Transcription
Antithrombotics and DVTprevention/managementKim WilliamsPGY-2 TJU Neurosurgery
Introduction In Neurosurgery, antithrombosis is a critical andcontroversial issue.Deep Vein Thrombosis (DVT) is a serious concern forNeurosurgical patientsMany neurosurgery patients are prone to clotting: Long operative timesParalysis/prolonged bed restHypercoaguabilityTrauma/SAHStroke
IntroductionThe coagulation cascade Hypercoaguablility Classes of Antithrombotics - a review ofthe drugs DVT and Surgical prophylaxis
Inherited Hypercoaguability(HC) There are many causes of inherited HC: Factor V LeidenHyperhomocysteinemiaProthrombin G20210AAT, or Protein C and/or S deficiencyAntiphospholipid antibody syndromeFactor deficiency (VII, IX)DysfibrinogenemiaPlasminogen deficiency
Acquired Hypercoaguablility There are many causes of acquired HC as well: Lupus anticoagulantMalignancy/myeloproliferative HFPregnancyObesityOld age
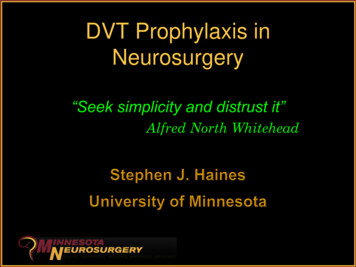
Hemostasis VIRCHOW’S TRIAD Primary Hemostasis Platelet adhesionSecondary Hemostasis Contact activation pathway (intrinsic) Tissue factor pathway (extrinsic) Final common pathway
Hemostasis: Virchow’s Triad Endothelial injury/dysfunctionHypercoaguabilityHemodynamic changes StasisTurbulence
Primary Hemostasis Activated when subendothelial connective tissueis exposedStarts with rapid platelet aggregation Platelets will then aggregate at the site of injury Within secondsvon Willenbrand Factor (vWF)Platelets will bind to each other using fibrinogenand glyoprotein IIB/IIIa complexes
Contact activation pathway(intrinsic) Hageman factor (Factor XII), High-Molecularweight Kininogen (HMWK), and prekallikrein(PK) form a complex on subendothelial colagenFactor XII XIa Xa final common pathMonitored by PTTProbable minor role in coagulation as patientswith deficiencies have normal hemostasis
Tissue factor pathway (extrinsic) Factor VII is activated into a protease,forming a complex with Tissue Factorwhich is then converted to factor XaVitamin K dependentMonitored by PTMajor role in coagulation
Final common pathway Factor X is activated (Xa) by Factor VIII byactivated factor IX (IXa)Xa and factor V then convert prothrombininto thrombin using several other factors Calcium, phospholipidThrombin then bind fibrinogen and formfibrinFibrin then uses factor XIII to cross-link
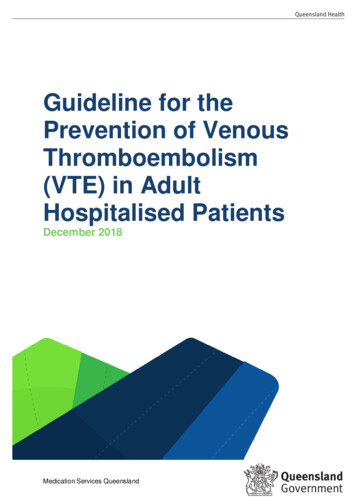
The Coagulation Cascade
Antithrombotics - Two majorclasses Antiplatelet Glycoprotein IIB/IIIa inhibitorsADP receptor/P2Y inhibitorsCox inhibitorsAnticoagulants Vit K antagonists (inhibits II, VII, IX, X)Factor Xa inhibitors (some II inhibition)Direct thrombin (II) inhibitorsOther: Antithrombin III
Classes of Antithrombotics Antiplatelet Glycoprotein IIB/IIIa inhibitors ADP receptor/P2Y inhibitors Plavix, ticlopidineCox inhibitors Abciximab (ReoPro), tirofibanAspirinOther Dipyridamole
Acetylsalicylic Acid (Aspirin) Irreversibly inhibits cyclooxygenase andprevents synthesis of thromboxane A2,which prevents platelet aggregationPeak concentration in 1hour, lasts up to aweek (duration of platelet life-span)Platelets for reversal
Clopidogrel (Plavix) Irreversibly inhibits P2Y2 subset of the ADPreceptor The ADP receptor is important in plateletaggregation and the cross-linking of platelets byfibrinInhibition detectable 2 hrs after 400mg dosePlatelet function returns 7 days after lastdoseAlternative for aspirin
Abciximab (ReoPro) GIIb/IIIa inhibitor - prevents fibrinogen adhesionBinds to platelets with half-life of 10 minutes, buteffects can last up to 48 hoursIndicated for use in individuals undergoingpercutaneous coronary intervention (angioplastywith or without stent placement) The use of abciximab in this setting is associated witha decreased incidence of ischemic complications dueto the procedure
