Transcription
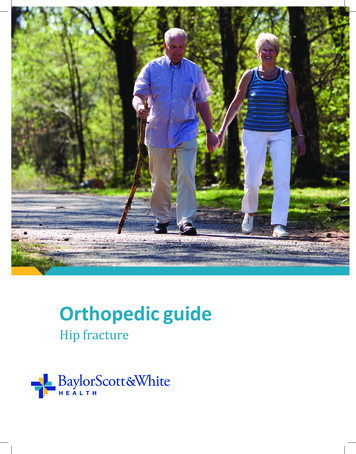
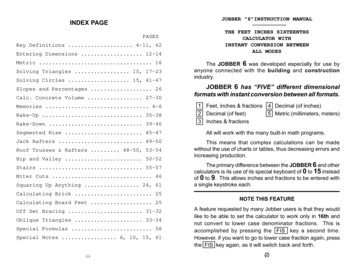
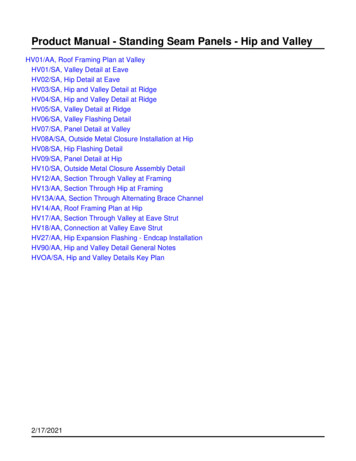
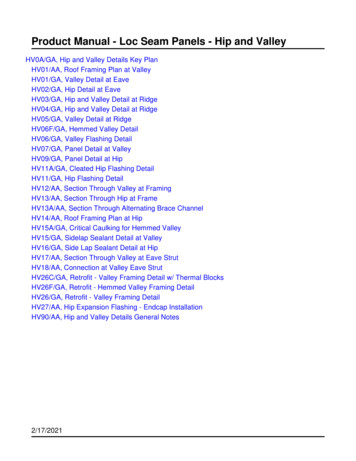
U W H E A LT H S P O R T S R E H A B I L I T A T I O NRehabilitation Guidelines for Surgical HipDislocationThe hip joint is composed of thefemur (the thigh bone) and theacetabulum (the socket which isfrom the three pelvic bones). Thehip joint is a ball and socket jointthat not only allows flexion andextension, but also rotation of thethigh and leg (Figure 1). The headof the femur is encased by the bonysocket in addition to a strong, noncompliant joint capsule, makingthe hip an extremely stable joint.Because the hip is responsible fortransmitting the weight of the upperbody to the lower extremities andthe forces of weight bearing fromthe foot back up through the pelvis,the joint is subjected to substantialforces. Walking transmits 1.3 to5.8 times body weight through thejoint, and running and jumping cangenerate forces across the joint equalto 6 to 8 times body weight.Lunate surface of acetabulumArticular cartilageAnterior superior iliac spineAnterior inferior iliac spineHead of femurIliopubic eminenceAcetabular labrum(fibrocartilainous)Greater trochanterFat in acetabular fossa(covered by synovial)Neck of femurObturator arteryAnterior branch ofobturator arteryIntertrochanteric linePosterior branch ofobturator arteryIschial tuberosityRound ligament(ligamentum capitis)Lesser trochanterObturator membraneAcetabular arteryTransverseacetabular ligamentFigure 1 Hip joint (opened) lateral viewBoth the head of the femur andthe bony acetabulum are coveredwith articular cartilage to aide inabsorbing weightbearing forcesthrough the joint (the gray materialin Figure 1).The acetabular labrum is a circular,fibrocartilaginous structure thatsurrounds the socket. It functions toseal the joint enhance stability, andprovide proprioceptive feedback(a sense of joint position) to thebrain and central nervous system.The labrum acts as a suction seal orgasket for the hip joint. This helpsto maintain the hydrostatic pressurethat protects the articular cartilageFigure 2: Frog leg radiograph: The thin arrow on your left indicates the area of “flattening” of theright femoral head and lack of the normal femoral head-neck offset. The thick arrow on the rightindicates the more normal, rounded contour of the left femoral head.The world class health care teamfor the UW Badgers and proudsponsor of UW AthleticsUWSPORTSMEDICINE.ORG621 SCIENCE DRIVE MADISON, WI 53711 4 6 0 2 E A S T PA R K B LV D . M A D I S O N , W I 5 3 7 1 8
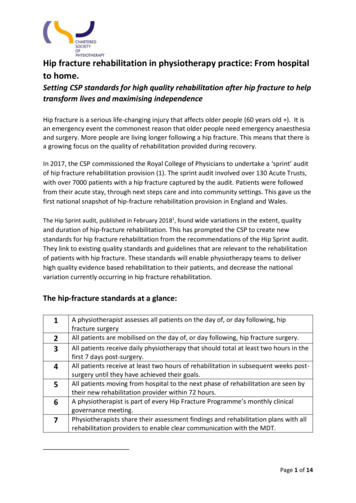
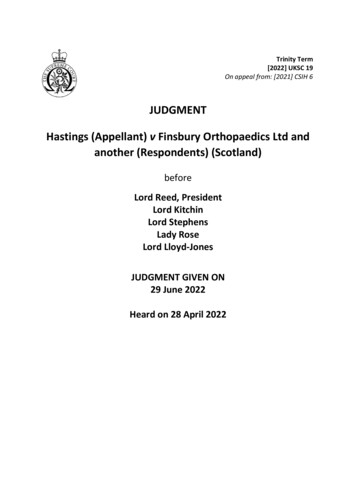
Rehabilitation Guidelines for Surgical Hip DislocationFigure 3: A defect in the subchondral bonewas too large for microfracture so it wasreshaped allowing a bone plug to be placedFigure 4: A harvest bone plug with overlyingarticular cartilage fit into the cartilage defectFigure 5: The plug has been brought even withthe rest of the articular surfaceon the head of the femur and theacetabulum.using long arthroscopic instrumentsinserted in to the hip. This includeslabral tearing where some of thelabrum has been absorbed or brokenoff so there is not enough tissue fora repair. These patients may need alabral reconstruction that is best doneif the hip is surgically dislocated first.The surgical hip dislocation involvesseparating a piece of bone from thegreater trochanter (the upper part ofthe thigh bone) which is referred toas a greater trochanteric osteotomy(figure 8). By using this approach, thesurgeon can safely dislocate the hipwhile protecting its blood supply andpreserving key muscle attachmentsaround the joint. The surgeon is thenable to fully visualize and correctabnormalities of bone and soft tissuesabout the hip joint. Before closing theincision, the separated bone fragmentis reattached with screws to maintainalignment and stability as healingoccurs. (Figure 8)Hip joints of athletes are exposedto extremes of motion. These forcesare absorbed by and can injure thelabrum by impingement of the hip.This is referred to as femoroacetabularImpingement (FAI). FAI can occurfrom change
4. There are precautions that need to be followed to reduce chances of dislocation of the hip during the early recovery phase. No hip rotation or excessively turning toes either outwards or inwards by rotating the entire leg. Hip flexion needs to be limited to 75 for the first 4 weeks, then can be 90 until 6 weeks out. 5.