Transcription
Risk Stratification;a Calculated approach to care
Learning Objectives:Participation in this workshop will enable you to: Describe how other clinics are implementing riskstratification models. Explore benefits and considerations whenimplementing risk stratification. Collaboratively develop a proposal to pilot in aclinic or department.
1:00 Welcome and Overview1:10 Getting AcquaintedAGENDA:1:30 Panel Presentations2:30 Break2:45 Questions for the Panel3:15 Networking/Putting It Into Practice4:15 Wrap Up and Key Learnings4:30 Adjourn
Getting Acquainted
Panel Presentations
Risk Stratification: An Innovative Approach toCare ManagementJill Swenson, BSN, RN, CCMMelissa Hurt, BSN, RN2019 MDH Learning Days Conference
MDH Health Care Home Certified Health Care Home Clinics– 21 North Region– 20 South Region– Combine regions in April 2019 12 Large Metro Clinics 29 Small Regional Clinics
Risk Stratification Risk Stratification is defined as a ongoing process of assigningall patients in a practice a particular risk status – risk status isbased on data reflecting vital health indicators, lifestyle andmedical history of your adult or pediatric populations.Stratifying risk helps to :– Address specific population management challenges– Match risk with levels of care– Individualize treatment plans to lower risk and improvefunction– Align the practice with value-based care approaches
What is the aim of RiskStratification Identify patients who are most likely tobenefit from care management– Self Management– Reduce unnecessary utilization– Improve Health Outcomes
RegistriesWhy – Risk Stratify– Colorectal CancerScreening– Mammography Screening– Hypertension– Depression– Asthma– Cardiovascular Disease– Cervical Cancer Screening Payer / ACO contract CMS Utilization data Huddle Sheets–––––ObesityHTN suspectPre DiabetesAsthma SuspectAnxiety Suspect
Patient Centered Medical HomeAlignment MDHAccess and CommunicationStandardRegistry StandardCare CoordinationCare Plan StandardQuality ImprovementStandardCPC Access and Continuity Care Management Comprehensiveness andCoordination Patient and CaregiverEngagement Planned Care andPopulation Health
Risk Stratification Process Algorithm Based Criteria Clinical Intuition
Algorithm Categorize patients into risklevels Diagnoses / Cluster Data Structured Fields in EMR Vendor - analytic software AutomatedClinical Intuition Care Team to refinealgorithm score– Social Needs– Utilization– Health Literacy– Activation– Caregiver Support– Behavioral / MedicalNeeds
Criteria - Utilization Hospital Encounter in the past year ED Encounter in the past year No Show Office Visit
Lab Values / Screening Tools A1CBlood PressureASCVD ScoreGAD scorePHQ 9 scoreACT score
Diagnosis COPDDiabetesCHFChronic Liver DiseaseDepressionChronic Kidney Disease
Other Criteria Age Smoking Status BMILook back period of one year
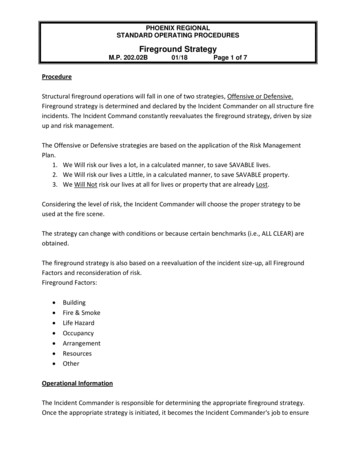
High Risk5%Medium Risk 20%Low Risk75%
High Risk – 5% Medium Risk – 20% Low Risk – 75% Data Analytics team analyzedthe entire patient populationbased on the algorithm todefine the populations
GOALSelf Management
Care Management Program Support patient self-management and activation.Awareness of community resources and social support.Coordination of care transitions and follow up.Coordinate closely with the care team, including Primary CarePractitioner, Integrated Health Therapist, Pharmacy, SocialWorker and Specialty providers. Receive and review timely information on hospital andemergency department admissions. Motivational Interviewing / Goal Setting
Care Managemento Risk Stratificationo Longitudinal Care Management Individualized Plan of Careo Episodic Care management Post hospital discharge ED Follow up Transitions in care
Future Enhancements – Criteria: Look back period – increaseUtilizationPoly PharmacyPediatric criteriaCKD, CAD, CHF, DepressionSocial Determinants of Health
Future Enhancements – Criteria
References Lin, J.S., Evans, C.V., Grossman, D.C., Tseng, C-W, Krist, A.H. Framework for usingrisk-stratification to improve clinical preventive service guidelines. Am J PrevMed. 2018;54:S26–S37.American Academy of Family Physicians. Risk-Stratified Care Management. ion/risk-stratified-care-mgmt-rubricGrembowski D, Schaefer J, Johnson KE, et al. ; AHRQ MCC Research Network. Aconceptual model of the role of complexity in the care of patients with multiplechronic conditions. Med Care. 2014;52 (Suppl 3):S7–S14.Grant RW, Ashburner JM, Hong CS, Chang Y, Barry MJ, Atlas SJ. Defining patientcomplexity from the primary care physician’s perspective: a cohort study. AnnIntern Med. 2011;155(12):797–804.Zulman DM, Asch SM, Martins SB, Kerr EA, Hoffman BB, Goldstein MK. Quality ofcare for patients with multiple chronic conditions: the role of comorbidityinterrelatedness. J Gen Intern Med. 2014;29(3):529–537. 10.1007/s11606-0132616-9.
