Transcription
Esthetic Templates for Complex Restorative Cases:Rationale and ManagementDEAN E. KOIS, DMD*KYLE K. SCHMIDT, DDS*ARIEL J. RAIGRODSKI, DMD, MS†ABSTRACTComplex restorative cases require difficult clinical decisions regarding the final estheticoutcome in which the operator must visualize the definitive restorative position of the teeth.These critical decisions need to be made before treatment is rendered. Communicating thesedecisions to the patient and the treatment team are crucial prior to achieving clinical success.The esthetic template is the conduit for providing excellent communication. The selection ofthe appropriate esthetic template is based on four sequential decisions: (1) dentofacial analysis,(2) blueprint development, (3) matrix management, and (4) template application. When utilizing an esthetic template, the clinician must know where the teeth should be placed based on adentofacial analysis. The dentofacial analysis must then be communicated to the laboratory,and then a blueprint is developed from the diagnostic casts. A matrix is then fabricated fromthe blueprint and then related back to the existing dentition. The esthetic template is an invaluable communicator that can be utilized in office, with the patient at home, or even within themultidisciplinary treatment team. Clearly, the effective use of esthetic templates demonstrates areversible way to visualize difficult esthetic decisions before any irreversible procedures arecompleted. Esthetic templates are a physical means of communication that provide the patient,technician, and multidisciplinary team an instrument to predictably manage complex restorativecases. The purpose of this article is to present a rationale for esthetic template selection andmanagement of several techniques for complex restorative cases.CLINICAL SIGNIFICANCEComplex restorative cases require difficult clinical decisions regarding the final estheticoutcome in which the operator must visualize the definitive restorative position of the teeth.The use of an esthetic template commensurate with a rationale for selection enables the operator, patient, and entire interdisciplinary team to visualize the final esthetic outcome.(J Esthet Restor Dent 20: 239–250, 2008)treatment is based mainly on diagnosis and treatment planning.1Complex restorative cases requiredifficult clinical decisions regardingINTRODUCTIONDentistry continues to evolvewith new techniques andmaterials; however, the success of†the final esthetic outcome inwhich the operator must visualizethe definitive restorative positionof the teeth. These critical*Graduate student, Graduate Prosthodontics, Department of RestorativeUniversity of Washington, Seattle,Associate professor and director, Graduate Prosthodontics, Department of RestorativeUniversity of Washington, Seattle,Dentistry,WA, USADentistry,WA, USA 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .DOI 10.1111/j.1708-8240.2008.00186.xVOLUME 20, NUMBER 4, 2008239
E S T H E T I C T E M P L AT E S F O R C O M P L E X R E S T O R AT I V E C A S E Sdecisions must be made beforetreatment is rendered. Communicating these decisions to the patientand the treatment team are crucialprior to achieving clinical success.2The esthetic template isthe conduit for providingexcellent communication.Esthetic templates are not provisional restorations; the templatesdescribed in this article are preprovisionals that incorporate diagnostically driven matrices thattransfer predicted tooth positionbefore any irreversible proceduresare performed. Confirming one’sclinical impression in the diagnostic phase reduces the risk forproblems during the course oftreatment. The goals of esthetictemplates are (1) patient visualization, (2) laboratory communication, and (3) clinician verification.These templates allow the patientto visualize predicted treatmentoutcomes directly in the mouth.Moreover, the esthetic templatecan be utilized to communicatekey esthetic information to thedental technician. Traditionally, inremovable prosthodontics, a waxrim has been used to evaluateprospective tooth position andmaxillary plane orientation.3By creating an esthetic templatefor fixed prosthodontic cases,the clinician can verify the finaltooth position before any irreversible procedures are performed.In essence, this is the wax240rim concept applied todentate patients.Various esthetic diagnostic techniques have been described in theliterature, such as direct compositeresin mock-ups, the use of indeliblepen, computerized dental imaging,intraoral tooth reshaping, anddenture teeth setup. Gureldescribed a “preevaluative temporary technique,” which enables theclinician and patient to visualizethe definitive outcome. Once theesthetic goals are confirmed, thedentist can start preparing the teeththrough the preevaluative provisional, which has been bonded tothe teeth, utilizing it as a toothreduction guide.4 Presently, onetechnique that facilitates estheticdiagnostics for complex clinicalscenarios has not been described inthe literature. Moreover, a rationalefor appropriate indications is stillneeded. Understanding which typeof template works well and whereit works is critical to which esthetictemplate the clinician chooses. Theselection of the appropriate esthetictemplate is based on four sequential decisions: (1) dentofacial analysis, (2) blueprint development,(3) matrix management, and(4) template application.The purpose of this article is topresent a rationale for esthetic template selection and management ofseveral techniques for complexrestorative cases. 