Transcription
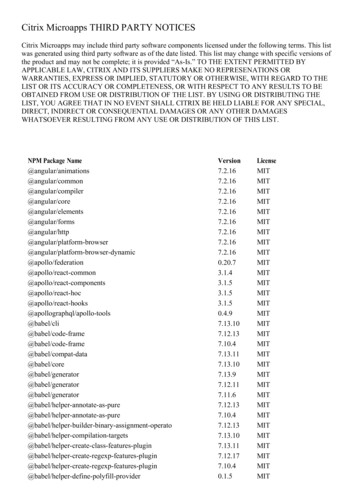
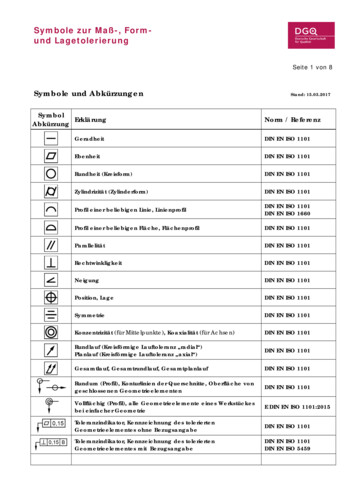
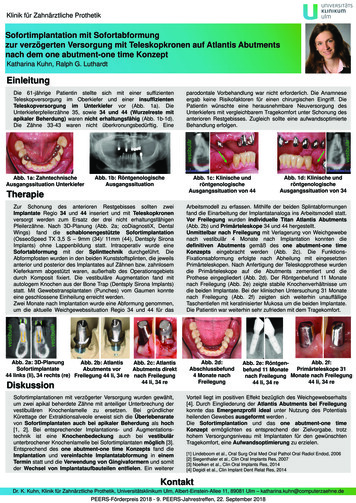
Klinik für Zahnärztliche ProthetikSofortimplantation mit Sofortabformungzur verzögerten Versorgung mit Teleskopkronen auf Atlantis Abutmentsnach dem one abutment-one time KonzeptKatharina Kuhn, Ralph G. LuthardtEinleitungparodontale Vorbehandlung war nicht erforderlich. Die Anamneseergab keine Risikofaktoren für einen chirurgischen Eingriff. DiePatientin wünschte eine herausnehmbare Neuversorgung desUnterkiefers mit vergleichbarem Tragekomfort unter Schonung desanterioren Restgebisses. Zugleich sollte eine aufwandsoptimierteBehandlung erfolgen.Abb. 1a: ZahntechnischeAusgangssituation UnterkieferAbb. 1b: RöntgenologischeAusgangssituationTherapieAbb. 1c: Klinische undröntgenologischeAusgangssituation von 44Abb. 1d: Klinische undröntgenologischeAusgangssituation von 34Arbeitsmodell zu erfassen. Mithilfe der beiden Splintabformungenfand die Einarbeitung der Implantatanaloga ins Arbeitsmodell statt.Vor Freilegung wurden individuelle Titan Atlantis Abutments(Abb. 2b) und Primärteleskope 34 und 44 hergestellt.Unmittelbar nach Freilegung mit Verlagerung von Weichgewebenach vestibulär 4 Monate nach Implantation konnten diedefinitiven Abutments gemäß des one abutment-one timeKonzepts eingebracht werden (Abb. 2c). Die FunktionsFixationsabformung erfolgte nach Abheilung mit eingesetztenPrimärteleskopen. Nach Anfertigung der Teleskopprothese wurdendie Primärteleskope auf die Abutments zementiert und dieProthese eingegliedert (Abb. 2d). Der Röntgenbefund 11 Monatenach Freilegung (Abb. 2e) zeigte stabile Knochenverhältnisse umdie beiden Implantate. Bei der klinischen Untersuchung 31 Monatenach Freilegung (Abb. 2f) zeigten sich weiterhin unauffälligeTaschentiefen mit keratinisierter Mukosa um die beiden Implantate.Die Patientin war weiterhin sehr zufrieden mit dem Tragekomfort.vestibulärvestibulärZur Schonung des anterioren Restgebisses sollten zweiImplantate Regio 34 und 44 inseriert und mit Teleskopkronenversorgt werden zum Ersatz der drei nicht erhaltungsfähigenPfeilerzähne. Nach 3D-Planung (Abb. 2a; coDiagnostiX, DentalWings) fand die schablonengestützte Sofortimplantation(OsseoSpeed TX 3,5 S – 9mm (34)/ 11mm (44), Dentsply SironaImplants) ohne Lappenbildung statt. Intraoperativ wurde eineSofortabformung mit der Splinttechnik durchgeführt. DieAbformpfosten wurden in den beiden Kunststoffsplinten, die jeweilsanterior und posterior des Implantates auf Zähnen bzw. zahnlosemKieferkamm abgestützt waren, außerhalb des Operationsgebietsdurch Komposit fixiert. Die vestibuläre Augmentation fand mitautologem Knochen aus der Bone Trap (Dentsply Sirona Implants)statt. Mit Gewebstransplantaten (Punches) vom Gaumen konnteeine geschlossene Einheilung erreicht werden.Zwei Monate nach Implantation wurde eine Abformung genommen,um die aktuelle Weichgewebssituation Regio 34 und 44 für dasvestibulärvestibulärDie 61-jährige Patientin stellte sich mit einer suffizientenTeleskopversorgung im Oberkiefer und einer insuffizientenTeleskopversorgung im Unterkiefer vor (Abb. 1a). DieUnterkieferpfeilerzähne 35, sowie 34 und 44 (Wurzelreste mitapikaler Beherdung) waren nicht erhaltungsfähig (Abb. 1b-1d).Die Zähne 33-43 waren nicht überkronungsbedürftig. EineAbb. 2a: 3D-PlanungAbb. 2b: AtlantisAbb. 