respiratory Therapy; RCVT, RPFTFormer occupation: Director of High Risk Case Management; Director of Clinical InformaticsDirector of Cardio-Pulmonary RehabilitationRecent Losses: Occupation and Avocational activity (Private Pilot)Goals: Control CD process and part time work in field of passion
Sorting, distributing, analyzing, paying, communicating,why the heck won’t my records synchronize?
2 hours later , 3 Starbucks, one fruitsmoothie, 8 units of Apidra
How much more can we take!
PCMH at of “Medical Neighborhood”Health IT nt-CenteredMedical Home PharmacyHospitalOral h Health ITSpecialty &SubspecialtySkilledNursingFacility
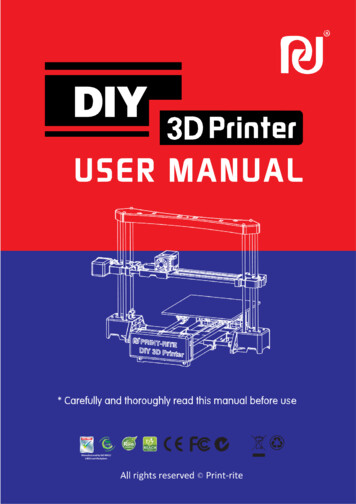
Without data interchange we areNon Integrated SystemIntegrated System with e-HR“dead in the water”PHRPCMHSingle Practice EMRSiloCommunication BarrierLocal hospital riptsPharmacyLocal PharmacyHealth Info ExchangeVarious LabsHospitalSystem
NCHICA Proposes ArchitectureA long way from vision to reality
Stopping the revolving door"Go to the people, live with them, learn from them.Start with what they know, build with what they have."Lao TzuAfter ten years work with 3000 pulmonary and cardiac diseasepatients I learned some very simple lessons: We are an interdisciplinary workforce, our patients count on ourability and desire to share our treatment plans and assessments We may have individual treatment plans by sub-specialty orepisode of care but we all share in the development of a “LifePlan” engaging patients and families in their own self-defined“Plan of Care” Self mastery starts with understanding how the system works,who the cast of actors are and everyone's responsibility.
Preparing for a trip
My PHR
How I connected my system Located physician with knowledge of health datainterchange and motivation to heal Located surgeons who would treat me as equal Located tools online that worked and wereinteroperable Created my own accounts {HealthVault,Connected to Connected to CVS, SPINN secure Communicationand LabCorp
Decision Support
Details of record source
Medication ReconciliationWho ordereddrugWhere did record comefromIs this patient staying with medicalhome or Dr. Shopping
Providers and Contacts
Monitoring
Educating patients to select resourcesfrom published information
Using process measures to make decisions whenchoosing providers
Why Wouldn’t Patients Recommend
If patients are readmitted is that the hospital issue ordoes it say something about the supportingcommunity?
Would you go somewhere with noreported data?
Teaching patients and families to evaluate integrationbased on hospital readmission rates
Medical Home DIY!Self-Guided PracticeTransformationJeff Halbstein-Harris, Patient/AdvocateCollette Carver, Sentara HealthcareSuzanne Berman, Plateau PediatricsC.J. Peek, University of Minnesota
Guiding PrinciplesSentara Medical GroupCare ModelPatient-CenteredData Driven Decision MakingStandardizationPractice at Highest Level ofClinical LicensePatient-Centered Medical HomesPrimary Care Teams Standardization of patient experience Same Day Appointments 7 day hospital follow up EMR Patient EMR Portal Evidenced based guidelines Best practice alertsAimImprove the health of our patientsDeliver clinical and service excellencethat is cost effective and promotes anoptimal experience for all.Care ManagementRN/Social Worker/Pharm D Hospital follow up Transitional contact after facility care Disease Management High Risk population management Managing psychosocial barriers Behavioral Health Integration Utilization analysis Coding optimizationPopulation ManagementRN/ LPN/MA/Secretaries Preventive Care TelephonicOutreach Preventive Care and ScreeningRegistries Health Maintenance review Chronic Disease Registries At Risk and Full Risk Patientpopulations with PayersIntegration between PCP, Specialty andCommunity yHealth Centers Clinically Integrated Network with communityproviders Hospitalists and PCP communication Specialist and PCP care agreements Health Plan collaborationsSupporting programs: Leadership and Professional Development, Safety andRegulatory, Quality Committee, IT and Analytics, Health System
Medical Home DIY!Self-Guided PracticeTransformationJeff Halbstein-Harris, Patient/AdvocateCollette Carver, Sentara HealthcareSuzanne Berman, Plateau PediatricsC.J. Peek, University of Minnesota
DIY MedicalHomeTransformationSUZANNE BERMAN, MD, FAAP
Transformation takes timeNo consultantcan come inand do an“instantmakeover” toPCMH-ify yourpractice.
