Transcription
ERGONOMICS GUIDELINES OR OCCUPATIONAL HEALTH PRACTICE IN F INDUSTRIALLY DEVELOPING COUNTRIES
SPONSORSInternational Commission on Occupational HealthConsultants in Occupational Health Safety and Risk ManagementInstitute for Science of LabourThe printing of the Guidelines has beenfinancially supported by ergonomia andIAD the Institute for Ergonomics at theUniversity of Darmstadt (Germany).ISBN 978-3-935089-16-3 IEA and ICOH 2010All rights reserved. No part of this publication may bereproduced, stored in a retrieval system, or transmittedin any form or by any means, electronic, mechanical,photocopying, recording or otherwise, without priorpermission of the copyright owners.ContactsInternational ErgonomicsAssociation (IEA)http://www.iea.ccInternational Commissionon Occupational Health http://www.icohweb.org2ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
AcknowledgementsKazutaka KogiThe authors are very grateful for the support of theInternational Ergonomics Association (IEA), theInternational Commission on Occupational Health(ICOH), the Institute for the Science of Labour in Japanand the Jim Knowles Group in Australia for theirfinancial support.Kazutaka Kogi, Research Adviser of the Institute forScience of Labour (ISL) in Kawasaki, Japan, graduatedfrom the University of Tokyo, Faculty of Medicine in1957. He conducted applied research at this Instituteuntil 1983 when he joined the International LabourOffice as Regional Adviser for Asia and the Pacific,stationed in Bangkok. During 1988-1993, he workedat the ILO headquarters in Geneva as Chief of theOccupational Safety and Health Branch and Director ofthe Working Conditions and Environment Department.He then served as Director of the Institute for Science ofLabour during 1993-1999.We are also indebted to Cara Gray for the design ofthe Handbook and many of the illustrations; extremelygrateful to Tom Leamon and Hal Hendrick (IEA) andToru Itani and Veikko Louhevarra (ICOH) for reviewingthe final draft and giving us such valuable feedback.Pat Scott, Kazutaka Kogi and Barbara McPheeAugust 2009About the authorsPat ScottPat Scott is Emeritus Professor of Ergonomics atRhodes University where she was on the staff for 27years. In 1996, as Head of the department, she startedthe first-full time Ergonomics degree programmein South Africa; a programme including bothundergraduate and postgraduate students, and hassupervised over 20 postgraduate ergonomics students.She is author of over 150 papers and chapters inbooks, and is editor of the book “Ergonomics indeveloping regions: needs and applications”, coveringthe good work being done in IDCs and which hasrecently been published.Pat was a founder member of the Ergonomics Societyof South Africa, and she has served as both Secretaryand Chairperson of the society. As Chief editor of theJournal “Ergonomics: SA” for 12 years, she canvassedpapers from Industrially Developing Countries worldwide in an attempt to encourage those who are doingsuch good work in IDCs to publish their research andshare their experiences with others.In 1997, as an executive member of the IEA, shewas appointed Chairperson of the IEA’s StandingCommittee for Ergonomics in IDCs, a positionshe held for two terms. During this time shetravelled extensively to developing countries givingpresentations and running ergonomics workshops.Pat is a Fellow of the IEA and ESSA, and in 2003 wasthe recipient of the IEA award for the Promotionof Ergonomics in IDCs. In 2007 she received theDistinguished International Colleague award of theHFES in recognition of her work in IDCs.His major areas of interest are workload and fatigueassessment and practical improvement of workplaceconditions including participatory ergonomics. Workingin technical cooperation projects for developingcountries, he has contributed to the development ofparticipatory training for workplace improvements insmall enterprises and in agriculture. He is particularlyinterested in the application of cost-effective safety andhealth measures including low-cost solutions.He contributed to the editing of Ergonomic Checkpoints,a joint publication of the ILO and the InternationalErgonomics Association. He was Treasurer of the IEAduring 1997-2003. He has served on the InternationalCommission on Occupational Heath (ICOH) as BoardMember from 2000-2006. In 2006 he was elected VicePresident of