2c: AtlantisSofortimplantateAbutments vorAbutments direkt44 links (li), 34 rechts (re) Freilegung 44 li, 34 re nach Freilegung44 li, 34 reDiskussionSofortimplantationen mit verzögerter Versorgung wurden gewählt,um zwei apikal beherdete Zähne mit anteiliger Unterbrechung dervestibulären Knochenlamelle zu ersetzen. Bei gründlicherKürettage der Extraktionsalveole erweist sich die Überlebensratevon Sofortimplantaten auch bei apikaler Beherdung als hoch[1, 2]. Bei entsprechender Implantations- und Augmentationstechnik ist eine Knochenbedeckung auch bei vestibulärunterbrochener Knochenlamelle bei Sofortimplantaten möglich [3].Entsprechend des one abutment-one time Konzepts fand dieImplantation und vereinfachte Implantatabformung in einemTermin statt und die Verwendung von Gingivaformern und somitder Wechsel von Implantataufbauteilen entfielen. Ein weitererAbb. 2d:Abschlussbefund4 Monate nachFreilegungAbb. 2f:Abb. 2e: RöntgenPrimärteleskope 31befund 11 Monatenach Freilegung Monate nach Freilegung44 li, 34 re44 li, 34 reVorteil liegt im positiven Effekt bezüglich des Weichgewebserhalts[4]. Durch Eingliederung der Atlantis Abutments bei Freilegungkonnte das Emergenzprofil ideal unter Nutzung des Potentialsheilenden Gewebes ausgeformt werden .Die Sofortimplantation und das one abutment-one timeKonzept ermöglichten es entsprechend der Zielvorgabe, trotzhohem Versorgungsniveau mit Implantaten für den gewünschtenTragekomfort, eine Aufwandsoptimierung zu erzielen.[1] Lindeboom et al., Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2006[2] Siegenthaler et al., Clin Oral Implants Res, 2007[3] Noelken et al., Clin Oral Implants Res, 2014[4] Degidi et al., Clin Implant Dent Relat Res, 2014KontaktDr. K. Kuhn, Klinik für Zahnärztliche Prothetik, Universitätsklinikum Ulm, Albert-Einstein-Allee 11, 89081 Ulm – katharina.kuhn@computerzaehne.dePEERS-Förderpreis 2018 - 9. PEERS-Jahrestreffen, 22. September 2018
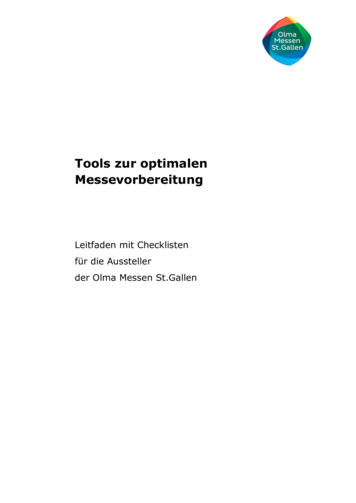
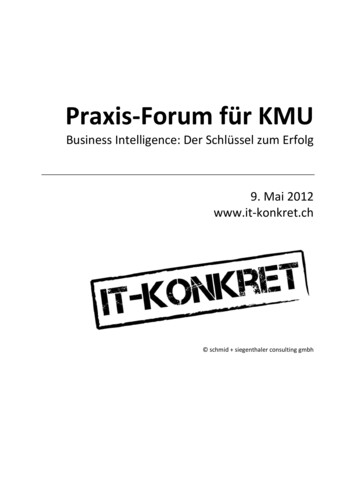
Rehabilitation of two patients with individual Abutments– case report –Research & Reviews: Journal of Dental Sciences Volume 5 Issue 2 March, 2017Ali-Reza Ketabi 1 , Dr med dent, Sandra Ketabi 1, Dr med, Dr med dent,Hans-Christoph Lauer 2 , Professor, Dr med dent and Silvia Brandt 2, Dr med dent1Private Practice, Stuttgart, Germany2 Dept. of Prosthodontics, J.W. Goethe University, Frankfurt, GermanyRadiologic parameters:In order to obtain an optimal treatment result in the context of a comprehensive supply ofimplant-supported dental prosthesis, several factors must be considered. While survivalrates of enossal titanium implants are no longer a relevant problem [1-4], the aestheticrequirements of patients have risen further in recent years. This applies not only to the socalled "white aesthetics", which can be optimally solved using modern veneering or fullceramic systems, but also to the so-called "red aesthetics", which is determined by thehealth and contour of the gingival tissue. In addition to its function, aesthetics is an essentialsuccess criterion, which must be foreseeable to be solved by the implant dentist. Amongother things, we discuss the extent to which long-term results can be achieved by stableimplant-abutment connections and corresponding peri-implant hard and soft tissuetechniques. A further very important aspect is the design of the emergence profile [5-7].Thedesign of the transition from the round implant cross-section to the tooth-root-like individualthrough-flow profile is achieved by the abutment, which must be adapted asrequired.Corresponding individual profiles have been produced in the past by casting onpreformed abutments, which is, of course, very time-consuming and cost-intensive. A furtherpossibility for the production of individual abutments consists in the use of CAD / CADabutments (eg Atlantis VAD , DENTSPLY IH GmbH), a