Transcription
MARCH2013THE VALUE OFMEDICAL DEVICEINTEROPERABILIT Y:Improving patient carewith more than 30 billionin annual health care savings@westhealth #interoperabilitywesthealth.org
ABOUT WESTHEALTH INSTITUTEwesthealth.org@westhealthThe West Health Institute is an independent, non-profit501(c)(3) medical research organization whose missionis to lower health care costs by developing innovativepatient-centered solutions that deliver the right care atthe right place at the right time. This is accomplishedby conducting innovative medical research, educatingkey stakeholders and advocating on behalf of patients.Solely funded by pioneering philanthropists Garyand Mary West, the Institute is part of West Health,an initiative combining four separate organizations– the West Health Institute, the West Health PolicyCenter, the West Health Investment Fund and the WestHealth Incubator. The Institute is located in San Diego,California, the global center for health care innovation.For more information, find us at westhealth.org andfollow us @westhealth.CONTENTS03ABSTRACT13DETAILED ALL TO ACTION10SUMMARY OF RESULTS36APPENDIX:Detailed CalculationsABSTRACTUnsustainable and ever-escalating U.S. health care costs, an estimated 700 billion inwasteful spending and the emerging centricity of medical information and its seamlessavailability in the search for solutions prompt investigation into the value of creatingfunctional medical device interoperability – the ability for medical devices to exchangeinformation with each other and with patient data repositories such as electronichealth records.ACKNOWLEDGEMENTSThis report examines areas of waste in health care that can potentially be eliminatedthrough greater medical device interoperability and the adoption of commonlyaccepted standards for interoperability. Waste reduction through greater medicaldevice interoperability would lead to increased efficiency, improved quality and moreaffordable care. Commonly adopted standards can accelerate the move towardsgreater medical device interoperability and potentially reduce the cost of achievinginteroperability. With all of the caveats associated with estimating the value of aprocess improvement not yet deployed, our combined top-down and bottom-upmodeling suggests that annual savings in excess of 30 billion may be liberated bywidespread adoption of functional interoperability for medical devices.The Medical Device Interoperability CoordinatingCouncil (MDICC) is an open forum to allow collaborationbetween stakeholders that are actively engaged inaspects of promoting or creating interoperable medicaldevice systems. The MDICC formed in March 2012to advance wide adoption of medical devices thatseamlessly interoperate with other medical devices andinformation systems with the goal of enabling improvedpatient care. This analysis was prompted, in part, byMDICC’s efforts, which validated the need to betterquantify the value of medical device interoperability.Several individuals within MDICC deserve thanks fortheir contributions to this work.Copyright 2013 Gary andMary West Health InstituteTo realize the benefits, providers, payers, medical device manufacturers and thegovernment will need to collaborate and partner to promote the development andadoption of seamlessly interoperable devices. Industry trends are already drivingproviders and payers to converge and share risk through care coordination, clinicalintegration and improved population health management. Stakeholder collaborationis expected to provide a strong platform for accelerating adoption of medical deviceinteroperability and realizing its associated benefits.
INTRODUCTIONINTRODUCTIONHealth IT, Medical Devices and InteroperabilityINTRODUCTIONOverviewHealth care costs continueto consume an everincreasing proportionof U.S. spending,significantly outpacingthe growth of oureconomy for each of thelast four decades, andrecently reaching as highas 18 percent of grossdomestic product (GDP).1Healthcare costs18%U.S. grossdomestic productWhile both the absolute level of spending and its disproportionate growth areunsustainable, evidence indicates that as much as a third of this spending is waste(i.e., does not contribute to quality outcomes). According to recent estimates, morethan 700 billion of the 2.4 trillion in health care spending could otherwise beavoided through improvements to the health care system.1 Waste takes many forms,including inefficiency, unnecessary services and missed prevention opportunities, andis believed to be broadly distributed across the spectrum of health care delivery.This study examines the sources of waste in health care that could be eliminatedwith medical device interoperability, as well as the waste resulting from a lack ofcommonly adopted interoperability standards. The report’s findings suggest thatincreased medical device interoperability would reduce waste, lead to improvementsin quality and decrease the cost of care. Additionally, comprehensive adoption ofinteroperability standards has the potential to reduce waste