Transcription
Pathophysiology of PainRamon Go MDAssistant Professor Anesthesiology and Pain medicineNYP-CUMC
Learning ObjectivesAnatomic pathway of nociceptionDiscuss the multiple target sites ofpharmacological agentsLearn risk factors for the development ofchronic painUtilize information to treat pain atmultiple target sites
What is pain?"an unpleasant sensory andemotional experience associated withactual or potential tissue damage”
Anatomy of thePain PathwayTransduction: Conversion of a noxious stimuli(chemical, mechanical, or thermal) intoelectrical energyTransmission: Electrical stimulus is sent to thedorsal horn of the spinal cord and synapse atthe 2nd order neuronModulation: Inhibition vs amplification of signal(facilitated by EAA)Perception: Conscious awareness of pain as aculmination of previous processes in thecontext of the individuals experiences.
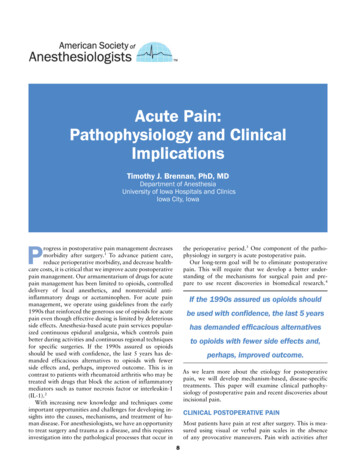
A closer lookTransduction: Primary afferentsSkinSpineNerve FiberFunctionA-betalow threshold mechanoreceptorsA-deltalow threshold mechano and thermoreceptorsChigh threshold thermal, mechano, and chemicalreceptors
Transduction: Primary afferentsInflammatory SoupMast cells andNeutrophils: ATP,bradykinin, PGE2,Na , H , serotoninCOX-2 activationMacrophage: NGF,IL-6, TNFaC-fibers: CGRP,Substance P,neurokinin
Transduction: Primary afferentsUp-regulation ofsubstance PEnzyme activationTRPV activationIncreased excitabilityof nociceptorsActivation of silentnociceptors
Transduction: Primary afferentsNaked mole rat: Inability to convert capsaicin and acidstimulus to electrical signal
Transduction: Primary afferentsNGF/TRKA Pathway: Activates TRPV1 ion channel allowsdepolarization and activation of voltage gated Na channels
Transmission: Electrical stimulus is sent to the dorsal horn of the spinalcord and synapse at the 2nd order neuron
Transmission: Electrical stimulus is sent to the dorsal horn of the spinalcord and synapse at the 2nd order neuron
Transmission: C fiber activity increases Wide DynamicRange Neurons firing
Modulation: Inhibition vs amplification of tory:SerotoninNEGABA
Perception: Conscious Awareness of PainCortical:Somatosensorycortex, insula, andanterior mygdala,hippocampus
When the norm diverges.
When acute pain turns to chronic.
Surgical procedures and prevalence rates of developing postsurgical pain syndromeProcedurePrevalenceBreast 1%Limb Amputation5‐50%Hip7‐13%Laparoscopic HerniaRepair15% at nine months
Allan Gottschalk, M.D., Ph.D.; Srinivasa N. Raja, M.D.
Abnormal Transmission of PainGottschalk et al 2001
Changes to the pain pathway in chronic painTransductionSustained increase innociceptors.Activation of TRPV1-RIncrease in sP and CGRPTransmissionNMDA-R activationModulationWind-upDecreased inhibitionvsIncreased amplificationWDR-Neurons sproutabnormal connectionsLoss of pain filteringActivation of glial cellsIncreased release of paintransmittersCentral sensitizationPerceptionGray matter decrease(reversible)Increased connections:Medial Prefrontal Cortex(mPFC) and NucleusAccumbens
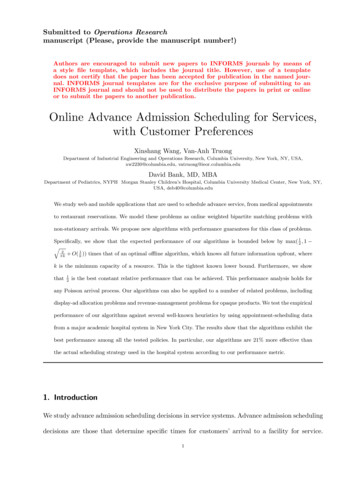
Risk Factors for acute pain to become chronic.8]TI SJ 7YVKIV]Higher preop and postop painscores, increases risk for CPSP4VIST 4EMRChronicPain IRIXMGW2 IVZI -RNYV]ࢸ
Risk Factors for acute pain to become chronic.Extensive surgery, long surgicaltime, radiation and chemotherapy.8]TI SJ 7YVKIV]Higher preop and postop painscores, increases risk for CPSP4VIST 4EMRChronicPain IRIXMGW2 IVZI -RNYV]ࢸ
Risk Factors for acute pain to become chronic.Extensive surgery, long surgicaltime, radiation and chemotherapy.8]TI SJ 7YVKIV]Higher preop and postop painscores, increases risk for CPSP4VIST 4EMRChronicPain IRIXMGW2 IVZI -RNYV]ࢸPerioperative anxiety, paincatastrophizing, excessive empathyfrom family.