4/9/2019Risk Stratification from aRural Perspective
Core TeamRisk stratification involves all members of the organizational team. While keyplayers may involve a physician champion, quality or population health staff,and administrative personnel, the work of Risk Stratification andimplementation of new policies, workflows, and procedures could not be donewithout considering the frontline staff and ancillary workers.“Change is more difficult when it’s coming from the people who are not familiarwith the work. The people who do the work have the best ideas, and that’s animportant concept not only to understand and absorb as a quality person, but toinstill in the team as well. ” –Alyssa Palmer, Southside Community HealthServices, Director of Quality
The Journey
Alexandria Clinic and HCH Initial certification PrimeWest and the Accountable Rural CommunityHealth (ARCH) agreement Horizon Public Health collaboration with PW andthe Alexandria Clinic to develop workflows basedon mutual goals
Initial Efforts at RiskStratification Received registry data from PrimeWest Care Coordinators made phone calls to patientsbased on their identified gaps in care A clinic level approach was focused on addressingthe needs of the Medicaid population Workflow was done by the care coordinators
Progression As the Quality Team continued to grow, riskstratification efforts grew as well New partnerships with more payors allowed forincreased access to data Culture change from a focused approach onspecific populations led to a clinic-wide change Risk stratification strategies were applied to theentire population and embraced by teammembers at all levels
Partnerships andData
ACOs and CommunityPartnerships ARCH agreement with PrimeWest HealthCentral Minnesota Health NetworkInsurance agreements with Humana and BCBSHorizon Public Health PartnershipLong term care (SNF)Controlled Substance Care Team and CommunityTask Force
Risk Stratification: PrimaryPrevention Best practice in cost reduction and quality of care Reports and data from partnerships guideworkflows to address gaps in care Creativity and continuous improvement to identifywhat works and what doesn’t
Examples
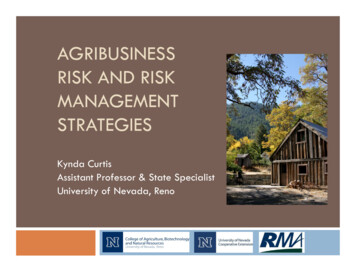
Hospitalizations/ED Use LPN Quality Team member works daily reports forhospitalizations and ED use Sends notifications (telephone encounters in Epic)to nursing team members for follow up Standard “dot phrase” used to ensure consistentfollow up is done Informal screening for care coordination done witheach chart review by Quality Team member
Transitional CareWorkflow Example
Hospitalizations and ED Use
Blue Card Initiative
Next Visit Begins Today
Risk Stratification HospitalReadmissions Quality team member runs monthly report of hospital readmissionsand gives to HCH Coordinator (Care Coordination lead at AlomereHealth)HCH Coordinator reviews chart for: Frequency of hospitalizations/ED visits Extensive diagnoses/Chronic Conditions Polypharmacy High risk diagnoses** Frequency of PCP office visitsSuggests care coordination consideration to PCP and CareCoordination TeamOnce enrolled in CC, MDH Tier Tool is used to further risk stratifyInformation is put into patient’s active problem list to indicate theirtier # and if they have external care plans
Where Do You GoFrom Here?
Types of Risk Stratifying Advance DirectivesMedicare Annual Wellness VisitsWell-Child VisitsMammogram CompletionColorectal ScreeningDiabetic Optimal Care MeasuresMental Health (Anxiety and Depression)HypertensionCOPDControlled Substance Use
What do you do with thisdata? Utilize Functionality in your EHRto run lists/build reports Use care team members Try different approaches Remember—It’s what you dowith this information that matters
Thank you!
Break
Questions for the Panel
Networking/Putting It Into Practice
Wrap Up and Key Learnings
Adjourn
Thank You!
Certified Health Care Home Clinics - 21 North Region - 20 South Region - Combine regions in April 2019 12 Large Metro Clinics 29 Small Regional Clinics