Transcription
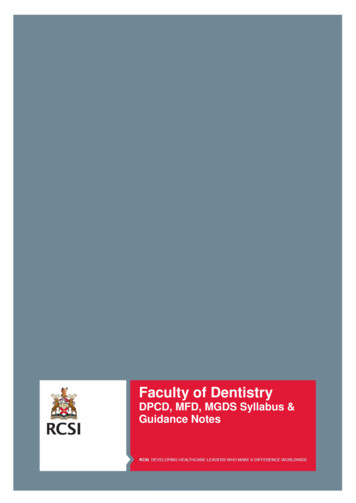
Cosmetic or esthetic dentistry?Louis Z. G.Touyz, BDS, MSc(Dent), M Dent (POM)*/Eli Raviv, DMD"/Mili Harel-Raviv, DMD'"This artide, tiirough presentation ot case studies, defines differences and suggests separate definitionstor the terms cosmetic dentistry and esthetic dentistry. Dentistry strives to emuiate iiarmonious form andfunction tor therapy, and modification of appearance is an intégrai part of dentai treatment. Cosmetic dentistry suggests a certain accommodation and is a compromise cf current teci nclogy Cosmetic dentistry iscommonly selected as an interim procedure tiiat does not necessariiy tunction ideaiiy and does not aiwaysemuiate the pristine state ot a natural dentition. Esthetic dentistry requires iess accommodation, incorporates acceptabie biologic technology tor long-term survivai. functions suitahiy. and mimics the pristineState of the naturai dentition. Cosmetic and esthetic dentistry are different in definition, concept, and execution. (Quintessence Int 1999;30:227-233)Key words: cosmetic dentistry, esthetic dentistry, proslhodonticsn the pursuit of excellence, plastic surgery has consistently emulated the natural state of optimal humandevelopment and health.'- Conversely cosmetic plasticsurgery can permanently alter the human body and notmiinic the pristine state.' For example, tattooing, elongating necks, and ear lohe or lip mutilation are attractive in certain cultures, but can be classified by currentsurgical standards as primitive cosmetic plastic surgery, Dental treatment that modifies crofacial appearancecan be considered part of plastic surgery, becausephysical appearance is critical to both specialties.'- -"-*Cosmetic surgery and esthetic surgery have been traditionally regarded by many surgeons and health careproviders as synonymous with an identical philosophical approach. In addition, the majority of dental patients, dentists, and personnel of dental insurance companies have mistakenly believed that cosmeticdentistry and esthetic dentistry are identical entities."-"*Most dental therapies treat both hard and soft tissuesto modify appearance." If modification of appearanceinvolves elimination of component parts, it can be technicaDy termed mutiiation; when modification consistsof changing the shape of a part, it is called dejorma-I'Diiector and Associate Professor of Periodontics. Faculty of Dentistry,UcGiii Uniuersity, Montreai, Quebec, Canada."Director of Prosthodortics, Sir Mortimer B, Davis-Jewisti GêneraiHospitai, Mortreai; Assistanl Professor, Faculty ol Dentistry, McGiliUniversity, Montreal, Qjebeo, Canada,' 'Director, Preuenlive and Community Dentistry Division, and AssistantProtessor, Faculty of Dentistry, McGiil Universily, Montreal, Quebec,Canada.Reprint requests: Dr Louis Touyz, Faculty of Dentislry, MoGill University,/ W Docteur PenfielO Streel, Montreal, OC H3A 1A4 CanaOa. E-maii'touyz medcor.mogili.caQuintessence Internationaltioii.'- When deformation or mutilation is performedduring dental treatment, the clinical results commonlydetermine if the procedure is esthefie or cosmetic denfistry.'"" Specific guidelines as to what is esthetic andwhat is cosmetic dentistry are rare: The Glossary ofProsthodontic Terms fails to define cosmetic dentistry, 'Patients, dentists, other health care professionals,third-party health care providers, and insurance companies are confused about what constitutes esthetic orcosmetic dentistry.' -'' Tbis article presents workingdefinitions for cosmetic dentistry and esthetic dentistry, differences between them, and, through casestudies, attempts to define specific concepts for thetwo ways of