method for making individualabutments from the ideal shape of the crown.Panoramic radiographies were performed on behalf of pre-implantological diagnosis beforeimplant treatment with the Orthophos D 3297 (Sirona Dental Systems GmbH). Conventional xrays were taken in parallel technique at three different points in time, using the Sirona SR60/70/7L tube. The first x-ray was taken immediately after implant placement in order to controlthe insertion-success. The second radiologic examination was performed at the time of the onsetof the final prosthetic restauration (Baseline). The third x-ray was taken one year after functionalloading of the implant (Figure 11-14).Cases and Methods:An individual design of the emergence profile is necessary for the success of an implantprosthetic treatment [5-7]. Individual emergence profiles have been made in the past by castingon prefabricated abutments, which is of course very time-consuming and cost-intensive. Inaddition, there is a risk that exposure to dark metal particles will occur during gingival recessions.In order to avoid aesthetic disadvantages, the abutment can be veneered with ceramics in thebuccal area, but remaining oxide layers or porosities in the ceramic can lead to irritation of theperi-implant gingiva [8] (Figure 8). For a number of years, the possibility to make individualabutments for a wide variety of implants is available with various CAD/CAM procedures (in thiscase, Atlantis VAD , DENTSPLY IH GmbH). The method allows the production of individualabutments from different materials, starting from the ideal shape of the crown. Thus, theemergence profile can be optimized by the abutment.CAD/CAM-Systems for the fabrication of individual abutments facilitate the customizedproduction of aesthetically formed abutments, made of different materials, like titanium, withtitanium nitride anodized titanium, also designated as gold-hue titanium, or zirconia [9-15].Implant abutments generated by CAD/CAM-technology are more precise than those created byconventional casting and fit more precisely than stock abutments [16]. A radiographic andScanning Electron Microscopy assessment revealed no differences between customized andprefabricated titanium-abutments of the DENTSPLY IH GmbH with respect to the microscopicand radiographic fit at the implant-abutment interface [17]. Individually designed Atlantisabutments (DENTSPLY IH GmbH) are available for all major implant systems, including the AstraTech Implant System. Besides the low-cost aspects of Atlantis [11, 18], there are notable benefitsas a reduced patient treatment time [11, 19-20] and a simplified treatment protocol [11, 18].In this case report, the supply of two patients with individual abutments by two different methodsis presented. In Case 1 a prefabricated zirconium abutment was individualized with ceramics inthe cervical area, while in case 2 the abutment was CAD-designed and CAM- fabricated. Notechnical complications in terms of fractures of the veneering material or abutment fracture orloosening of the abutment could be observed. In both cases an increase of the papilla could beobserved (Figure 8, 10) after one year. During the observation period soft tissue-complication,concerning a red coloring of the mucosa around the abutment, was observed only in Case 1(Figure 8) without any radiological consequence for hard-tissue. No bone changes, on the mesialand distal aspect of the implants could be found after one year in both cases (Figure 12, 14). Theaesthetic result was estimated as very good by both patients.Clinical and radiological examinations were performed in