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .1 . D E N T O F A C I A L A N A LY S I SIn order to select the proper template, the most important questionto answer is where the teeth belongin the face (Figure 1). Based on theclinician’s dentofacial analysis,tooth position can be described inthree planes of space: vertical,horizontal, and sagittal. The vertical plane of space allows the visualization of the incisal edge length,proposed gingival location, andrelative position of the maxillaryocclusal plane (Figure 2A,B).5 Thehorizontal plane allows the clinician to visualize the anterior andposterior position of the incisaledge (Figure 3). The sagittal planecomprises the dental midline andthe mesial and distal position ofthe teeth. Typically, the cliniciancombines movements in theseplanes of space in order to visualize the final tooth position. Oncethe desired position of the teethhas been verified, the clinicianmust decide whether laboratorysupport is needed.If minimal alteration is indicated,the clinician may choose betweenthe direct composite resin mock-uptechnique, dental imaging, maskingof selected areas of the teeth withan indelible black marker, orremoval of tooth structure.Minimal alterations are performedin cases such as mild attrition, milderosion, peg laterals, or diastemata.The direct composite resinmock-up technique is highly
KOIS ET ALesthetic and an excellent patientand laboratory communicator, thusallowing for an accurate representation of the proposed treatment(Figure 4A–C).6 However, this technique requires longer chair time, istechnically demanding, and is bestsuited for anterior esthetic cases.Figure 1. Full preoperative facial view allows the clinicianto perform a dentofacial analysis.ADental imaging can be effective forvisualization; however, a twodimensional picture of a threedimensional object does notprovide critical three-dimensionalinformation. The technique ofmasking selected areas of the teethwith an indelible black markerrequires minimal chair time and iseasy to perform but is restricted toshortening teeth. Recontouringteeth with a bur is also relativelysimple to perform; however, it isan irreversible procedure.Extensive alterations are performedin cases such as moderate-severeattrition and erosion, modificationsin contour and position, missingteeth, and orthodontic movement.Often, this type of alteration isoutside the clinicians’ comfort leveland overly time consuming toperform chairside. If extensivealteration is indicated, then laboratory support is utilized to create ablueprint, which is the envisionedBFigure 2. A and B, Frontal view of lips at rest position and high smile are used to visualize the definitive tooth positionin the vertical plane.VOLUME 20, NUMBER 4, 2008241
E S T H E T I C T E M P L AT E S F O R C O M P L E X R E S T O R AT I V E C A S E SFigure 3. Lateral view of smile is used to visualize toothposition in the horizontal plane. Note the current positionis retroclined compared with the desired position.comprehensive plan based onthe dentofacial analysis, onthe diagnostic cast.clinician to analyze the blueprintupon return from the laboratoryand ensure that it satisfies theesthetic vision.2. BLUEPRINT DEVELOPMENTA diagnostic wax-up is createdbased on the clinician’s dentofacialanalysis and esthetic judgmentcommensurate with the patient’svision. Some restorative casesrequire a multidisciplinaryapproach with the involvement ofvarious specialties.7 More specifically, orthodontics necessitatessome form of setup for treatmentvisualization. This information canbe transferred to the laboratorytechnician, who can now developthe blueprint. Before movingahead, it is important for the242After the analysis, the clinicianmust decide whether the blueprintis additive or subtractive. Somealterations are more predictablethan others when utilizing esthetictemplates. Movement of teeth apically and posteriorly is more difficult, if not impossible, to perform.These movements are consideredsubtractive procedures, whichinclude shortening teeth, narrowingteeth, and moving teeth lingually.This type of movement haslimitations because the teeth areusually in the way. Masking or 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .recontouring teeth can shortenthem as described; however,moving teeth lingually is impossibleto achieve with an esthetic template. If the treatment plan incorporates lingual movement, then thebest way to communicate with thepatient is the blueprint itself. Asopposed to moving teeth apicallyand posteriorly, moving teeth incisally and anteriorly is predictable,and there are many ways to accomplish this outcome. These movements are considered additiveprocedures, which include lengthening teeth, widening teeth, movingteeth facially, and replacing missingteeth. Once the clinician knowsthat the alteration is additive, he orshe is ready to create the matrix.3 . M AT R I X M A N A G E M E N TAs soon as the clinician has determined that the blueprint is additive, the next step is to create amatrix and transfer the blueprintto the mouth. At this point, theclinician knows the blueprint andneeds to relate the matrix back tothe existing dentition. In mostcases, transferring the blueprint tothe mouth is accomplished with amatrix fabricated off the diagnostic wax-up/setup. These matricescan be fabricated off the castusing two distinctive approaches:a vacuum-formed template or adirect impression with eithersilicone putty or irreversiblehydrocolloid as matrix material.These materials essentially
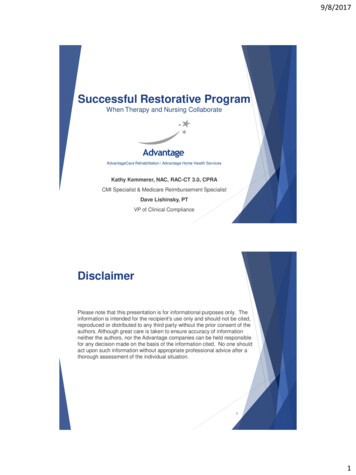