management.TISSUE ACCOMMODATION AND REACTIONCosmetic dentistry demands some physical accommodation and manifests some physiologic tolerance orreaction. The artificial crown on the maxillary rightcentral incisor (Fig la) has created irritation of thegingival fissue with violation of the biologic width, byoccupying dentogingival space intended for gingivalfibers and ¡unctional epithelium. A low centralfrenum, deep pericoronal pocketing extending fromthe free gingival margin to the base of a pocket thatexceeds 4 mm, and interdentai papillary infiammatoryhyperplasia are present. This is cosmetic dentistry thatcompromised tissue tolerance, and vital tissue accommodation evoked a soft tissue reaction. After specific periodontal treatment, a new crownwas piaced on the maxillary right central incisor (Figlb); the soft tissues are within normal limits and227
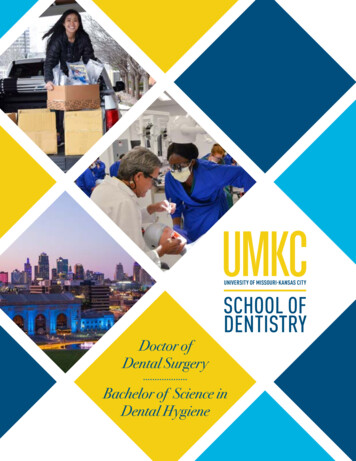
Touyz et aiFig l a Ccsrnetic crown on the maxiliary right central inoisorImmediate crown piacement satisfied instant appearancedemanda but induced a periccrcnai seit tissue reactionFig I b Esthetic crown on the maxiiiary right centrai incisor. Afterperiodontal intervention, the permanent crown satisfies appearance demands witb minimai soft tissue reaction.Fig 2a Provisionai crowns on tbe maxiliary anterior teeth. Theywere purposefuliy oonstructed to primarily meet immediate cosmetic needs. Functional demands are ol secondary importance.Fig 2b Maxiliary fixed partiai dentures. Desirabie form, appearance, and function are provided with this esthetic resulLhealthy. This is an example of esthetic dentistry,requiring minimai tissue accommodation and tolerance.PROVISIONAL VERSUS PERMANENTA provisionai fixed partiai denture (FPD) of 6 singleunits placed on maxillary teeth (canines, central incisors, and lateral incisors) during restorative treatment(Fig 2a) can be pleasing in appearance, provide temporary coverage of prepared teeth, and be functional.Selection of specific techniques and materials for provisional artificial crowns is acknowledged as a shortterm, interim measure. This could be an example ofcosmetic dentistry consciously selected as a temporarytherapeutic measure. The definitive maxillary FPD,which has an improved appearance and suitable function, is purposefully intended for long-term survival {Fig2b), but most biomaterials, including porcelain fused tometal (PFM), are not expected to endure permanently.IDEAL FUNCTIONAttempts to provide cosmetic dentistry can result inmutilated tceth ' (Fig 3). Major reduction of the edgesof central incisors seriously compromises ideal func228Fig 3 Mutilated incisors of a Mahimba female from Namibia,incisai contact becomes impossibie after this cosmetic procédure.tion. This mutilation, or any similar cosmetic procedure producing occlusal disharmony, causes considerable masticatory dysfunction.On the other hand, esthetic PFM crowns on incisors can be used to ensure optimal anterior guidanceand group function, without interceptive occlusal contacts, have ideal omnifunctional gnathic excursions,and serve harmoniously within the dentition (Fig 4).Volume 30, Number 4,1999