related to developingand implementing interoperability and facilitate increased interoperability.4The Value of Medical Device InteroperabilityWest Health InstituteDespite a nationwide push for adoption of information technology throughout thehealth care system and the concurrent significant advances in the technologiesunderlying medical devices, numerous barriers continue to impede the realizationof health information technology’s potential. A lack of functional medical deviceinteroperability is one of the most significant limitations.Medical device interoperability refers to information sharing from one device toanother or between devices and Electronic Health Records (EHRs). Functionalinteroperability would enable clinical medical devices to communicate in aconsistent, predictable and reliable way. By allowing for the exchange of data withother medical devices and with patient data sources and repositories, such as EHRs,medical device interoperability would enhance the function of the systems anddevices. Exchange of data between EHRs is commonly designated as HealthcareInformation Exchange (HIE) and has been analyzed in great detail elsewhere.2 Thereliable and seamless transfer of information through medical device interoperabilitycan facilitate a number of improvements in efficiency and safety that can bequantified in billions of dollars of savings to the health care system, yet, despitethese significant benefits, medical device interoperability is limited today.WASTE:Any activity that does not add value to the health caresystem.Health IT, Medical Devices and InteroperabilityFUNCTIONAL MEDICAL DEVICE INTEROPERABILITY:the ability for clinical medical devices to communicate ina consistent, predictable and reliable way, allowing for theexchange of, and interaction with, data from other medicaldevices and with patient data sources and repositories, suchas electronic health records (EHRs), in order to enhancedevice and system functionality.5
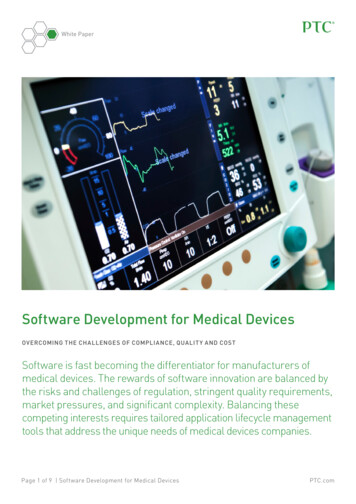
INTRODUCTIONINTRODUCTIONThe Current State of Medical DeviceInteroperability and Interoperability StandardsAccording to a recent report by HIMSS Analytics,3 while over 90 percent ofthe hospitals surveyed by HIMSS use six or more types of devices that couldbe integrated with EHRs (such as defibrillators, electrocardiographs, vital signs monitors, ventilators and infusion pumps) only a third of hospitals actuallyintegrate medical devices with EHRs today. Additionally, those that are investing ininteroperability integrate fewer than three types of devices on average, a far cry fromthe six to twelve devices that may be present around an intensive care unit (ICU) bed.This lack of interoperability creates significant sources of waste and risk to patientsafety because of incomplete or stale information clinicians must rely on for workflowand decision making.Part of the reason for limited interoperability is the high cost and complexity ofmedical device integration, which results from the lack of incentives for medicaldevice and HIT companies to use open interfaces to establish interchangeableinteroperability. In contrast to the “plug and play” world of consumer electronics,where consumer demand for simple and seamless functionality has drivenconvergence on a few common standardized interfaces and platforms, providers havenot required a consistent means for achieving interoperability. As a result, there isa wide range of methods used by device vendors today. Some vendors use distinctproprietary and closed communication methods even among their own devices.Additionally, some standards are loosely specified, with a number of options forconfiguration, meaning that even devices that use similar standards may not be ableto communicate without further customization. As a result, facilitating the exchangeof data between and among medical devices and EHRs currently requires hospitalsto invest significant resources in developing custom interfaces and paying formiddleware solutions. The cost of medical device integration has been estimated atas much as 6,500 to 10,000 per bed in one-time costs, plus as much as 15 percentin annual maintenance fees.4 These investments are a substantial undertaking forhospital systems when compared against already squeezed operating margins ofless than three percent on revenue of approximately 700,000 per bed (based onaverage length and cost of inpatient stays).5,6Within the current system, the medical device industry lacks the imperative to offerinteroperability among devices because providers who are integrating bear thesecosts and do not require medical device companies to follow specific standards.Many providers continue to work without interoperability since the value propositionhas not been adequately quantified to drive prioritization of the investmentsnecessary to achieve integration over competing technology or other needs. Whilemiddleware software providers and systems integrators have issued white papersillustrating the impact of medical device integration at a