Reversal of Antiplatelets in Spontaneous ICHAuthor Number (n)AgentDesign InterventionRoquer, 05194 total47Antiplatelet43 ASA, 2T, 1 C, 1 DProspective, n/aObservationalToyoda, 05251 total57Antiplatelet33 ASA, 12T, 3 Cl, 7ASA TRetrospecti n/ave,ObservationalCantalapiedra, 06500 total49Antiplatelet37 ASA, 3C, 4Tri, 3DRetrospecti n/ave,ObservationalAPAuthor NumbeEffectsr (n)Independentpredictor of30 daymortalityp 0.004 OR2.77 (1.38–5.59)Independentpredictor ofhematomaenlargementp 0.01 OR7.67, (1.62to 36.4)Predictor ofneed foremergentsurgicalevacuationOR 3.10(1.18–8.15)30 daymortalityfor APgroup44.9% vscontrols29.9%AgentDesignRoquer, 05194 total47Antiplatelet43 ASA, 2T, 1 C, 1 DProspective,ObservationalToyoda, 05251 total57Antiplatelet33 ASA, 12T, 3 Cl, 7ASA TRetrospective,ObservationalCantalapiedra, 06500 total49Antiplatelet37 ASA, 3C, 4Tri, 3DRetrospective,Observational
Reversal of Antiplatelet Agents in TraumaticICHAuthor Number(n)AgeAgentType ofICHDesignInterventionAP EffectsASA is a risk factor for ICHafter head injury (13%)Of all ASA patients, none hadinsignificant bleedingcompared to 6 controlsSimilar in-hospital mortality(34.5% in AP group vs 30.0%in controls), but AP grouprequired more craniotomies(79.3% vs. 76.4%)Increased in-hospitalmortality (38% of AP vs 8%of controls, p 0.006)Reymond,92198 TotalAllAll ASASevere ICHRetrospectiveN/ARozzelle, 95157 Total31 Antiplatelet 65Not SpecifiedSubduralHematomaRetrospectiveN/AMina, 0271 Total34Anticoagulation231 Total110AntiplateletAll12 W, 19ASA, 1 E, 1C, 1 PAny traumatichead injury*RetrospectiveN/A 60100mg ASAMainly Mild HeadInjury*Prospective,observational 2centersN/A50 ASA,12C, 20combination43 CAny traumaticICHRetrospective25 Head Injury*Retrospective24 patientsreceivedtransfusion29 patientsreceivedplatelettransfusionSpektor, 03Ohm, 05179 Total90 Antiplatelet 50Jones, 061020 AllTrauma43 Antiplatelet 50Similar rates of ICH in bothgroups (24.5% vs. 25.6%)Similar rates of surgicalintervention in both groups(4.5% vs 4.1%)Increased in-hospitalmortality (23% of AP vs8.9% of controls, p 0.016)No statistics provided, buthigher numbers of cranialsurgery, rebleeds, andtransfusions in ClopidogrelgroupComparable lengths of stay
Classes of Antithrombotics Anticoagulants Vit K antagonists (inhibits II, VII, IX, X) WarfarinFactor Xa inhibitors (some II inhibition) Heparins, lovenoxDirect Xa inhibitors Direct thrombin (II) inhibitors RivaroxabanLepirudinArgatrobanOther: Antithrombin III
Heparin Heparin is produced by bovine lung andporcine mucosaHeparin binds to, and activates, theinhibitor anti-thrombin III (AT)The activated AT then inactivates thrombinand factor Xa
Heparin Heparin does not break down clots thathave already formedIt allows the body's natural clot lysismechanisms to work normally to breakdown clots that have formedUse protamine for reversal
Heparin - HIT H.I.T. - Heparin induced thrombocytopeniaIgG antibodies to PF4 in patientspreviously exposed to heparinIgG, PF4, and heparin form complex whichactivates platelets and clots decreasedplatelet number
Enoxaparin Enoxaparin decreases thrombin formation and ultimately preventsfibrin clot formation. It binds to Antithrombin III which then inhibits factor Xa.Factor Xa catalyzes the conversion of prothrombin into thrombin whichthen is used for fibrin clot formationEnoxaparin does not affect the INR, PT, or PTT.The only monitoring is to measure anti-Factor Xa levelsProtamine can be used for reversal
Fondaparinux (Arixtra) Mediates effect indirectly through ATIt is selective for factor Xa Unlike HeparinLower incidence of H.I.THalf-life is 130 hours May be longer in pt’s 75yrs or 50kg
Argatroban A small molecule direct thrombin inhibitor. Indicated for prophylaxis or treatment of thrombosis inpatients with HIT Liver metabolized; monitored by PTT May falsely elevate INR The combination of argatroban and warfarin may raise the INRto greater than 5.0 without a significant increased risk ofbleeding complications.