Touyz et aiFig 4 Estiietic erawns m harmonious lunction. Form and (unctionare ideal.Fig 53 Discoiored maxiilary left central incisor, compiioating asuccessful retrograde root treatment.Fig 5b Maxillary ieft centrai incisor after permanent bleachingThe appearance has been enhanced withoul any further compromise in survival or function.Fig 6a Gingival asymmetry and permanent intrinsic discolorationof incisors. The appearance was unacceptabie to the patient.Fig 6b Cosmetic asymmetric porcelain iaminate veneers on theincisors The improvement in coior restored the patient's seifesteem, and the gingival asymmetry became unimportant.PRISTINE NATURAL STATEheight and staining of incisors may result in an unacceptable appearance (Fig 6a). Placement of porcelain laminate veneers, without an alteration in verticalheight of the incisors, can produce a pleasing appearance. Laminate veneers are piaced tnainly to improveappearance, but minor postcementation irritation ispossible un the facial gingival margin, despite wellfitting supragingival margins and acceptable emergence profiles of the veneers (Fig 6b). However, porcelain laminate veneers function well compared to resinRoot canal therapy can restilt in tooth discoiorations.For example, a maxillary left central incisor, discolored by a treated root canaL may not reflect the natural state of the dentition (Fig 5a). Recently, successfulesthetic bleaching has heen introduced to emulate thepristine natural state of teeth -* (Fig 5b).Asymtnetry and discoloration frequently representat! aberration. Discrepancies of symmetry in verticalOiiinlessence Internationai229
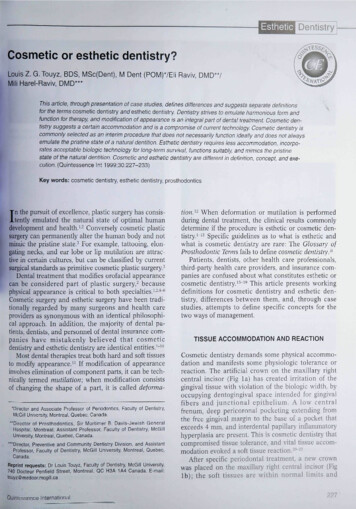
Touyz et aiFig 7 Cosmetic cowns on maxiliary incisors with chronic marginal intiammation. Ctironic gingivai irritation produces ttiis tiyperplastic reaction.Fig 9 Diamond inlaid into natural enamelot a maxiiiary canine Sociai values andpersonal desires dictate selections for cosmetic decorationFig 8 Cosmetic crowns on leetii with edematous marginal gingiva. Bieeding occurs with tiie slightest stimuius.Fig 10 Two briiiiant-out diamonds decorating the facia i surface ot maxiliary premolar gold crowns. The diamonds serve oniyas cosmetic enhancers.Fig 11 Round crystal in the incisor ot a removabie partialdenture. The entire cosmetic piosthesis is devised to enhance self-esteem.Fig 12 Gold dollar symbol on the maxiliary central incisor andgold distoincisai restoration on the ieft centrai inciser in a removable partiai denture. Tooth jewelry is intended to intiuence sociaiprestige.composite veneers, acrylic resin veneers, and crowns.In tbis case, cosmetic porcelain laminate veneers donot equal tbe pristine natural state of teetb and, witbout gingival modification, do not ensure the optimalsymmetry of supporting tissues.promote, or enhance bealth. Cosmetic PFM crownscan manifest subgingival impingement and compromiseorai healtb (Fig 7). Porceiain-fused-to-metal crowns frequently blanch gingival tissues, and the reacfion is followed by a chronic inflammatory adaptive response. " 'Tbe red edematous marginal gingiva and violafion ofthe biologic width ' resulfing from cosmetic crownscould cause the patient's oral health to deteriorate (Fig8). These inflatned tissues often bleed and progressfrom gingivitis to periodontitis.TISSUE HEALTHTbe major mission of health care providers is to sustain,230Volume 30. Number 4,1999
Touyz et ai11Fig 13 Complete-mouth cosrreiic resloratio.n Progressive solt(issue managemenl and ooniemporary restorative techniqueswere not usedFig 14 Comprehensive complete-moutin esihetio rehabilitation,integrat ng modern managemenl of both iiaid and soft tissuesDECORATIONprocedures, renders an esthetic dental treatment plan,without compromise of chosen techniques (Fig 14),Tooth decoration with unnatural artifacts is considered appealing in certain cultures. Extraneous dentaltlecorations can imply not only enhanced beauty butalso social wealth, status, and power. However, ametal-mounted diamond permanently inlaid to naturalenamel of a canine is not curative but is considered bydifferent ethnic groups as a cosmetic mode of treatment (Fig 9). Cosmetic decorating of restorations isnot always conducive