hospital level,7 there6The Value of Medical Device InteroperabilityWest Health Institute90%of hospitals use sixor more types ofdevices that could beintegrated with EHRsof hospitals actuallyintegrate medical deviceswith EHRs todayfewer than3only1/3types of devices on averageare integrated in thosehospitals investing ininteroperabilityhave been no studies to date attempting to quantify the value of medical deviceinteroperability in addressing waste across the health care system as a whole. Therehas also been no detailed examination of the waste generated by the lack of commonlyadopted standards. Given the efficiencies and quality assurance tools medical deviceinteroperability offers, this report provides health care stakeholders a clear andcompelling case to invest in medical device interoperability.This paper examines the benefits of medical device interoperability in terms of thereduction of waste in health care. It also estimates the costs that could potentially beeliminated in a world where medical devices are connected in a standardized manneras computer and communications devices do today.7
METHODOLOGYThis report limited the scope of its analysis to interoperability between clinicalmedical devices and patient data repositories such as EHRs and device-todevice interoperability. It included only those clinical devices that are potentiallyinteroperable today, encompassing bedside monitoring devices (e.g., ECGs andphysiologic monitors), imaging devices, diagnostic devices, surgical devices andtherapeutic devices (e.g., infusion pumps). It focused on acute care (encompassingemergency room and inpatient settings) and did not examine the benefits ofinteroperability between EHRs in different health care organizations since HIEsconstitute a distinct type of interoperability and have been analyzed in detailelsewhere.2 Finally, while it is appreciated that the lack of functional interoperabilityamong consumer medical devices (e.g. glucometers, weight scales and blood pressuremonitors) outside the hospital and between such devices and more central EHRs isa related significant and growing challenge with its own attendant waste, the lack ofconformity around the magnitude and growth of this aspect of the issue precludedit being included in this analysis, making the results of this work a more conservativeestimate of the overall impact of true, functional interoperability.for which the impact of interoperability could be readily quantified, and others wereidentified as longer-term savings opportunities that were indirect (i.e., would requireseveral additional enabling factors to address) or were difficult to measure andtherefore not specifically quantified in this report (Figure 1).Figure 1: Areas of Waste IdentifiedPrimary Stakeholders BenefitedQuantified Areas of WasteProvidersPayers Patients DeviceCo.Due to Lack of Medical Device Interoperability1. Adverse events from drug errors, misdiagnosis andfailure to prevent harm2. Redundant testing resulting from inaccessibleinformation3. Clinician time spent manually entering information4. Increased length of stay from delays in informationtransferD D DD D DDDDue to Lack of Commonly Adopted Standards for InteroperabilityThis analysis followeda three-stage process:1238Identification ofrelevant sources ofhealth care wasteDefinition andquantification ofthe addressablebuckets of wasteDefinition andquantification ofthe share of costsaddressable byinteroperabilityThe Value of Medical Device InteroperabilityWest Health InstituteIDENTIFICATION OFRELEVANT SOURCES OFHEALTH CARE WASTEMETHODOLOGYMethodology5. Device testing and development costs6. Provider costs to integrate devices with EHRsIndirect or Difficult to Quantify Areas of WasteDDPrimary Stakeholders BenefitedProvidersPayers Patients DeviceCo.Due to Lack of Medical Device InteroperabilityRelying on the Lean Six Sigma methodologyas a lens to define waste as “all activity thatdoes not add value to the health care system,”the perspective of each stakeholder withinthe ecosystem was examined to identify areaswhere waste could potentially be addressedand eliminated through interoperability.8Interviews with more than 30 stakeholdersfrom across the health care ecosystem(including providers, payers, medical devicemanufacturers and health IT vendors), alongwith secondary research, led to identifying tenareas of waste that fell into two categories:those arising from the lack of interoperabilityand those arising from a lack of commonlyadopted standards. Of these, some weredetermined to be primary sources of waste7. Limited ability to collect and leverage data analyticsto improve clinical decision support8. Sub-optimal care driven by limited adoption andefficacy of remote patient monitoring9. Limited ability for operational maintenance andoptimization of utilization/inventory managementD D DD DDDue to Lack of Commonly Adopted Standards for Interoperability10. Limited device choice, innovation and competitiondue to switching costsDDDEFINITION AND QUANITIFICATION OF THEADDRESSABLE BUCKETS OF WASTEFor each segment of waste, a reference market was established to set a maximumvalue of spending that could be impacted by interoperability. For example, theanalysis of savings related to “time wasted manually entering information” firstquantified the total value of nurses’ time nation-wide as a maximum, and thenidentified the portion of that time spent manually documenting information andprogramming devices.9
