Transcription
DVT Prophylaxis inNeurosurgery“Seek simplicity and distrust it”Alfred North Whitehead
54
VTE Prophylaxis in Critically Ill Patients with:Intracranial HemorrhageAneurysmal Subarachnoid HemorrhageTraumatic Brain Injury (TBI)Brain TumorsSpinal Cord Injury
Recommendations for Prevention of VTEin Patients Undergoing Neurosurgical andNeurovascular Interventions in:Elective Spine SurgeryComplicated Spinal SurgeryElective CraniotomyElective Intracranial/Intra-arterialProceduresIntracranial Endovascular Procedures
DVT, PE or VTE?DVT is the most common, but is notalways seriousPE is the most serious, but is much lesscommonIf PE were always preceded by DVT, theDVT would be a reasonable surrogatemeasure, but it is notTherefore most researchers use VTE asthe measure of choice for analysis
Is VTE a Reasonable Choice ?It lumps minor superficial DVT with deathdue to massive pulmonary embolismDVT maybe independentof PE, precedeTherefore,VTE imates the risk of DVT and/orbe disabling without leading to PEPE with serious consequencesDVT and PE may be undetectedIn some studies as many as 50% of PEhave no associated DVT
Soooo Much DataBy my count, there at least 20randomized trials involving more than8,000 patients assessing somecomponent of VTE prophylaxispredominantly in intracranial surgeryThere are also at least 4 systematicreviews with meta analysis of thesubject(s)
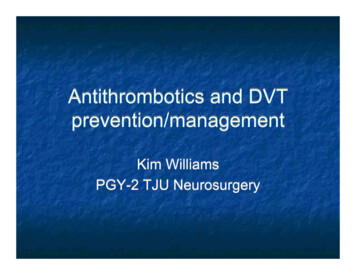
RCTREF18Nsrefs refer to "Beyond " paperPooled N4UFH vs LMWH23, 242472Craniotomy25, 263792Spinal surgery19, 20792 2CS to LMWH23UFH ICD75LMWH ICD25200UFH ICD188 2ICD to LMWH21, 28203 3UFH to placebo2930-32335092LMWH CS87153placebo CS154 20LMWH CS241placebo CS24427ICD60LMWH605ICD21UFH50placebo50 28UFH22LMWH23ICD LMWH55placebo4878CS80placebo1Spinal surgery1171Spinal surgery29N 50 UFHplacebo30N 70 ICDCSCan’t confirm 3rd ref Wautrecht33ICD57CS31CS ICD8160Mixed craniotomy and spine34N 95 ICDplacebo35104 1ICD to electrical stimMixed craniotomy and spine35UFHCalf stim 58 dextran4675ICD thigh59Used as cohort36134 1Thigh ICD to foot ICDSpinal surgeryUsed as cohortICD foot3612Cohort37, 38247 7Pharmacologic2LMWH aloneCraniotomyLMWH37392823401501LMWH and CSCraniotomy1UFH aloneCraniotomy41-43LMWH15039LMWH CS38972823UFH4015043UFH ICD872Craniotomy111642UFH ICD1063UFH and ICDFrim is used in both RCT andcohortUFH ICD41138ICD47344-46370 5Mechanical3ICD aloneSpinal surgery44 ICD3145ICD20047, 483922CS and ICDSpinal Surgery47 ICD CS7548 ICD CS3177716232Craniotomy3Craniotomy95 1ICD to placebo26UFH CS49Mostly craniotomy309 4CS to ICD34LMWH ICD48LMWH ICDMostly craniotomy19LMWH CS5, 2775 24UFH ICD46139
Meta AnalysisShould simplify by pooling dataCannot make all the included trials havethe same:Eligibility and exclusion criteriaChoice of prophylactic methodChoice of outcome measureand yet, pooling the data assumes that allof these things are so similar that thedifferences among the studies don’t matter
Khan, et al. J Neurosurg 129:906–915, 2018
Assumptions Underlying Meta AnalysesThe risk of VTE and IntracranialHemorrhage is the same in cranial andspinal patients
OutcomesSeparatelyAnalyzedAuthor Number of studies RCT Cohort Spine Included DVT PE VTEIorio4no yes no yesCollen 12 RCT, 18 cohortyes yes yes noHamilton6no no no yesKhan9yes yes no noComparing Meta nHamiltonKhanNumber of studies412 RCT, 18 cohort69RCTCohortSpine oyesno
Assumptions Underlying Meta AnalysesIs the risk of VTE and IntracranialHemorrhage is the same in cranial andspinal patients ?Is it OK to include non-randomized cohorts ?Is it OK to assume that DVT and VTEoutcomes are similar enough to pool?