Coumadin (Warfarin) Inhibits Vitamin K-dependent synthesis ofclotting factors II, VII, IX, and X as well asProtein C and Protein SIs monitored by the PT or INRMay be reversed with vitamin K, factor IX(profilnine), or fresh frozen plasma
Tissue Plasminogen Activator(tPA) Obtained from ß-hemolytic strep Binds to serine protease found on endothelial cellsof vessels Pt’s with prior exposure to tPA or previous strep infectionsmay be resistant to tPACatalyzes plasminogen to plasmin conversionCleaves the single chained plasminogen into two chainsMust be used within 3 hours of onset of CVAsymptomsaminocaproic acid works as an antidote
DVT Morbidity and Mortality
DVT Morbidity and Mortality Mark et al. reported a 24.8% prevalencerate of PE in a consecutive autopsy seriesof 101 patients with neurological disease.Pulmonary embolism was the primarycause of death in almost half of thesepatient
DVT Morbidity and Mortality Dalen and Alpert estimated the incidence of PEin the United States to range as high as 630,000cases per year, resulting in 200,000 (32%)deaths.Risk Factors: older age, obesity, varicose veins,immobility, pregnancy, puerperium, estrogentherapy, previous DVT or PE, deficiency ofantithrombin III, protein C or protein S, trauma,surgery, malignancy, heart failure, and infection
DVT Morbidity and Mortality DVT can lead to pulmonary embolism withsubsequent cardiopulmonary arrest Stroke from paradoxical emboliIn Neurosurgery patients PE formationrates range between 0 and 5%, with asignificant mortality rate varying from 9 to50%
DVT Morbidity and Mortality
DVT Morbidity and Mortality
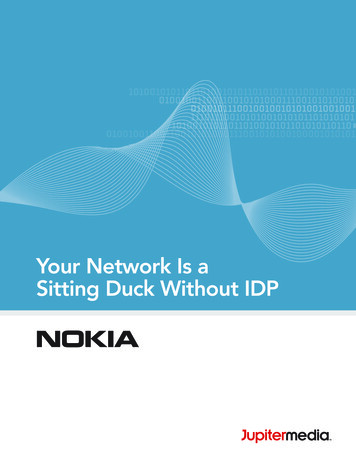
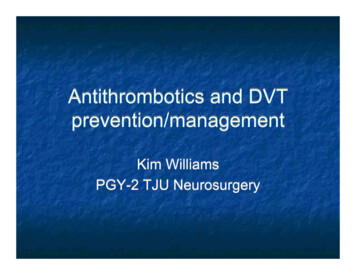
In the Beginning In 1993, Laohaprasit and Mayberg looked at theoptimal postoperative interval after whichheparin therapy can be safely initiated They used fifty rats weighing 450 to 500 g thatwere assigned to 10 groupsNine groups of five rats each had heparinstarted 1, 2, 3, 5, or 7 days after standardizedbilateral frontal corticectomy and was continuedfor 7 days.The last group was the control - saline
In the Beginning There were two ranges, 1.5x therapeutic, and 3xtherapeuticAfter 7 days the rats were sacrificed and thebrains were stained for amount of bloodIntracerebral hematomas were classifiedaccording to three categories: minimal (0-10mm3), small (10-50 mm3), or large ( 50 mm3)
In the Beginning
In the Beginning
In the Beginning Conclusion: heparin therapy can be safelyinitiated at 48 hours after craniectomy andcorticectomy in the rat,supratherapeutic anticoagulation isassociated with intracerebral hemorrhagefrom 3 to 5 days after surgery.
DVT prophylaxis Non-pharmacologic: TED’s/SCD’s have class I evidence forefficacyEarly ambulationTEDs/SCD’s should not be used inconfirmed DVT
DVT Prophylaxis - Heparin Levin et. al did a retrospective analysis of 10studies looking at VTE rates in patients whowere H.I.T. positiveThey compared UFH to LMWH hypothesizingthat development of H.I.T. is associated withhigher VTE ratesThe frequency of HIT-associated VTE amongUFH and LMWH (12.8% [31 of 242 patients] vs0.7% [1 of 144 patients]; odds ratio, 21.0; 95% confidence interval, 2.8 to 156;p 0.001.