Risk Factors for acute pain to become chronic.Extensive surgery, long surgicaltime, radiation and chemotherapy.8]TI SJ 7YVKIV]Higher preop and postop painscores, increases risk for CPSP4VIST 4EMRChronicPainࢸPerioperative anxiety, paincatastrophizing, excessive empathyfrom family.Surgical ProcedureNerve InjuredMastectomyLateral pectoral, medial pectoral,intercostalThoracotomyIntercostalCesarean sectionIlioinguinal, iliohypogastricHerniorrhaphyIlioinguinal IRIXMGW2 IVZI -RNYV]
Risk Factors for acute pain to become chronic.Extensive surgery, long surgicaltime, radiation and chemotherapy.8]TI SJ 7YVKIV]Higher preop and postop painscores, increases risk for CPSP4VIST 4EMRChronicPainMay explain 70% of pain variabilityࢸPerioperative anxiety, paincatastrophizing, excessive empathyfrom family.Surgical ProcedureNerve InjuredMastectomyLateral pectoral, medial pectoral,intercostalThoracotomyIntercostalCesarean sectionIlioinguinal, iliohypogastricHerniorrhaphyIlioinguinal IRIXMGW2 IVZI -RNYV]
Genetic polymorphisms result in altered nociceptionGenetics may explain 70% of variability in experiencing painSCN9A Gene: Nav1.7NormalPainPerception“No pain”“Man on Fire Syndrome”
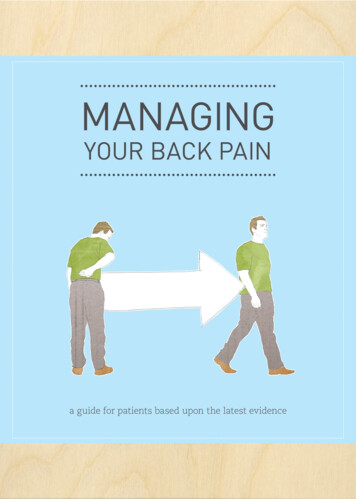
Increased Pain SensitivityGeneProtein affectedPhenotypeKCNS1Voltage gated potassium ion channelIncrease sciatica pain and phantom limb painSCN9AVoltage gated sodium ion channelChronic burning pain, phantom limb painADRB2Beta-2-adrenergic receptorRisk for widespread body painIL6Interleukin 6Pain from endometriosisCACNG2Voltage-gated calcium ion channelPost mastectomy painHTR2ASerotonin receptorIncreased post-surgical painDecreased Pain SensitivityGeneProtein ecreased or increased pain perceptionOPRM1OPRM1: opioid receptor mu 1Decreased pain perceptionTRPV1Transient receptor potential vanilloid 1Decreased thermal pain sensitivityMC1RMelanocortin 1 receptorDecreased pain perceptionGCH1GTP cyclohydrolaseDecreased post-surgical painCACNA2D3Voltage-gated calcium ion channelDecreased thermal pain sensitivity
SummaryNormal Pain ionWhen acute becomeschronic painRates of chronic painAbnormal changes in the painpathwayRF for acute to chronic painGenetics in pain pathway
Thank you for you attention!
KCNS1 Voltage gated potassium ion channel Increase sciatica pain and phantom limb pain SCN9A Voltage gated sodium ion channel Chronic burning pain, phantom limb pain ADRB2 Beta-2-adrenergic receptor Risk for widespread body pain IL6 Interleukin 6 Pain from endometriosis CACNG2 Voltage-gated calcium ion channel Post mastectomy pain