Comparing Meta AnalysesMethods of Diagnosis for inogen angio CT V/QAll methods used inconsistently across studies
Assumptions Underlying Meta AnalysesIs the risk of VTE and IntracranialHemorrhage is the same in cranial andspinal patients ?Is it OK to include non-randomized cohorts ?Is it OK to assume that DVT and VTEoutcomes are similar enough to pool?Is it OK to assume that using differentdiagnostic methods doesn’t affect outcome?
Comparing Meta AnalysesMethods of ntcompression compression unfractionatedenoxaparin nadroparinheparindevicesplacebo stockingsAll methods used inconsistently across studies
Assumptions Underlying Meta AnalysesIs it OK to assume that using differentmethods and combinations of prophylaxisdoesn’t affect outcome?In addition, many studies mix populations ofpatients known to have different risk of VTE(brain tumor patients subarachnoidhemorrhage patients and other electiveintracranial surgery patients)
Well, let’s just assumethat all thoseassumptions are OK
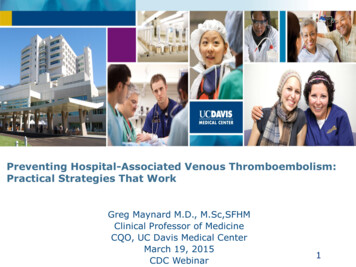
Odds Ratiofor DVT for DVTOddsRatio0.900.900.800.700.600.500.50lower 95% ci0.40Odds Ratioupper 95% Collen Hamilton Khan
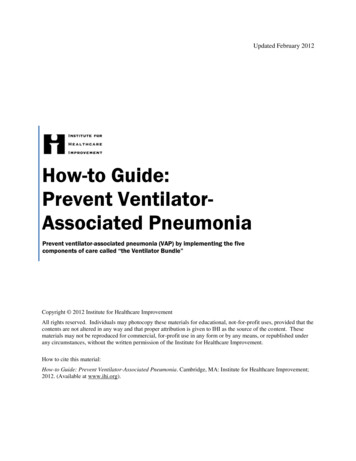
4.00Odds Ratio for ICH or Maj. Hem.4.003.503.003.002.502.00lower 95% ci2.00Odds Ratioupper 95% KhanCollen Hamilton Khan
Another Viewproportion with VTENNTabsolute NumberNumber ofnon-pharmchemoriskNeededstudiesAuthorprophylaxis prophylaxis reduction to TreatAgnelli4 RCT0.1297.740.2900.161Collen12 RCT, 18 cohort0.0610.0330.02934.59Hamilton6 RCT0.1128.930.2600.148Khan9 RCT0.08911.240.2150.126
Another Viewproportion with ICH ormajor hemorrhageNNHabsolute NumberNumber ofNeeded torisknon-pharm chemostudiesHarmprophylaxis prophylaxis increaseAuthor102.200.00984 RCTAgnelli0.02350.013711.260.088812 RCT, 18 cohort 0.0630Collen0.1244100.000.01006 RCTHamilton0.05000.0400111.110.00909 RCTKhan0.03300.0240
trying to simplify the comparisonAuthorCollenIorioHamiltonKhanabsolute riskreduction0.030.130.110.09NNTNumberNeeded toTreat358911NNHNumberabsolute Needed torisk increaseHarm0.09110.011020.011000.01111
diConstantiniKhan
ConclusionsMeta-analysis does not fix flaws in theincluded studiesDifferent approaches to inclusion andexclusion lead to wildly different resultsIt isn’t clear which is rightMore than 3 decades of uncoordinatedunderpowered randomized trials havefailed to provide clear guidance on thisissue
DVT Prophylaxis in Neurosurgery . prophylaxis chemo-prophylaxis absolute risk increase Number Needed to Harm Agnelli 4 RCT 0.0137 0.0235 0.0098 102.20 Collen 12 RCT, 18 cohort 0.0630 0.1244 0.0888 11.26 Hamilton 6 RCT 0.0400 0.0500 0.0100 100.00 Khan 9 RCT 0.0240 0.0330 0.0090 111.11