Assemble your teamTeam Leads: Project manager (lead): to assign, track, andcheck pieces for completion. Needs to 1) beOCD and 2) have nag power. Provider (lead)– to write/approve the clinicaldecision-making pieces, to provide input forclinical protocols, and to champion providerworkflow changes Administrator (lead) – to write/approve policiesand procedures (clinical and nonclinical) and tochampion front desk, clinical staff, and backoffice workflow changes.
Assemble your teamTeam Supports: Nonclinical and clinical staff (support) – toprovide feedback on current practices andproposed changes Patient/parent representatives (support) – toprovide feedback on current practices andproposed changes Computer geek (support) – to prepare andanalyze data for reporting. Needs familiarity withExcel, screen captures, PDF creation, etc. Wordsmith (support) – to proofread others’materials; to draft protocols and/or find goodones to borrow on the Internet.
Assemble your tools Web-based project management tool Dividing projects up into smaller tasks Assigning people to tasks Letting team members provide status reports Collaborative document writing Scheduling meetings and deadlines Sending reminders Spreadsheet software Screen capture and screen capture editor –essential for documention of computer-basedworkflow
Protected time Non-administrators MUST have protected time towork on transformation. Even if they have some “interstitial downtime,”most staff have difficulty working ontransformation in 5- and 10-minute pieces. If you want transformation to be a priority,schedule (paid) blocks of time for each staffmember to work on their pieces. To prevent “playing” during protected time, usevery short deadlines with frequent smalldeliverables; make it an activemeeting/discussion with the transformationleader, rather than a self-paced activity.
Getting started is thehardest partPICKING THE FIRST PROCESS TO IMPROVE CAN BEOVERWHELMING!
Your first change: choosesomething with benefitHuddles: reduce overtime Better lab, x-ray, and referral tracking: reduceovertime Recall: more remunerative schedule saturation Same day appointments: fewer no-shows Team engagement: better employee morale andlower turnover
Your second change:what bugs you? Find a common annoyance in your practice thatall staff can rally around Taming the telephone or fax? Message tracking? Patient wait times?Avoid “picking on” one department
Other longer-term or moreexpensive transformations:do later Extending evening/weekend hours Hiring, training, and implementing a carecoordinator Formal comanagement agreements Hospital and ER tracking/coordination Empanelment matching Culturally and linguistically appropriate teaching
Medical Home DIY!Self-Guided PracticeTransformationJeff Halbstein-Harris, Patient/AdvocateCollette Carver, Sentara HealthcareSuzanne Berman, Plateau PediatricsC.J. Peek, University of Minnesota
Integrating Behavioral Health with PCMH Practices:An overview of Why, What, HowC. J. Peek, PhDProfessor, Dept. of Family Medicine and Community HealthUniversity of Minnesota Medical Schoolcjpeek@umn.eduPatient Centered Primary Care Collaborative (PCPCC)Panel: Medical Home DIY--Self-Guided Practice TransformationNovember 13, 2014Washington, DC50
Why should BH be part of the PCMH?PCPCC slide th-integration-pcmhPCPCC slide contentsPrevalence Prevalence of BH, burden of illness, primaryand burden care as de-factor MH system, behavioralfactors in medical illnessesUnmetneedsUntreated persons, challenge of access;problems of separate and parallel systemsCostIncreased health cost with BH co-occurrence;lower cost when BH treated—ROI; increasedemployee costsOutcomesImproved MH outcomes; improved physicalhealth outcomesExperienceImproved patient and provider satisfaction51
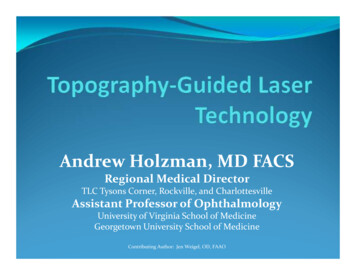
A legacy of separate and parallel systemsMedical CareMental Health CareA forced choice between: 2 kinds of problems 2 kinds of clinicians 2 kinds of clinics 2 kinds of treatments 2 kinds of insuranceIntegrated behavioral health leads to a better matchof clinical services to the realities that patients andtheir clinicians face daily.Original Source: CJ Peek 19965252