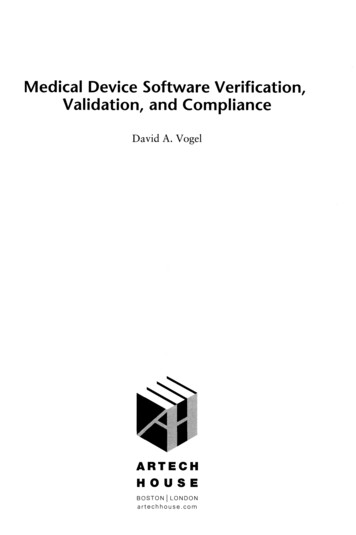
SUMMARYOFRESULTSThe potential impact of interoperable vs. non-interoperable devices was definedbased on available clinical literature. Continuing the example of “time wastedmanually entering information,” this analysis looked at the impact of medical deviceintegration on documentation and programming time in published case studiesto estimate the reduction in waste. Where an exact case study of medical deviceinteroperability was not available, a surrogate analysis was selected based on itsrelationship to the activities interoperability would address. For example, “increasedlength of stay from delays in information transfer,” used the impact of anotherintervention that decreased test turnaround time - point of care testing - to estimatethe impact of medical device interoperability on emergency department (ED) lengthof stay.Figure 2: Estimated Addressable WasteEstimated Waste from Lack of Medical Device Interoperability ( M) 40,000 17,800 35,100Increasedlength of stayfrom delays ininformationTOTAL 30,000 20,000 12,300 10,000 3,000 2,000Adverse eventsavoidable withinteroperabilitySummary of ResultsThe analysis identified an estimated 36 billion in potential, annual addressable wasteacross segments of health care in the U.S. (Figure 2). The bulk of this waste (97percent) relates to the lack of interoperability itself, with the remainder coming fromthe lack of commonly implemented standards. While a lack of commonly adoptedstandards for medical device interoperability may result in a small amount of directsavings, it has the ability to facilitate a more rapid adoption of interoperability, whichcan achieve the benefits described below.SUMMARYOFRESULTSDEFINTION AND QUANITIFICATION OF THE SHAREOF COSTS ADDRESSABLE BY INTEROPERABILITYRedundanttesting resultingfrom inaccessibleinformationTime spentmanuallyenteringinformationEstimated Waste from Lack of Commonly Adopted Standards ( M) 10,000 430Device developmentand testing costs 740 1,170Provider costs tointegrate deviceswith EHRsTOTAL*Note: Numbers rounded for clarityThe benefits from interoperability arise from four primary activities:1) quality improvement through reduction of adverse events due tosafety interlocks ( 2 billion)2) reduced cost of care secondary to avoidance of redundant testing( 3 billion)3) increased clinician productivity secondary to decreased timespent manually entering information ( 12 billion)4) increased capacity for treatement secondary to shortening lengthof stay ( 18 billion)For waste due to lack of medical device interoperability, the majority of benefits (93percent) accrue to providers, followed by payers (6 percent), with initially de minimisdirect economic benefit to patients. Additionally, device manufacturers and healthIT companies are expected to gain little from medical device interoperability (Figure3). It is important to note that differences in reimbursement policies make it difficultto precisely allocate the magnitude of benefits to each stakeholder; therefore theallocation provided below represents a reasonable estimation and allocation of thosebenefits. Furthermore, as patients are being asked to bear greater responsibility forthe entirety of their medical costs, the savings initially attributed to providers andpayors will necessarily decrease overall costs with likely proportional patient savings.Benefits from common adoption of standards include reduced costs for medical devicedevelopment and systems integration within a health system.10The Value of Medical Device InteroperabilityWest Health Institute11
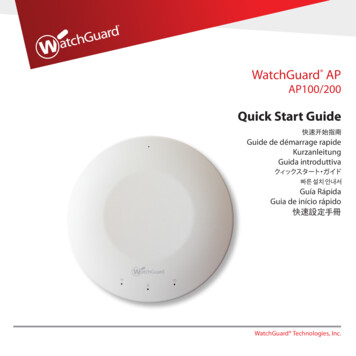
SUMMARYOFRESULTSAreas of Waste due to Lack ofMedical Device InteroperabilityDetailed FindingsLACK OF MEDICAL DEVICE INTEROPERABILITYShare of Total ( M)Providers PayersPatients DeviceVendorsDue to Lack of Medical Device Interoperability 1,000 850 1502. Redundant testing resulting from inaccessibleinformation 1,500 1,275 225 32,600 2,125 375 093%6%1%0%3. Clinician time spent manually enteringinformation 12,3004. Increased length of stay from delays ininformation transfer 17,800Total Savings (%)Costs Resulting from Avoidable Adverse Events: 2 billionMedical errors result in as many as three million preventable adverse events each year,driving as much as 17 billion in excess annual medical costs and as many as 98,000deaths per year.9, 10 Several of the most common causes of medical errors can besubstantially addressed by improved medical device interoperability, including drugerrors (accounting for 20 percent of adverse events), diagnostic errors (17 percent)and failure to prevent injury (12 percent).9,10 