DVT at TJU The frequency of DVT and PE in untreatedpatients with SCI is around 67-100%PE is the third leading cause of death inthe SCI population
DVT at TJU Literature review looking at 23 studiescomparing different modalities of DVTprophylaxis in patients with spinal cordtrauma with and without injury
DVT at TJU Looked at several variables: Mechanical vs. combined prophylaxis in acuteSCIvitamin K antagonist vs. non-vitamin Kantagonist prophylaxis in acute SCIUFH vs. LMWH in acute SCIStart and duration of prophylaxis in acute SCI
DVT at TJU: Inclusion Criteria Randomized studiesAdequate complianceAdequate duration of treatmentObjective tests for DVT, PE and bleeding(LEUS, VQ, CTA, positive guiac etc)
DVT at TJU The prevalence of deep-vein thrombosis wassignificantly lower in patients without spinal cordinjury (odds ratio 6.0; 95% confidence interval 2.9 to 12.7; p 0.00001, fixed effects)however, the prevalence of pulmonary embolismdid not differ significantly between the twogroups (odds ratio 1.5; 95% confidenceinterval 0.2 to 15.4; p 0.73, fixed effects).
DVT at TJU: Results LMWH is more effective than UFH for theprevention of DVT in patients with acuteSCIBoth are equivalent for PE preventionLMWH has had fewer bleedingcomplications than UFH in patients withacute SCI
DVT Prophylaxis - LMWH(Lovenox) Tetri et. did a retrospective analysis of 407 patients whowere admitted for ICH of 3 month mortality.232 received lovenox, 175 did notThere was a higher incidence of increased hemorrhagein the treated group that was statistically significant.However, there was an increase in PE in the non-treatedgroupOverall, there was a decrease in mortality in the treatedgroup, but it wasn’t statistically significantAlso, there was a significant worsening of GOS in thetreated group
DVT Prophylaxis - LMWH(Lovenox) Spyropoulos et. al looked retrospectively at venousthromboembolism prevention in cancer patients922 neurosurgery patients were split into LMWH and notreatment groups.There was a statistically significant decrease in VTE intreated patients (p 0.001)However there was also an increase in major bleedingevents and for every 7 VTE’s prevented there was 1major bleeding event.
DVT Prophylaxis - LMWH(Lovenox) Dickinson LD et. al looked prospectively atDVT prophylaxis in 68 patients undergoingcraniotomyThree Groups were compared over amonth using ANOVA SCD 22 patientsLovenox 23 patientsBoth 23 patients
DVT Prophylaxis - LMWH(Lovenox) Inclusion criteria Age 18 with diagnosis of intracranial neoplasmUndergoing surgeryExclusion criteria History of DVT or pulmonary embolismAllergy to heparin or other anticoagulant agentsHistory of surgery or major trauma to the lower extremitiesConcurrent condition requiring anticoagulation therapycranial base neoplasms and pituitary adenomas
DVT Prophylaxis - LMWH(Lovenox) DVT was observed for 8 of the 66 studypatients, yielding an overall DVT incidenceof 12%All patients with DVT had undergonecraniotomy procedures
DVT Prophylaxis - LMWH(Lovenox) DVT incidence in treatment group was 3 of 22 (13.6%) in the SCD-treated group1 of 21 (4.76%) in the enoxaparin-treated groupThe difference was not statistically significant (P 0.53).DVT incidence in the combined group was 4 of23 (17.4%) also not significantly different from that for the SCDtreated group (P 0.90).
DVT Prophylaxis - LMWH(Lovenox) Post-op ICH did not occur in the SCDtreated group5 of 46 patients receiving low-molecularweight heparin suffered clinicallysignificant intracranial hemorrhageThe study was terminated because of theincreased incidence of adverse events inthe enoxaparin-treated groups.