What is integrated BH?AHRQ Lexicon functional definition“What”: (An ordinary two-sentence definition)“How” functions:1. A practice team tailored to the needs of each patient andsituation (3 sub-clauses)2. With a shared population and mission3. Using a systematic clinical approach (6 sub-clauses)“Supported by” functions:4. Supported by 1) reliable office processes, 2) leadershipalignment, and 3) sustainable business model5. Ongoing QI and measurement of effectiveness (2 sub-clauses)6. With a community or population expecting that BH and PC willJeffrey ( 1995)—Joy of Herding Catsbe appropriately integrated Peekas a&standardof care53
Example—plain old glossary (AHRQ 2013)integrationacademy.ahrq.gov/sites/ default/files/Lexicon.pdf54
Scope of Integrated BHCondition-Centered and Person-CenteredIntegrated care forMH conditions Depress / anxiety Substance abuse ADHD OtherIntegrated care forMedical conditions Diabetes / BP / obesity Heart disease Childhood chronic illness Stress-linked phys sxCJ Peek & Mac Baird, 2010;PCPCC 2014Integrated care for Persons: Social and care complexity Distress, distraction & readiness to engage in care Social safety, support & participation Understanding own health situation / health literacy Health behavior change Organization of care / relationships in health system55
Questions to ask early on with yourconsultant “hat” onWho is your population—who do you serve? What are theBH aspect of their needs? How well are those needs met?One way to get at that:“Who feels what kind of pain when it comes to the BHaspect of doing your job in your PCMH?”What initial target for BH integration to start with?Significant to the practice; can actually get it goingWhat financial arrangement at first? What payment orbusiness models will you use to stay in business at first?See this panel’s Berman and Carver presentations!56
Only a sample of resources for actionAHRQ Integration Academyintegrationacademy.ahrq.govLit repository; lexicon (definitions); Atlas ofintegration measures; soon on-linecommunity, “playbook”Center for Integrated HealthSolutions (CIHS)www.integration.samhsa.govFrameworks and models; guides andarticles on financing, workforce, clinical,administrativeAIMS Center—AdvancingInnovative MH Solutions; U ofWashington; aims.uw.eduImplementation guides, resource library,research; pieces on teams, roles,workflows, financing, examplesPCPCC Behavioral Healh SIGSlide decks; monthly phone calls orpresentations on topics suggested ration-pcmhCenter for Integrated Primary Care. Training, literature, websites, reports,www.umassmed.edu/cipc/videos,Collaborative Family HealthcareAssociation: www.cfha.netMembership organization, journal,conferences, webinars, listserv, blog 57
References AHRQ Academy for Integrating Behavioral Health and Primary Care:integrationacademy.ahrq.gov/ AIMS Center (Advancing Innovative Mental Health Solutions), Univ of WA. aims.uw.edu Center for Integrated Primary Care: http://www.umassmed.edu/cipc/ Collaborative Family Healthcare Association: www.cfha.net Evolving Models of Behavioral Health Integration in primary Care. Milbank Memorial Fund2010. http://www.milbank.org Peek & National Integration Academy Council. Lexicon for Behavioral Health and PrimaryCare Integration. AHRQ 2013: integrationacademy.ahrq.gov/sites/ default/files/Lexicon.pdf National Alliance on Mental Illness. Integrating Mental Health & Pediatric Primary CareResource Center: http://www.nami.org SAMHSA/HRSA Center for Integrated Health Solutions: http://www.integration.samhsa.gov Kathol, R., deGruy, F., & Rollman, B. (2014). Value-based financially sustainable behavioralhealth components in patient-centered medical homes. Annals of Fam Med Vol 12, No. 2. Melek, S. (2012). Milliman Research Report: Bending the medicaid healthcare cost curvethrough financially sustainable medical-behavioral integration Manderscheid R. & Kathol R. (2014). Fostering sustainable, integrated medical and behavioralhealth services in medical settings. Annals of Internal Medicine; 160:61: 61-6558
Medical Home DIY!Self-Guided PracticeTransformationJeff Halbstein-Harris, Patient/AdvocateCollette Carver, Sentara HealthcareSuzanne Berman, Plateau PediatricsC.J. Peek, University of Minnesota
Sentara Medical Group Care Model Patient-Centered Medical Homes Primary Care Teams Standardization of patient experience Same Day Appointments 7 day hospital follow up EMR Patient EMR Portal Evidenced based guidelines Best practice alerts Care Management RN/Social Worker/Pharm D Hospital follow up