to oral health. Two briOiant-cutdiamonds, placed in the facial surface of gold crowns,provide a good example (Fig 10),The insertion of cut crystai into removable partialdenttires (RPDs) or FPDs ser\'es visualiy as a cosmeticadjunct (Fig 11).Monetary symbols ( , t, , ) are occasionally cosmetically adapted on teeth to elevate social status oramusement. A gold dollar symbol positioned on themaxillary right central incisor and a gold distoincisalpseud ore sto ration affixed to a maxillary ieft central incisor are both cosmetic decorations when fitted in anRPD (Fig 12).COMPROMISED TECHNIQUESScientifically substantiated modem dentistry can providetreatment options that were previously only dreamed of.Selecting the confirmed optimal treatments dictates expectations and esthetic success. Various factors, such asskills, attitudes, and finances may influence decisions fortreatment plans. If patients are subjected to questionableprocedures, the approach is usually cosmetic, until replaced with superior doctimented treatment. For example, placement of an acrylic resin veneered crown that isnot in correct alignment and supported by inflamed softtissues is cosmetic therapy (Fig 13).Comprehensive oral rehabilitation, embracing endodontic, periodontic, orthodontic, and prosthodonticOuin (esse nee Internationa iDISCUSSIONCosmetic dentistry has existed for severai miilennia,and many relics from pritiiitive populations havedemonstrated dental rnutilation or decorative modification. ''' '' Esthetic dentistry certainly has its origin incosmetic dentistry, but, because of the refinements ofmodern treatments, these entities have evolved intotwo distinct directions and, therefore, should haveseparate definitions and approaches. Table 1 lists suggested criteria for differentiation between cosmeticdentistry and esthetic dentistry.The dentist shouid understand the differences between the concepts, execution, realization, and missions of esthetic and cosmetic dentistry. These concepts can infiuence the dentist's judgment as towhetber the planned procedures are esthetic or cosmetic. At this stage, the dentist should present thetreatment plan to the patient, explain the differencesbetween cosmetic and esthetic dentistry, and state hisor her wiilingness to perform an esthetic denial treatment plan. Occasionally, there may be a compromiseor hybrid therapy, but most treatments can be definedas cosmetic or esthetic if the provider and patient aremutualiy involved in treatment planning.Subjective vaiue systems of beauty impact on botbtypes of dentistry.'"'5 Consequently, making cosmeticdecisions may he perfectly desirable and estheticallyacceptable to some patients. Patients' opinions shouldbe included in decisions involving appearance-modifying procedures. Hasty, hedonistic procedures that areneither durable nor physiologic, aithough intended asesthetic, will be deemed cosmetic in tbe long run.Nevertheless, there are some overlapping areas common to both esthetic and cosmetic dentistry, such asappearance modification.231
Touyz el aiTABLE 1 Suggested factors for differentiating cosmetic and estheticdentistryFactorPhysical accommodation/toleranceSiiort-lerm ( interim/provision aLong-term (durabiiity)FunctionPristine stateHealthSuperfiuous decoralicnTectiniquesCtioice of materiaiOuaiity of materiaiMcdifies appearanceTtie rape uticCosmetic dentistryNet tolerated/unacceptableConsciousiy seiectedRareiy ctiosenNot idea iDoes not emuiateDoes not sustainDoes not eniianceDoes not promoteUsuaily providesCompromisedLeast irritating/ctieapestSecondary importanceYes/short termYes/short termNot selectedAlvjays chosenIdea iAlways emulatesSustainsEnhancesPromotesNever