Errors in technique, accounting for 44percent, are assumed to be largely unaddressable by improved interoperability.101. Adverse events associated with medical deviceinteroperabilityTotal Savings ( M)DETAILEDFINDINGSFigure 3: Savings by Stakeholder from Increased MedicalDevice InteroperabilityDrug ErrorsWith and without Medical Device Interoperability*Note: Numbers rounded for clarityFor waste related to the lack of commonly adopted standards, the allocation of coststhat could be eliminated was based upon interviews of stakeholders, whose viewsvaried significantly, and was therefore a reasonable estimate based upon variousexpert opinions about how those costs are borne today (Figure 4).Figure 4: Maximum Potential Savings by Stakeholder due toLack of Commonly Adopted StandardsShare of Total ( M)Areas of Waste due to Lack ofCommonly Adopted StandardsProviders PayersPatientsDeviceVendorsDue to Lack of Medical Device Interoperability5. Device testing and development costs6. Provider costs to integrate devices with EHRsTotal Savings ( M)Total Savings (%) 430 740 740 43063%37%Medication errors can stem from errors in drug ordering by the physician, ordertranscription by various clinicians, drug dispensing by the pharmacist and drugadministration at the point of care (Figure 5).Medical device interoperability will facilitate the push of test results and vital signsreadings to clinicians or pharmacists and automate the integration of relevantinformation to inform ordering decisions, thus avoiding ordering errors stemming fromlack of patient information or inadequate monitoring. Interoperability can addresstranscription and administrative errors by allowing EHRs, physiological monitoringdevices and medication administration devices to communicate in a seamless manner.Automation of these activities and functions with medical device interoperabilitycan 1) enable automatic population of drug orders into the devices that administerthese drugs, 2) transfer alerts and parameters for drug delivery from an EHR into thedevice and 3) provide a physiological data feed into the device. Any one of theseinterventions can reduce drug-related adverse events. For example, the integrationof intelligent infusion devices, bar-code-assisted medication administration andelectronic medication administration records has been found to reduce errors furtherthan using these systems in a siloed manner, as it enables the automatic populationof provider-ordered, pharmacist-validated infusion variables directly into the infusiondevice, which verifies the dose and rate against dosing limits defined in the druglibrary (Medical device interoperability would not address any pharmacy dispensingerrors beyond those that stem from errors in transcription or ordering).*Note: Numbers rounded for clarity12The Value of Medical Device InteroperabilityWest Health Institute13
DETAILEDFINDINGSCalculationsAccording to a study in Health Affairs, adverse drug events result in an estimated 3.8 billion in incremental medical costs annually.9 Ordering errors account for 39percent of all drug errors.11 There are few studies specifically examining the impact ofinteroperability on ordering errors, but a relevant proxy is the impact of closed-loope-prescribing, automated dispensing, bar-code and eMAR systems, as such closedloop systems achieve their benefits by integrating the flow of information among thesubsystems which comprise them. A study in Quality & Safety in Healthcare foundthat such a closed-loop system reduced prescribing errors by 47 percent.12Transcription errors account for 12 percent of all drug errors;11 these errors can beaddressed for all types of dosage forms, as interoperability between automateddispensing devices and computerized physician order entry (CPOE) systems canaddress errors for intravenous (IV) and non-intravenous drugs alike. There are fewstudies on the impact of interoperability between automated dispensing machinesand CPOE systems specifically, but the impact of integrating bar-code medicationverification with an electronic medication administration system can be used as aproxy, as the latter reduces transcription errors through a similar mechanism: byimporting orders electronically from the physician’s order entry or pharmacy system.Studies have found that this reduces between 5013 and 100 percent11 of transcriptionerrors, so an average value of 75 percent is used.Administration errors account for 38 percent of all drug errors.11 Because themechanism for error reduction is specific to IV interoperability, the proportionof addressable errors is limited to the 60 percent that are due to intravenouslyadministered medications.14 A study in the American Journal of Health-SystemPharmacy found that IV interoperability resulted in a 32 percent reduction in reportedmonthly errors involving IV administration of heparin,15 which was used as a proxy forthe impact of interoperability on intravenously administered drug errors as a whole,given that the mechanism by which interoperability addresses such errors