ICOH. In 2009 he was elected President.Barbara McPheeBarbara McPhee is a Certified ProfessionalErgonomist and Specialist Occupational HealthPhysiotherapist who has worked in occupationalhealth and safety for over 30 years as a consultant,teacher and researcher most particularly inergonomics. During this time she has worked in allaspects of the field at every level of industry andgovernment throughout Australia and overseas.Over the last 15 years she has worked mainly in miningconcentrating on reducing risks to employees’ healthand safety through improved ergonomics design. Shealso provides specialised ergonomics advice to clientsin a range of other industries including light and heavymanufacturing, aviation, retail food and government.Barbara is a Past President and Fellow of the HumanFactors and Ergonomics Society of Australia. Sheis an Executive Council Member of the Pan PacificCouncil on Occupational Ergonomics and is a formerBoard Member of the International Commission onOccupational Health. She is a Life Member of theAustralian Physiotherapy Association and a Fellow ofthe Australian College of Physiotherapists. She wasrecently appointed by the NSW Minister for PrimaryIndustries as an Independent Expert in ergonomicsand occupational health on the NSW Mine SafetyAdvisory Council.3
4ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
CONTENTSINTRODUCTION60.1 AIMS OF THE GUIDELINES100.2 ERGONOMICS AND ITS PRACTICE120.3 IDENTIFYING WORKPLACE PROBLEMS220.4 RISK MANAGEMENT IN THE WORKPLACE280.5 PLANNING AND IMPLEMENTINGWORKPLACE IMPROVEMENTS38 0.6 USEFUL TOOLS FOR IMPLEMENTINGWORKPLACE IMPROVEMENTS46 0.7 TWO HUNDRED PRINCIPLES OFOCCUPATIONAL ERGONOMICS58 0.8 GLOSSARY OF TERMS880.9 SOURCES OF USEFUL INFORMATION965
Representatives of the InternationalCommission on OccupationalHealth (ICOH) and the InternationalErgonomics Association (IEA) havejointly compiled these guidelines.They are designed to assistpersonnel in the field of occupationalhealth who have a limited knowledgeof ergonomics. They outline theprocess of identifying, assessingand controlling problems related tohealth and safety in the workplace.The ultimate aim is that they canprovide assistance in planning basicintervention strategies based onsound ergonomics principles.6ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
INTRODUCTIONHistory of co-operation between the IEA and ICOHIn 1996 ICOH and the IEA signed a Memorandum of Understanding (MOU) which outlined ways inwhich the two organisations could work together to enhance the impact of their activities. One ofthe points in the MOU was that both organisations would explore the possibilities of co-operationin promoting the advancement of occupational health and ergonomics in industrially developingand economically emerging countries, referred to here as IDCs.At the IEA’s triennial international congress in San Diego in July/August 2000, a small grouprepresenting the IEA and ICOH met to discuss how to implement this project. Those participatingwere: Jean-Francois Caillard, then President of ICOH, Kazutaka Kogi and Pat Scott, thenMembers of the IEA Executive and Barbara McPhee, then a Member of the Board of ICOH. Thegroup agreed that, at this time, the most effective method for promoting ergonomics to nonprofessional ergonomists would be to develop basic guidelines on the practice of ergonomics forpersonnel in occupational health fields.7
Occupational HealthIn 1950, a joint Committee of the International Labour Organisation and WorldHealth Organisation defined Occupational Health (objectives) as the: Promotion and maintenance of the highest degree of physical, mentaland social well-being of workers in all occupations Prevention among workers of departures from health caused by theirworking conditions Protection of workers in their employment from risks resulting fromfactors adverse to health Placing and the maintenance of workers in an occupational environmentadapted to their physical and mental needsTherefore Occupational Health services deal with:1. Health promotion and maintenance (Primary Prevention or well people care)2. Prevention of disease and injury, or workers’ return to full work dutiesafter injury or illness (Secondary Prevention or threatened people care)3. Some treatment or workplace modification for residual disability (TertiaryPrevention or sick people care)The workplace affords the best community opportunity for health promotion andmaintenance in working adults.Ergonomics is an essential and integral element of occupational health practice.8ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