providesUncompromisedNonirritating/nol cheapPrimary importanceYes/long termYes/long termA dentist who prescribes a gold crown for anteriorteeth has adopted the decorative aspect from cosmeficdentistry and may dilute the esthetic value of treatment. This selection affects appearance, but a naturalappearing, ideally shaped PFM crown can be classifiedas estbetic denfistry. A plastic restoration, an arfificialcrown, and a resin composite facing are all cosmeUc iflong-term success is not evident. Limitations of treatment and patient cooperation force compromise, because cosmetic dentistry is less expensive, requiringless detailed manipulation than esthetic dentistry.Exposure of unsightly metal, as may occur on metalceramic crowns, distinguishes these as artificial and cosmetic, in spite of good bealtb and long-term survival.Alternative techniques, rendering a perfectly natural appearance in metal and ceramic of the replacementcrowns, would be regarded as esthefie. Esthefie dentistryinherently demands more detail and involves more expense because it is definitive, pristine, biologically stable,and periodontal-conscious dentistry. The ulfimate praefice of esthetic dentistry is preventive dentistry withpreservation of intact, natural, and attractive dentitions.Nevertbeless, cosmetic denfistry can be a valid therapeufic approach for the dentist. Cosmetic dentistry doesnot commonly survive long-term function and is characterized by ease of manipulation, but requires frequentreplacement. Social appearances, involving self-esteemand fear of evoking undesirable value-judgments, induce many patients to choose a rapid cosmetic result tosustain a desirable image in public, Tbe pinnacle of cosmetic dentistry has been "theatrical denfistry," when theonly requirement is appearance, regardless of long-termcomfort, funcfion, health, or expense.All dental procedures affecfing appearance can be232Esthetic denlislryTole rated/acceptableclassified as esthetic or cosmetic dentistry, and thedefinitive determinants are longevity, predictablehealth, and harmonious funcfion. Ideally, esthefie dentistry does not jeopardize appearance and should be indisfinguisbable from a natural appearance. Completedenture service that involves future modification can bedesignated, in certain instances, as cosmefic dentistry.Most prostheses that implement desirable modificatiotiscan be so classified. Maintenance of the natural dentition with optimal appearance, health, and functionshould be regarded as the best of esthetics. Guidance orexploitation of growth or opfimal heahng that includesorthodonfics and pcriodonfics to maintain oral healthwithout addifional degeneration is also considered tobe esthetic dentistry. ' Tooth-colored fissure sealantsare preventive and termed estbetic dentistry.CONCLUSIONCosmetic dentistry and esthetic dentistry should bedifferentiated and approached differently. The suggested working definitions could be the following:Cosmetic dentistry requires accommodation of oralphysiologic function and is primarily concerned withimmediate self-esteem, changes in color and shape,instant comfort, form, and appearance. Attentionto long-term well-being, reactions, and function issecondary.Esthetic dentistry is harmonious integrafion of oralphysiologic functions with equal emphasis on promoting pristine, ideal dentitions, through the restorafionof color, shape, form, and function, to ensure optimalhealth and durability.Volume 30, Number 4, 1999