DVT Prophylaxis - LMWH(Lovenox) Lovenox groups received 30mg SQ in theanesthesia holding room.Lovenox was continued from holding at30q12 until discharge
DVT Prophylaxis - LMWH(Lovenox) Four of the five patients with intracranialhemorrhaging demonstrated gliomas inhistological examinations.Three developed a new neurologicaldeficit within 6 hours of recovery fromanesthesia, two required an emergency return to theoperating room for evacuation to preventherniation
DVT and PE treatment The only current absolute contraindications foranticoagulation are patients with an unsecuredaneurysm after a subarachnoid hemorrhage orpatients with an acute intracerebral hemorrhageor hematomyeliaAlthough the possible outcome of an intracranialhemorrhage might include increasedneurological disability or death, there is no doubtabout the very high mortality associated with PE
DVT and PE treatment Level I evidence has substantiated theefficacy and safety for starting warfarin onthe same day as the heparin therapy isstarted.Warfarin should always be overlappedwith heparin for 4 to 5 days, withdiscontinuation around 5 to 7 days
DVT and PE treatment What about Inferior vena cava filters (IVCF)?IVCF are an alternative to full anticoagulation in thosepatients at highest risk for catastrophic hemorrhagiccomplicationsIVCF has a limited role after a patient has passed out ofthe high-risk period for bleeding complications beyond securing the aneurysm or beyond 1 to 2 weeks afterintracranial surgeryTherefore, full anticoagulation should be reconsidered,because the patient remains at risk for continued venousthrombosis and postphlebitic syndrome.
DVT and PE treatment Unfortunately there is no information todefine the the risk for hemorrhage after thefirst week after intracranial surgery.There is weaker evidence to suggest thesafety of therapeutic anticoagulationbetween postoperative Week 1 and Week6
References Kasper et. al. Harrison’s: Principles of Internal Medicine. 16th ed. McGraw-Hill2005Hamilton MG, Hull RD, Pineo GF. Venous thromboembolism in neurosurgeryand neurology patients: a review. Neurosurgery. 1994 Feb;34(2):280-96;discussion 296. Review.Mark P, Horst HM, Diaz FG. Neurosurgical patients: At high risk for pulmonaryemboli. Surg Forum 37:522–523, 1986Dalen JE, Alpert JS: Natural history of pulmonary embolism. Prog CardiovascDis 17:259–270, 1975Green D, Lee MY, Ito VY, Cohn T, Press J, Fibrandt PR, VandenBerg WC,Yarkony GM, Meyer PR Jr: Fixed- vs adjusted-dose heparin in the prophylaxis ofthromboembolism in spinal cord injury. JAMA 260:1255ミ1258, 1988.Tetri S, Hakala J, Juvela S, Saloheimo P, Pyhtinen J, Rusanen H, SavolainenER, Hillbom M. Safety of low-dose subcutaneous enoxaparin for the preventionof venous thromboembolism after primary intracerebral haemorrhage. ThrombRes. 2008;123(2):206-12. Epub 2008 Apr 16.Spyropoulos AC, Brotman DJ, Amin AN, Deitelzweig SB, Jaffer AK, McKeanSC. Prevention of venous thromboembolism in the cancer surgery patient. CleveClin J Med. 2008 Apr;75 Suppl 3:S17-26.
References Laohaprasit, V; Mayberg, MR. Risks of Anticoagulation Therapy after ExperimentalCorticectomy in the Rat Neurosurgery: Volume 32(4),ハApril 1993,ハp 625-629Skillman JJ, Collins REC, Coe NP, Goldstein BS, Shapiro RM, Zervas NT, BettmannMA, Salzman EW: Prevention of deep vein thrombosis in neurosurgical patients: Acontrolled, randomized trial of external pneumatic compression boots. Surgery83:354ミ358, 1978.Dickinson LD, Miller LD, Patel CP, Gupta SK. Enoxaparin increases the incidence ofpostoperative intracranial hemorrhage when initiated preoperatively for deep venousthrombosis prophylaxis in patients with brain tumors. Neurosurgery. 1998Nov;43(5):1074-81. PMID 9802851A. Ploumis, MD, PhD, R.K. Ponnappan, MD, M.G.Maltenfort, PhD, R.X. Patel, BS,J.T. Bessey, BS, T.J. Albert, MD, J.S.Harrop, MD, C.G. Fisher, MD, C.M. Bono, MD,and A.R. Vaccaro, MD, PhD Thromboprophylaxis in patients with acute spinalinjuries: an evidence-based analysis. J Bone Joint Surg Am. 2009 Nov;91(11):256876.Levin RL, McCollum D, Hursting MJ. How frequently is venous thromboembolism inheparin-treated patients associated with heparin-induced thrombocytopenia? CHEST2006 Sep;130(3):681-7.
IntroductionIntroduction In Neurosurgery, antithrombosis is a critical and controversial issue. Deep Vein Thrombosis (DVT) is a serious concern for Neurosurgical patients Many neurosurgery patients are prone to clotting: Long operative times Paralysis/prolonged bed rest Hypercoaguability Trauma/SAH Stroke In Neurosurgery, antithrombosis is a critical and