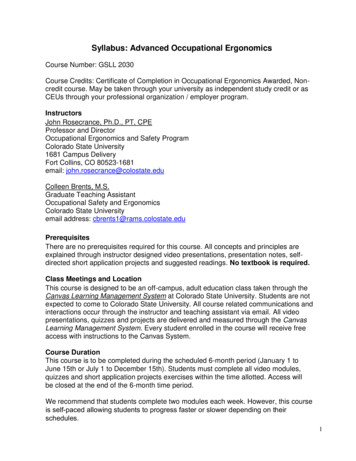
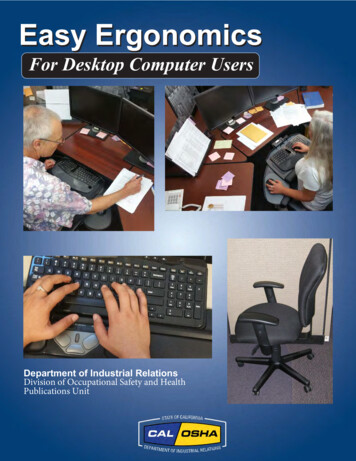
Ergonomics for occupationalhealth practiceAt the workplace, ergonomics is applied tothe design of work equipment and tasks andto work organisation. It is often referred to asoccupational ergonomics as it is an importantpart of occupational health and safety. Assuch, it aims to promote health, efficiency andwell-being in employees by designing for safe,satisfying and productive work.Ergonomics can play an important role inoccupational health and safety managementwhere the primary aim is to reduce risks ofinjury or disease while enhancing the quality ofworking life. Good ergonomics in the workplacecan improve productivity and morale of workersand decrease injuries, sick leave, staff turnoverand absenteeism.In occupational ergonomics it is necessary toexamine not only the physical design aspectsof work or the ‘hardware’, but also areas suchas work organisation and task design, jobcontent and control over workload, supportand training. The social and managerialenvironment is important. Usually theseaspects require ergonomics to be integratedinto the broader work systems.Therefore to determine if an optimum solutionhas been achieved, the people who performthe work (the ‘who’), the nature of the tasks(the ‘what’) and the context in which they aredone (the ‘where’, ‘when’ and the ‘how’) needto be considered. This integrated approachin applying ergonomics will be beneficial forimproving occupational health practice in IDCs.OrganisationalfactorsPhysical & mentaljob demandsPsychosocialfactorsWorker capabilitiesand limitationsIMBALANCE (mental and/or physical strain)BALANCE Decreased productivity Increased absenteeism Increased staff turnover Increased injury and accident rates Increased error rates and quality problemsNO ACTIONACTIONChronic problemor shutdownof operationAchieving change.Recovery (individualand/or organisation)Figure 1 P hysical, mental and psychosocial factors influencing workers’ health.From Aickin, Lusted and McPhee 2009There is strong evidence to suggest that the problemsassociated with the sub-optimal working conditions soprevalent in IDCs are getting worse despite extensiveisolated efforts to improve working conditions.It is therefore imperative that we establish a collaborativedrive to address an area of common concern to us all thatis: the health, safety and well-being of the worker.9
0.1 AIMS OF THE GUIDELINESWe have compiled these Guidelines to help occupational health personnel inindustrially developing countries (IDCs). Most particularly they are intended forthose who may be active in the field of health at work and who do not have formalqualifications or training in ergonomics. The Guidelines aim to provide informationabout the process of identifying and rectifying basic problems associated withsuboptimal working conditions by applying ergonomics.In order to apply ergonomics, we therefore need information about the: Human operator Task Overall work setting including equipment, environment and the organisation of the workHow these elements interact and allow for a good match between workers and theirjobs is one of the aims of occupational ergonomics. The other aim is to correct anymismatches so that they do not cause adverse effects such as illness or injury, humanerror or reduced productivity.The word ‘optimum’ is used in ergonomics to refer to the balancing of the abilities ofpeople with the demands of work. This requires careful observation and discussionwith workers as well as using any information to hand such as accident, injury andillness statistics, data on productivity and reworking product.Local solutions for local problemsThere are some generic guidelines produced for general needs but in reality workplaceproblems may vary substantially from site to site and even department to department.Some ergonomics solutions do not to transfer directly from one industry to another, letalone between different regions or countries. Each set of circumstances is different.10 ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