Touyz el alACKNOWLEDGMENTSFigure 5 courtesy of Professtir J. F. van Reenen. Paíít Dean.University of Witwaiersrand, South Africa.REFERENCES1. Murray ]E. Annual discourse; Organ replacement and plastic surgery. N EngI ) Med 1972;287:1069-1074.2. Converse JM. Reconstructive Plastic Surgery: Principles andProcedures in Correction. Reconstruction and Transplantation, vol IV, ed 2, Philadelphia: Saunders. 1977.3. Brain R, The Decorated Body. London: Hutchison, 1979:16-81.4. Converse M. In: Kazanjian VH, Converse JM (eds). Current Surgical Treatment of Facial Injuries, od 3. Baltimore,MD: Williams and Wilkins, 1974.5. Vasconez LO, Morris WJ, Owsley JQ, Alpert BS. In:Surgical Diagnosis and Treatment. Dunphy E, Way LW(eds). Plastic Surgery, ed 5. Los Altos. CA: Langer MedicalPublications. 19Sl:947-975.6. Rees T, Wood-Smith D. Cosmetic-Facial Surgery, ed 2. Philadelphia: Saunders, 1980.7. Philips DS. Incorporating cosmetic dentistry into a generalpractice. J Can Dent Assoc 1994:60:682-686.8. Carrick JL Cosmetic dentistry and implant prosthetics. CurrOpin Cosmet Dent 1994:93-989. Singer BA. Principles of esthetics [review]. Curr Opin Cosmet Dent 1994:6-12.10. Austin CJ. Marketing strategies for the cosmetic practice.Curr Opin Cosmet Dent 1994:123-133.11. Andrews P. Levine N, Milnes A, Pulver F, Sigal M, Titley K.Advances in the treatment of acquired and developmentaldefects of hard dental tissues [reviewj. Curr Opin CosmetDentl992;2:66-7112 Sturtevant WC. Mutilations and deformations. In: BentonW(ed). Encyclopedia Britannica. Chicago: W. Benton, 1970:1106-110713. de Kloet HJ. Davidson CL. Dental ethics, esthetics and cosmetics. Ned Tijdschr Tandheelkd 1991;98:198-202 (inDutch).Quintessence International14. Academy of Prosthodontics. Glossary of ProsthodonticTerms, ed 6. J Prosthet Dent 1994;71:43-94.15. Feiler K. "Cosmetic" dentistry {what's in a word?). J AmAcad Cosmet Dent 1992;7(3):13-16.16. Burgersdijk R, Truin GJ, Kalsbeek H, van't Hof M, Mulder ].Ohjective and subjective need for cosmetic dentistry in theDutch adult population. Community Dent Oral Epidemiol1991;19:61-63.17 Austin C. Is cosmetic dentistry for you? Dent Today 1990;9(2):29-31.18. Jackson R. An esthetic inlay/onlay technique using "totaletch". Pract Periodont Esthet Dent 1990;2í3):26-29.19. Austin CJ. Informing your patients about cosmetic dentistry.Dent Manage 1990;30(3):42-44,46,48.20. Pruthi VK. Surgical crown lengthening in periodontics.J Can Dent Assoc 19S7;12:911-915.21. Richter WA, Lieno H Relationship of crown margin placement to gingival inflammation. J Prosthet Dent 1973;30:156-161.22. Ingher ], Rose LF and Costlet JG. The biologic width-Aconcept in periodontics attd restorative dentistry. AlphaOmega 1977;7:62-65.23. Van Reenen JP. In: Singer R, Lundy JK (eds). Variation,Culture and Evolution in African Populations: FestsschriftPapers in Honour of Dr. Hertha de Villiers, No. 12, Toothmutilating and extraction practises amongst the peoples ofSouth West Africa (Namibia). Johannesburg, South Africa:Witwatersrand University Press, 1986:159-161.24. Mountouris G, Mantzavinos 2, Michou H. Discolorations:A new method of bleaching discoloured vital teeth (preliminary study) in Greek]. Odontostomatol Proodos 1990;44:195-206.25. Donaldson D. Gingival recession associated with temporarycrowns. J Periodontoi 1973 ;44:691-696.26. Lentz DL. Cosmetic dentistry among the ancient Maya.Miss Dent Assoc J 1990;46(3):2527 Cohen ES. Atlas of Cosmetic and ReconstructivePeriodontal Surgery, ed 2. Philadelphia: Lea & Febiger,1994.233
State of the naturai dentition. Cosmetic and esthetic dentistry are different in definition, concept, and exe-cution. (Quintessence Int 1999;30:227-233) Key words: cosmetic dentistry, esthetic dentistry, proslhodontics In the pursuit of excellence, plastic surgery has consis-tently emulated the natural state of optimal human development and .