is notspecific to any particular drug.Based on these assumptions, potential drug error-related savings from medicaldevice interoperability were estimated at more than 1.3 billion annually, or 8 percentof the 17 billion total cost of preventable adverse events.Diagnostic ErrorsWith and without Medical Device InteroperabilityDiagnostic errors result from a variety of root causes, such as a failure to accountfor symptoms, order appropriate tests and consider all relevant diagnoses. Medical14The Value of Medical Device InteroperabilityWest Health InstituteDETAILEDFINDINGSFigure 5: Case Study:Drug Errors60Current State:70A cancer patient’s pain is managed withpatient-controlled analgesia (PCA)and has a physician order for arelatively low constant infusion rateof analgesia, with an intermittentlyhigh rate available when requestedby the patient. As the infusion pumpis being programmed, thesetwo rates are reversed, resultingin over-sedation and respiratorydepression. The patient’s monitor1 mg/hour8 mg dolus8mg/hour1mg bolus1demonstrates droppingpulse oximetry, but vention is delayed untilthe nurse walks back into room,resulting in anoxic brain injury.Future State:1 mg/hourIf the PCA pump were able tocommunicate with computerizedphysician order entry, transcriptionand infusion errors couldbe avoided. If the physiologicalmonitoring device communicatedwith the pump, drug infusionwould automatically be discontinuedwhen physiological parameters moveoutside a predetermined range.8 mg dolus1mg/hour8mg bolus1234567890.EnterClearStart/StopHistory15
Missed Diagnoses 72 hoursCurrent State:80809595120120Joanne Callen and colleagues found that 16.5 percent of missed EmergencyDepartment (ED) diagnoses that harmed patients were due to a breakdown at thestep of transmitting test results to the provider.16 This was applied here as a proxy forthe improvement that could be realized by medical device interoperability facilitatingthe immediate “push” of test results to the EHR so that the care provider has theright information to make appropriate diagnoses.abnormal heart rhythm basedon bedside monitoring.The printed heart rhythm strip isreviewed by an ER physician,who admits the patient for observationand cardiology consultation.The next day, a cardiologist seesthe patient, but the diagnosticBased on this assumption, as well as the aforementioned estimates for the costsof preventable adverse events ( 16.6 billion) and the percentage due to diagnosticerrors (17 percent), it was estimated that interoperability could result in nearly 466million in annual savings related to addressing diagnostic errors, about 3 percent ofthe total cost of preventable adverse events.?rhythm strip in unavailable.Repeated ECGs are non-diagnostic.Additional testing is undertaken toreproduce the arrhythmia, all withouteffect. The patient is dischargedwithout intervention, and returns in72 hours with worsening symptoms.Failure to Prevent InjuryWith and without Medical Device Interoperability“Failure to prevent injury” encompasses a variety of potentially preventableconditions. A primary example is ventilator-associated pneumonia; interoperabilitycan reduce its incidence by automating and facilitating the monitoring ofphysiological parameters and matching the ventilator support needed by individualpatients (Figure 7). This is particularly important for managing ICU patientswith dynamic vital signs and lung capacity in accordance with best practiceguidelines. Interoperability supports clinicians in performing frequent “ready towean” assessments, which leads to fewer ventilator days and thus fewer cases ofpneumonia.Future State:Automated push of information tothe EHR would save an electronicversion of heart rhythm monitoringresults and present it to thecardiologist at the appropriatetime, enabling the correctdiagnosis and treatment.8095120Postoperative shock can also be addressed by improved interoperability, asintegrating continuous vital signs monitoring with alarm systems has been shown toreduce its incidence by allowing earlier intervention in patients whose condition isdeteriorating.ECGreceivedThe Value of Medical Device InteroperabilityWest Health Institutedevice interoperability can reduce such errors by making symptom readings availablein real time and pushing test results to a care provider in a timely and clear manner(Figure 6).CalculationsA 35 year-old male presents to theEmergency Department withweakness. A nurse notes an16DETAILEDFINDINGSFigure 6: Case Study:Calculations80 95 120A study in Quality & Safety in Health Care found that the incidence of ventilatorassociated pneumonia decreased by 57 percent in response to a bundle ofinterventions, which included the examination of a number
interoperability would enable clinical medical devices to communicate in a consistent, predictable and reliable way. By allowing for the exchange of data with other medical devices and with patient data sources and repositories, such as EHRs, medical device interoperability would enhance the function of the systems and devices.