both patients before implanted. Afterdetailed consultation, an Astra Tech Osseospeed Implant (DENTSPLY IH GmbH) was insertedin each patient. After a healing period of 2 months the patients were provided with cementedcrowns, made of veneered zirconia Ceramill ZI (Amann Girrbach GmbH). An impression copingwas placed, and a transfer impression was made. The abutments were prepared by differentmethods as follows.Case 1. A soft tissue model was made from the impression, and the desired gingival tissueFigure 1-3was carved into the model. The tissue contour of the adjacent incisor was used as a gide tocreate the new emergence profile. A prefabricated zirconium abutment (DENTSPLY IH GmbH)was modified in the cervical area to create a custom abutment with natural gingival contour(Figure 1). The abutment was veneered with Ceramill ZI (Amann Girrbach GmbH) and placedon the working model to fabricate a crown (Figure 2-3).Figure 1: Die master and abutment withindividual emergence profile.Figure 2: By Ceramill ZI veneeredprefabricated abutment.Figure 3: Die master and crowns.Case 2. The Abutment was fabricated using the Atlantis Virtual Abutment Design-Software(VAD) (DENTSPLY IH GmbH). Depending on the individual anatomic situation, the systemcomprises different options for a customized design of the abutments emergence profile. Itfurther offers the possibility to compensate the position of prosthetically not ideal placedimplants through different angulation options for the abutments. The basis for the millingprocess, performed by the manufacturer with the VAD-software, was a 3D-Scan of a plastercasted model with a gingival mask made of silicon (Picodent Dental-Produktions VertriebsGmbH) and Wax-up around the duplicate abutments in the respective implant region (Figure 4).The technician himself determined the required abutment design, by transcribing theinstructions firstly in a special virtual entry form, and sending the data subsequently via internetto the manufacturer. After the milling process, the finished abutment, made of zirconia, wasdelivered to the technician with a corresponding abutment screw (Figure 5). After that, theabutment was placed on the model and the final prosthetic restauration was manufactured bythe dental technician (Figure 6).Figure 11: X-ray control afterplacement of abutmentsand crown.Figure 12: X-ray control after 1year.Figure 13: X-ray control afterplacement of Atlantis abutmentsand crown.Figure 14: X-ray control after 1year.Figure 11-14Introduction:Discussion:Conclusion:Abutments serve as an important link between implants and the prosthetic superstructure. Theyare also a very important determinant for biological, technical, and aesthetic parameters. Theproduction of individual abutments using prefabricated pieces is often difficult and costly. With theCAD/CAM method abutments are designed starting from the ideal shape of the individual crown.This saves time and therefore costs. Individual CAD/CAM-fabricated abutments are a good and apredictable treatment option, and lead to a high patient satisfaction concerning therapeutic andaesthetic results.Figure 4-6Literature:Figure 4: 3D-Scan of a plaster casted modelwith a gingival mask.Figure 5: Die master and zirconia Atlantisabutment with individual emergence profile.Figure 6: Zirconia Atlantis abutment and crown.Clinical parameters:Figure 7-10Soft tissue conditions and state of the prosthetic restauration were recorded on baselineand after one year of function (Figure 7-10). Soft tissue quality was determined by theparameters mesial and distal height of the papilla and coloration of the