Therefore, to be successful every ergonomicsassessment must take into account the socioeconomic context ensuring that the solutionsare appropriate and acceptable to the localsituation. It can be described as ‘the way we dothings around here’ and relates to the culture ofthe country and the industry and/or company inthat country. Simply importing solutions withoutreference to local issues and resources is verylikely to fail; modifications to imported solutionsare generally necessary.Target groups for these GuidelinesIn most IDCs there is very limited knowledgeabout ergonomics and there are very fewqualified Ergonomists. However, there areoften people trained and involved in varioussub-sections of occupational health and safety(OHS). While the expertise may differ there aremany important common areas of concern, themost important of which is for the well-being ofthe worker.The IEA and ICOH take the view that the lack ofpersonnel formally trained in ergonomics shouldnot be a barrier to the application of basicergonomics principles in the workplace. TheseGuidelines should be useable by anyone who hasan interest in improving work conditions.Therefore, we have compiled them for peoplewithout formal ergonomics education butwho may have a basic working knowledge ofergonomics and its benefits.Professionals such as OccupationalHealth Nurses, Occupational Physicians,Physiotherapists, Occupational Hygienists andSafety Officers can promote ergonomics asthey look for opportunities to improve workingconditions. Ideally, ergonomics professionalsshould be involved in the training of the OHSpersonnel and are encouraged to help othersuse these Guidelines in their work.PrinciplesThese Guidelines concentrate on the applicationof ergonomics principles to improve workingconditions with the view to protecting andpromoting the health and safety of workingpeople. It is not a cookbook of menus to solveparticular problems. Rather it describes ageneral approach and way of thinking neededfor on-going assessment and improvements ofworking conditions in IDCs.Section 7 lists the range of areas withinoccupational ergonomics and outlines basic principles.11
0.2 ERGONOMICS AND ITS PRACTICEWhat is ergonomics?“Ergonomics is the scientific discipline concerned with the fundamentalunderstanding of interactions among humans and other elements of asystem, and the profession that applies theory, principles, data and methodsto design in order to optimise human well-being and overall systemperformance” (International Ergonomics Association (IEA), 2000).Derived from the Greek ergon (work) and nomos (laws) to denote the scienceof work, ergonomics is a systems‑oriented discipline that extends acrossall aspects of human activity, and therefore promotes a holistic approach toenhancing the well-being of people at work. To achieve this it considers thephysical, cognitive, social, organisational and environmental aspects of workand the impact, both positive and negative, that these may have on the worker.Practicing Ergonomists must have a broad understanding of the full scopeof the discipline and be able to apply the principles in practice to improveworking conditions.Domains of specialisation in ergonomicsDue to the wide scope of ergonomics, in 2000 the IEA proposed the followingthree broad domains of specialisation within ergonomics in order to establishsome clear identification of the recognised areas of the discipline.Physical ergonomics is concerned with human anatomical, anthropometric,physiological and biomechanical characteristics as they relate to physicalactivity. Relevant topics include working postures, materials handling,repetitive movements, heavy work, work-related musculoskeletal disorders,workplace layout, noise, thermal conditions and vibration, safety and health,as these relate to work.12 ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
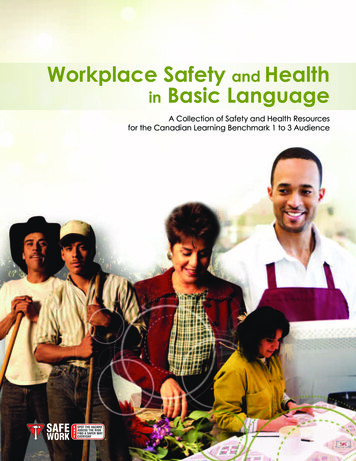