KOIS ET ALABCFigure 4. A, Initial image prior to the application of direct composite resin mock-up. Note no tooth display at restposition. B, Application of a direct composite resin mock-up (can be performed freehand or with a palatal matrix).C, Completed direct composite resin mock-up.duplicate the blueprint and createa vehicle for its transfer to themouth. The matrix is then filledwith a provisional material,approximated over the existingdentition, and allowed to cure.This technique allows a simple,low-cost way to verify plannedtooth position in an esthetic way.With some treatment strategies,the blueprint matrix cannot beapproximated over the existingdentition because extensive anterior or sagittal movement wastreatment planned. Therefore, atechnique that uses a referencepoint other than the teeth must beutilized. The most stable referencepoint to use is the palate whenthe teeth are undergoingorthodontic movement. Typically,when using the palate as a reference point, everything lingual tothe incisal edge is removed fromthe template, allowing it to beproperly oriented. This matrix isthen filled with a provisionalmaterial and approximatedover the diagnostic castusing an indirect technique(Figure 5A–D).Once the clinician has made thechoice of which template techniqueto utilize, the last decision to makeVOLUME 20, NUMBER 4, 2008243
E S T H E T I C T E M P L AT E S F O R C O M P L E X R E S T O R AT I V E C A S E SABCDFigure 5. A, A frontal preoperative smile of a patient requiring a comprehensive multidisciplinary treatment. An indirecttechnique will be used to simulate the prospective teeth position. B, A frontal preoperative view. C, A blueprintis created on the mounted diagnostic casts using a combination of orthodontic setup and diagnostic wax-up.D, Completed indirect removable template position on the diagnostic cast. Note the extensive alterations planned.is which material to select for theesthetic template. One of twochoices can be applied for esthetictemplate management. These materials consist of polymethyl methacrylate acrylic (PMMA) andcomposite resin (bis-GMA,Protemp 3, Garant, 3M ESPE, St.Paul, MN, USA). Both of thesematerials provide excellent esthetics, color, detail reproduction, andare relatively easy to use.A key factor in which of these twomaterials to choose is whether thistemplate should be removable orfixed. If the template needs to be244easily removed, then PMMAshould be the material of choicebecause the clinician can remove itduring polymerization to establisha path of draw. Large gingivalembrasures can pose a risk forlocking the template onto theteeth; wax or any blockout material should be considered. If thetemplate does not need to beremoved, bis-GMA is typicallyconsidered. These templates canthen be bonded to the teeth andworn as trial restorations orused as preparation guides foractual tooth preparation(Figure 6A–C). 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .4 . T E M P L AT E A P P L I C AT I O NEsthetic templates possess a multitude of applications. The primaryuse of these templates in office isto facilitate clinician/patient communication. Allowing the patientto visualize the anticipated treatment result can align the clinician/patient esthetic vision whileconfirming the clinician’s clinicalimpression. Typically, patients willhave some esthetic changes or affirmations about the template. Thetemplate promotes a dialoguebetween the clinician and patientthat possesses a much higher valuethan trying to explain the
KOIS ET ALABCFigure 6. A, Initial smile prior to using a fixed template. B, A blueprint was created with the diagnostic wax-up.C, Completed fixed bis-GMA template in the patient’s mouth during smile.treatment goals on a mounted setof diagnostic casts. The patientessentially wears the final resultbefore any irreversible proceduresbegin. If esthetic modifications arenecessary to the matrix, then thesechanges are communicated to thedental technician, allowing theblueprint to be modified beforetreatment ever commences.These templates can be designed asremovable appliances and given tothe patient to take home. Withcomplex restorative cases, thealterations are usually significant.Treatment discussions can be veryoverwhelming for some patients;the template allows the patient anopportunity to take his/her timewhile retaining a visualization tool.At home, opinions of friends andfamily can aid in the patient’sdecision process.Prerestorative template management facilitates multidisciplinarycommunication. The esthetic template enables the entire treatmentteam to visualize the definitivetreatment outcome in the patient’smouth in their own respectivepractices. Esthetic templates can beused to communicate periodontalprotocols, such as crown lengthening, implant position, and mucogingival procedures. Visualization ofpredicted esthetic outcomes is noteasily managed when teeth are notin the ideal position and theirshape and contour are not optimal.As with many multidisciplinarycases, tooth provisionalizationcannot always be performed priorto orthodontic procedures, and theVOLUME 20, NUMBER 4, 2008245
E S T H E T I C T E M P L AT E S F O R C O M P L E X R E S T O R AT I V E C A S E SABCFigure 7. A, Preoperative smile prior to orthodontic movement. B, Blueprint was created with orthodontic setup anddiagnostic wax-up. C, Completed vacuum-formed matrix to verify orthodontic space appropriation.Figure 8. Silicone putty matrix was generated from theblueprint to guide orthodontic treatment of the canine,utilizing the palate as a reference. Note that additionalmesial and apical movement of the cuspid is requiredto approximate the matrix.246 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .esthetic template allows an orthodontist to utilize the blueprint inthe mouth as well (Figures 7A–Cand 8). Another application isusing the matrix from the blueprintto verify proper tooth alignment oreven movement progression. Thistechnique is more predictable thantraditional methods of measurement off the diagnostic wax-upand arbitrary relation back to thepatient’s mouth. Understanding therationale and management ofesthetic templates allows the clinician to apply the template not onlyin the diagnostic phase but alsoduring various stages of treatment.