mucosa. Changesin papilla height were compared visually by photographs, taken at baseline and on thefollow up examination. Changes of the papilla soft tissue level were documented.Figure 7: Clinical state after placement Figure 8: Clinical state after one year.of abutment and crown.Figure 9: Clinical state after placement Figure10: Clinical state after one year.of Atlantis abutment and crown.1. Cooper LF, Ellner S, Moriarty J, Felton DA, Paquette D, et al. (2007) Three-year evaluation of single-tooth implants restored 3 weeks after 1-stagesurgery. Int J Oral Maxillofac Implants 22(5):791-800. [PubMed - indexed for MEDLINE]2. Den Hartog L, Slater JJ, Vissink A, Meijer HJ, Raghoebar GM (2008) Treatment outcome of immediate, early and conventional single-tooth implants inthe aesthetic zone: a systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J Clin Periodontol 35(12):1073-86. [PubMed- indexed for MEDLINE]3. Lang NP, Pietrusson BE, Tan K, Brägger U, Egger M, Zwahlen M (2004) A systematic review of the survival and complication rates of fixed partialdentures (FPDs) after an observation period of at least 5 years. II. Combined tooth-implant-supported FPDs. Clin Oral Implants Res 15 (6): 643-53.[PubMed - indexed for MEDLINE]4. Zurdo J, Romao C, Wennström JL (2009) Survival and complication rates of implant-supported fixed partial dentures with cantilevers: a systematicreview. Clin Oral Implants Res 20 (4): 59-66. [PubMed - indexed for MEDLINE]5. Al-Harbi SA, Edgin WA (2007) Preservation of soft tissue contours with immediate screw-retained provisional implant crown. J Prosthet Dent 98 (4):329-32. [PubMed - indexed for MEDLINE]6. King KO (1996) Implant abutment emergence profile: key to esthetics. J Oral Implantol 22 (1): 27-30. [PubMed - indexed for MEDLINE]7. Panaite D, Klokkevold P, Charles A (2008) Peri-implant papilla: realities on papilla preservation and reformation. J Calif Dent Assoc 36 (11): 851-67.[Sacramento Ca : California Dental Association]8. Abrahamsson I, Berglundh T, Glantz PO, Lindhe J (1998) The ucosal attachment at different abutments. An experimental study in dogs. J ClinPeriodontol 25 (9): 721-27. [PubMed - indexed for MEDLINE]9. Ganz SD (2003) Computer-milled patient-specific abutments: incredibly quality with unprecedented simplicity. Implantology 37-44. [Google Scholar]10. Ganz SD (2003) Use of stereolithographic models as diagnostic and restorative aids for predictable immediate loading of implants. Practicalprocedures & aesthetic dentistry 15:763-71; quiz 772. [PubMed - indexed for MEDLINE]11. Ganz SD (2005) Finally, a ‘win-win’ solution: Increasing accuracy while saving time, money with computermilled abutments. Dental Economics[Google Scholar]12. Ganz SD (2007) CT-derived model-based surgery for immediate loading of maxillary anterior implants. Practical procedures & aesthetic dentistry19:311-8; quiz 320, 302. [PubMed - indexed for MEDLINE]13. Ganz SD (2008) Defining new paradigms for assessment of implant receptor sites. The use of CT/CBCT and interactive virtual treatment planning forcongenitally missing lateral incisors. Compendium of continuing education in dentistry 29:256-8, 260-2, 264-7; quiz 268, 278. [PubMed - indexed forMEDLINE]14. Schneider A, Kurtzman GM (2001) Computerized milled solid implant abutments utilized at second stage surgery. General dentistry 49:416-20.[PubMed - indexed for MEDLINE]15. Watkin A, Kerstein RB (2008) Improving darkened anterior peri-implant tissue color with zirconia custom implant abutments. Compendium ofcontinuing education in dentistry 29:238-40, 42. [PubMed - indexed for MEDLINE]16. Priest G (2005) Virtual-designed and computer-milled implant abutments. Journal of oral and maxillofacial surgery 63:22-32. [PubMed - indexed forMEDLINE]17. Apicella D, Veltri M, Chieffi N, Polimeni A, Giovannetti A, et al. (2010) Implant adaptation of stock abutments versus CAD/CAM abutments: aradiographic and Scanning Electron Microscopy study. Annali di stomatologia 1:9-13. [PubMed]18. Garg AK (2002) The Atlantis Components Abutment: simplifying the tooth implant procedure. Dental Implantology Update 13:65-70. [PubMed indexed for MEDLINE]19. Adams MW (2005) Computer-designed and milled patient-specific implant abutments. Dentistry today 24: 80-3. [PubMed - indexed for MEDLINE]20. Osorio J (2000) Use of the Atlantis Abutment in restorative practice speeds time to function and aesthetics. [Interview]. Dental Implantology Update11:57-62. [PubMed - indexed for MEDLINE]
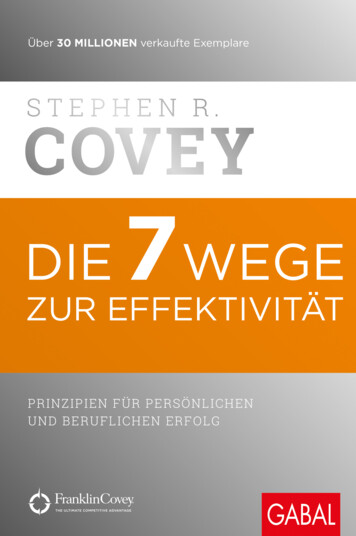
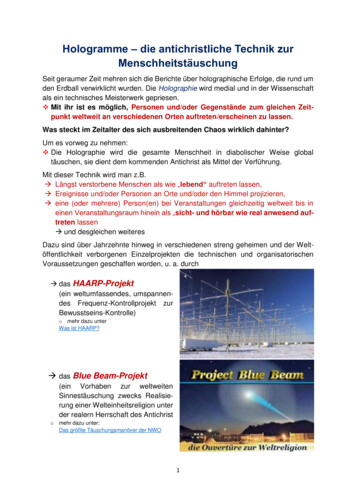
Mund-, Kiefer- undGesichtschirurgische KlinikDirektor: Prof. Dr. Dr. M. KestingUniversitätsklinikumErlangenImplantation im Frontzahnbereich des Oberkiefers undWeichgewebschirurgie nach TraumaM Buchbender,Mund-, Kiefer- und Gesichtschirurgische Klinik, Universitätsklinikum der FAU Erlangen-NürnbergEinleitungEin 28-jähriger Patient stellte sich mit einer Einzelzahnlücke in regio 21 in der Ambulanz der Mund-, Kiefer- undGesichtschirurgischen Klinik Erlangen vor. Der Zahn ging traumatisch 08/16 verloren, die Zähne 11 und 12 konntenbei lateraler Luxation und folgender endodontischer Behandlung erhalten werden, Anamnestisch sonstunauffällig, parodontal stabil (PSI 0) bei guter Mundhygiene (API/SBI 25%) und einem hohen ästhetischenAnspruch. Nach Beratung wurde die Implantation ohne geführte Bohrschablone geplant.Präoperative SituationRöntgenologischerBefund 05/17Intra/Postoperative SituationKlinischerBefund 05/17Nobel Active 4,3mmx13mm, 05/17OPG postimplantationem 05/17Im Rahmen der Implantatfreilegung wurde aufgrund des klinisch transversal schmal erscheinendemGingivaverlaufs, bei ausreichend vorhandener keratinisierter und befestigter Gingiva , zur Verdickung mittels einesautologen Bindegewebstransplantates vom Gaumen inisch erBefund 08/17Postoperative Situation nach FreilegungHealing H:5 mm, EntnahmeBindegewebe Gaumen rechts,Mukosalappen regio 21tunneliert Vicryl 6/0 und Vicryl5/0 08/17Postoperative Situation 10/17Einzelzahnaufnahme 08/17Healing H: 5mmEingliederung der definitiven Arbeit 06/18Material:MetallkeramikDiskussionDer Patient ist mit dem Ergebnis sehr zufrieden. Die erwartete Schrumpfung des autologen Transplantates istauch nach prothetischer Versorgung nicht eingetreten. So zeigt das periimplantäre Weichgewebe funktionellsowie ästhetisch beste Voraussetzungen für eine gute Langzeitstabilität.Universitätsklinikum ErlangenMund-, Kiefer- und Gesichtschirurgische KlinikDirektor: Prof. Dr. Dr. M. KestingMayte BuchbenderGlückstrasse 1191054 ErlangenEmail: mayte.buchbender@uk-erlangen.de
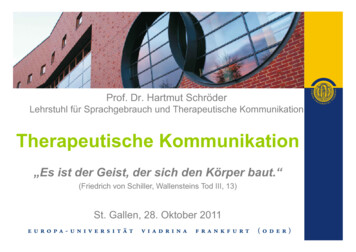
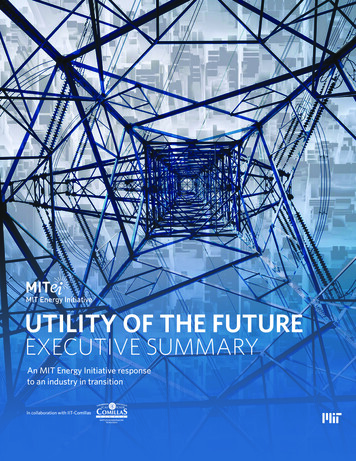
Immediate implant placement and timely provisionalization withchairside customized PEEK abutmentsAhlskog L, Messner H, Lüdke EPraxengemeinschaft Dr. K., H., und L. Ahlskog, TuttlingenIntroductionA flapless approach and the immediate reconstruction of the emergence profile is recommended to improve soft tissue esthetics and function of dentalimplants [1]. The time and effort to produce a temporary immediate reconstruction is generally viewed as fairly high.Material and methodsAfter failed, alio loco performed, multiple endodontic treatment a patients tooth22 