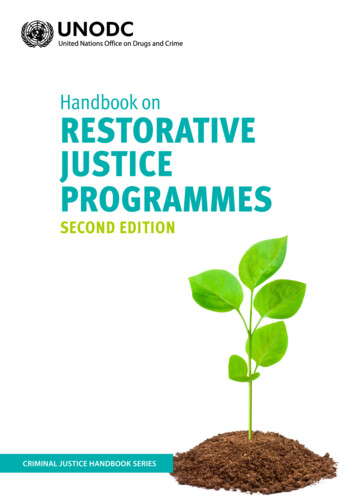
KOIS ET ALFigure 9. Step 1: dentofacial analysis—preoperative viewof the patient’s smile.Figure 11. Step 3: matrix management—vacuum-formed matrix prior to filling up withpolymethyl methacrylate acrylic.S U M M A RYIn summary, a diagnostic rationalefor esthetic template fabricationand management has been presented. Four sequential decisionsthat a clinician must contemplatewere discussed (Figures 9–12).When utilizing an esthetic template, the clinician must knowwhere he or she wants to put theteeth based on a dentofacialanalysis. The dentofacial analysismust then be communicated toFigure 10. Step 2: blueprint development—diagnosticwax-up.Figure 12. Step 4: template application—polymethylmethacrylate acrylic template after vacuum-formed matrixremoval.the laboratory and then a blueprint is developed from the diagnostic casts. A matrix is thenfabricated from the blueprint andthen related back to the existingdentition. The esthetic template isan invaluable communicator thatcan be utilized in office, with thepatient at home, or even withinthe multidisciplinary treatmentteam. Clearly, the effective use ofesthetic templates demonstrates areversible way to visualize difficultesthetic decisions before any irreversible procedures are completed.Esthetic templates are a physicalmeans of communicationthat provide the patient,technician, and multidisciplinaryteam with an instrument topredictably manage complexrestorative cases.DISCLOSUREThe authors do not have anyfinancial interest in the companiesVOLUME 20, NUMBER 4, 2008247
E S T H E T I C T E M P L AT E S F O R C O M P L E X R E S T O R AT I V E C A S E Swhose materials are included inthis article.REFERENCES1. Amsterdam M. Periodontal prosthesis:twenty-five years in retrospect. AlphaOmegan 1974;67(3):8–52.2. Marzola R, Derbabian K, Donovan TE,Arcidiancono A. The science of248communicating the art of esthetic dentistry: part I: patient-dentist-patient communication. J Esthet Dent 2000;12:131–8.5. Kokich V. Esthetics and anterior toothposition: an orthodontic perspective. partII: vertical position. J Esthet Dent1993;5(4):174–8.3. Hickey JC, Zarb GA. Boucher’s prosthodontic treatment for edentulous patients,9th ed. St. Louis (MO): CV Mosby;1985.6. Marcus R. Treatment planning and smiledesign using composite resin. Pract ProcedAesthet Dent 2006;18(45):235–41.4. Gurel G. Permanent diagnostic provisionalrestorations for predictable results whenredesigning the smile. Pract Proced AesthetDent 2006;18(5):281–6.7. Magne P, Magne M. The diagnostictemplate: a key element to the comprehensive esthetic treatment concept.Int J Periodont Rest Dent 1996;16:561–69. 2008, COPYRIGHT THE AUTHORSJ O U R N A L C O M P I L AT I O N 2 0 0 8 , W I L E Y P E R I O D I C A L S , I N C .
treatment. The goals of esthetic templates are (1) patient visualiza-tion, (2) laboratory communica-tion, and (3) clinician verification. These templates allow the patient to visualize predicted treatment outcomes directly in the mouth. Moreover, the esthetic template can be utilized to communicate key esthetic information to the dental technician.