had to be removed due to persisting pain. Following atraumatic removalof the tooth an immediate implant (OsseoSpeed EV 3,6 mm) was inserted.The remaining bony buccal gap was augmented with autogenous bone fromthe posterior region of the lower jaw, a further connective tissue graft was tobe avoided by request of the patient. The ideal prosthodontic support forthe soft tissues during healing was to be achieved by a chairside producedtemporary reconstruction through customizing a labside prepared TempDesign EV and adding composite over a mould. Finishing of the restorationcan be carried out in the Dental Laboratory. Professional prophylaxis beforesurgery, tooth extraction, immediate implant placement, gapfill and provisionalization was achieved in 4 hours. After 8 weeks an impression was takenfor the design of an Atlantis abutment and the fabrication of an all ceramiccrown. To optimized the regenerative potential of the stable surrounding softtissues through broadening their base, the shape of the final abutment wasshifted from convex to concave.Conclusions- Timely provisionalization can easily be achieved through customizing TempDesign EV- Semiindividual PEEK abutments for quicker lab- and chairside adjustments desirable- Further reduction of treatment time possible, under 3 hours can be achieved- CAD/CAM processing of TempDesign EV desirable- Identically shaped impression- and scanpost or even final abutments e.g. with Cerec possible- Final shape defined during healing, though changes can be implied at any stage (Fig. 4c)- Shifting the emergence profile can support further regeneration of the periimplant soft tissues (Fig. 4b-e)Fig. 1: Customized TempDesign EVFig. 2a-e, a: Via falsa on tooth 22, b: Before removal of tooth 22, thin gingival biotype c: Customizing a TempDesign EV for ideal support of the soft tissue at insertion,d: Immediate reconstruction after 4h, e: After 8 weeks of healing.Fig. 4a-e, a: Preservation of the buccal plate after 8 weeks, b: Emergence profile after 8 weeks, c: Shift in emergence profile from convex to concave to broaden the base of thepreserved papillas, d: All ceramic fixed restoration one week after incorporation, e: Regenerated papillas after 1 year.Fig. 3: Palatal positioningof the implant.Fig. 5: Healthy soft tissue after16 weeks.Fig. 6a-d, a: Before extraction of tooth 22, pronounced scalloping of the gingiva, b: Temporary reconstruction after 8 weeks, c: All ceramic crown after 16 weeks, further regeneration of the papillas desirable toreduce the width of the restoration cervically, d: Esthetic restoration surrounded by stable and healthy looking periimlant mucosa after 1 year.Literature[1] Noelken R, Moergel M, Kunkel M, Wagner W. Immediate and flapless implant insertion and provisionalization using autogenous bone grafts in the esthetic zone:5-year results. Clin Oral Implants Res. 2018 Mar;29(3):320-327.ContactPraxis für Zahnheilkunde Lars Ahlskog, Möhringerstr. 77, 78532 Tuttlingen Germany, e-mail: lars.ahlskog@ahlskog.deA H L S K O G
Eine PEEK-Brücke auf vier Zirkonoxidteleskopen imzahnlosen Unterkiefer – eine FallvorstellungDres. Michael Schupp und Fabian Schäffer, Fachärzte für MKG-Chirurgie, FreiburgZTM Reinhard Sroka, Petersen Dental, RheinfeldenEinleitungIn der Zahnheilkunde rückt der ältere Patient umso mehr in den Vordergrund, je älter die Bevölkerung wird. In dieser Patientengruppe ist die Reinigbarkeit und das Handling von Zahnersatz oft schwierig und so bedarf es angepasster implantologischerKonzepte für diese Altersgruppe.Ziel der gezeigten Versorgung ist es, einem in seinem Pflegebemühen wegen seiner Parkinsonerkrankung eingeschränktenPatienten durch „fest-sitzende“ Zähne mit wenig Aufwand ein hohes Maß an Lebensqualität zurückzugeben.Patient 84. Lj. NichtraucherPlanung und VerlaufZahntechnik Petersen DentalSeit 2009 Parkinson, Behandlung mit L-DopaVier interforaminale camlog-Implantate.Ursprünglich zur Sofortversorgung geplant.04.04.2016 Implantation mit intraoperativer Abformung,offen mit Impregum und individuellem Löffel.26.04.2016 Wachsanprobe09.06.2016 erneute Abformung, Grund: postoperativbeim Eindrehen eines GF Torsion möglich.14.07.2016 Einsetzen der ArbeitNano Zirkon von Panasonic für die Teleskope,Fräsung als Grünling und Sinterung.Peek-Optima LT1 Polymer Juvora-Dentalscheibezur Fräsung des Peek-GrundgerüstesBredent rohpak als rosa Opaker undBredent visio.link als Haftvermittler zum PMMAZähne Vita, KunststoffDatenverarbeitung mit 3Shape Exocat-SoftwareAbb. 1: ProfilansichtAbb. 2: Postoperatives Bild mit Gingivaformer (GF)Abb. 3: PEEK-Brücke von basal gesehenAbb. 4: Zirkonteleskope in situAbb. 5: Kontrollbild 19.04.2017Abb. 6: PEEK-Brücke in situAbb. 7: Kontrolle 03.05.2018 o.B.Abb. 8: Kontrollbilder 03.05.2018Abb. 9: Zahnstein an der KunststoffbrückeVorhofflimmern mit Xarelto-EinnahmeHerbst 2015 Verlust der letzten Zähne im UKNeue Prothese der HZÄ mit mangelndemHalt und Verschiebung der Kieferrelation.Ergebnisse und DiskussionDie Untersuchungsergebnisse von Tetsch und Schiefner aus dem Jahre 1986 konnten zeigen, daß reines Titan als Werkstoff imKnochen (Osseointegration) und Keramik im Durchtritt durch die Schleimhaut und in der Mundhöhle (Sauberkeit) optimal sind.Bei Wirthmann und Paulmann wurde die außergewöhnliche Verbindung von Titan und Knochen auf die Bildung von Perowskit(CaTiO3) zurückgeführt (2014), was auch in heutiger Zeit die von Tetsch seinerzeit aufgestellte Forderung unterstreicht.Bei Hochbetagten ist die oberste Prämisse einer Implantattherapie der Erhalt der Hygienefähigkeit. Overdentures bieten imzahnlosen Kiefer klare Vorteile gegenüber festsitzenden Brücken, am besten mit unverblockten Attachements (Schimmel 2016).Schnutenhaus hat hierfür die dann auch von uns verwendete metallfreie Doppelkronentechnik beschrieben (2015).Unser Patient berichtet über die gezeigte abnehmbare PEEK-Brücke, daß sie sich im Gegensatz zu der früher getragenenModellgußprothese durch Ihre Leichtigkeit und durch ihren festen Sitz wie seine festen Zähne anfühlt. Die Reinigung derKeramikpfeiler, die per se Plaque-abweisend sind, gelingt auch dem Patienten mit eingeschränktem Bewegungsmuster gut –lediglich die Kunststoffbrücke muß regelmäßig gereinigt und poliert werden. Letztlich ist bei unserem Patienten die Akzeptanzauch wegen der zahnfarbenen Pfeiler sehr hoch – auch ohne Brücke hat er wieder „Zähne“.SCHIMMEL, M., F. MÜLLER, V.G.A. SUTER und D. BUSER, Implantatversorgung bei Hochbetagten. Implantologie 24 (4): 355-365 (2016)SCHNUTENHAUS, S., C. SCHREIBER und D. WIRTHMÜLLER, Doppelkronentechnik: Metallfrei gelöst. Zahntech Mag 19,2: 111-122 (2015)TETSCH, P. und U. SCHIEFNER, Untersuchung zur parodontalen Situation bei Titan- und Keramikimplantaten. Z. Zahnärztl. Implantol. II: 18-21 (1986)WIRTHMANN, A.J.A. und C. PAULMANN, Wechselwirkung von Knochen und Titan – Neue Einblicke. Z. Zahnärztl. Implantol. 30: 288-300 (2014)
Dr. K. Kuhn, Klinik für Zahnärztliche Prothetik, Universitätsklinikum Ulm, Albert-Einstein-Allee 11, 89081 Ulm -katharina.kuhn@computerzaehne.de . implant-supported dental prosthesis, several factors must be considered. While survival . 18. Garg AK (2002) The Atlantis Components Abutment: simplifying the tooth implant procedure. Dental .