Cognitive ergonomics is concerned withmental processes, such as perception,memory, reasoning and motor response, asthey affect interactions among humans andother elements of a system. Relevant topicsinclude mental workload, decision‑making,skilled performance, human‑computerinteraction, human error, work stress andtraining as these may relate to the wayhumans work in systems.Organisational ergonomics is concerned withthe optimisation of socio‑technical systems,including their organisational structures,policies and processes. Relevant topicsinclude human system considerations incommunication, human resource management,work design, design of work schedules,teamwork, participatory design, communityergonomics, cooperative work, new workmodels, virtual organisations, tele-work andquality management.The emphasis of any ergonomics investigationmay be more in one domain than another.However, no thorough evaluation of a workplaceshould ever be exclusively in one area.The focus of ergonomics is the analyses of theinteraction between the human operator andother components within the system. If there isincompatibility between any of the elements thatmake up the overall system the risk to the healthand safety of workers increases. Any identificationof a “mismatch” between the worker and the taskneeds to be addressed by adjusting the task tosuit the capabilities of the worker.Integration of Ergonomics intoOccupational Health and Safety (OHS)The twofold objective of ergonomics is toenhance the safety and well-being of theworkers and to improve productivity. This hasobvious benefits for workers, the organisationand the nation.Enhanced workerhealth, safetyand tyFigure 2 Two fold objective of occupational ergonomics.13
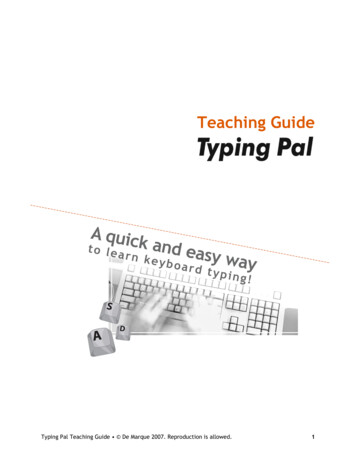
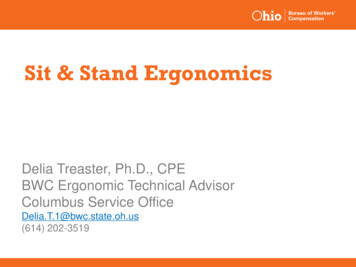
Ergonomics is well establishedin many countries. However, inIndustrially Developing Countries(IDCs) it is less well known and lesspracticed. Fortunately, there is agrowing awareness of the crucial rolethat ergonomics can play in IDCs. Itis therefore important that the fewErgonomists who are working in theseregions strive to establish “functionalpartnerships” with other professionalsinvolved in addressing the challengingproblem of improving such suboptimal working conditions.PHYSICALLY DEMANDING TASKS COMPOUNDED BY:Limited educationLow incomePoor living conditions& health issuesPoor nutritionLow work capacityPhysically demandingtasksFocus of ergonomicsErgonomics focuses on theappropriate design of workplaces,systems, equipment, work processesand environments to accommodatethe workers. The aim is to achievecompatibility between the needs ofpeople with real limitations and thedemands of their jobs. Considerationshould be given to the immediateproblem as well as the entire worksetting and beyond.Work demands need to be balancedwith social demands. For example,mothers with young children;families with sick or elderly relatives;workers who are inadequatelynourished may be more prone tooccupational injury and disease.Physically heavy work is oftenunskilled and the people employedto do it may have few options withrespect to the work that they do.Problems of poor education canbe compounded by low incomeand associated inadequate livingconditions, poor nutrition andhealth issues.MicroergonomicsMuch of ergonomics has focused onpeople working with tools, machinesLong working hoursInadequate recovery& chronic fatigueLow productivityNEGATIVE SPIRALFigure 3 T he consequences of poor education and lowincomes for workers.From Scott 2007and other equipment. This is what wecall the “human-machine” interfaceand is now often referred to asmicroergonomics.Any incompatibility between taskrequirements and the capabilities(mental and/or physical) of the workercan result in a sub-optimal situation.In turn, this may lead to errors,accidents and injuries. Workingwith employees Ergonomists canidentify and prioritise problem areasand propose possible solutions. Ifnecessary, they may recommend aredesign of the workplace, the tasksand/or the organisation of the work toaccommodate individual workers aswell as groups of workers.14 ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
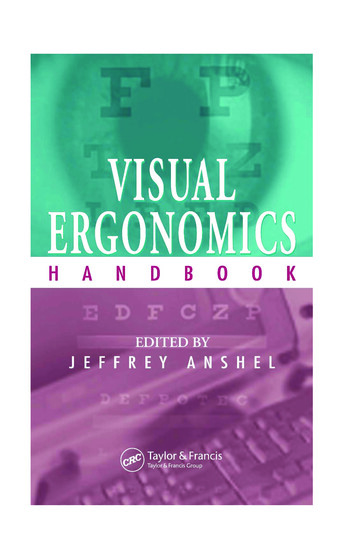
OPERATOR Handling l designOrganagement structuna(mre)Figure 4 MICRO-ERGONOMICSThe human-machine interface.From Grandjean 1988MacroergonomicsTechnTo address this problem he proposedthe concept of macroergonomics,which he defined as a “top-downsocio-technical systems approachto organisational and work-systemdesign”. Work organisation has beendefined as: the way in which all sub-systems of the workplace are coordinated, supervised and performedby each worker carrying out a specificjob within the broader system.p leology&toolsSince the 1980s Ergonomists haverecognised the need to look beyondthe obvious microergonomics issuesand to make an assessment ofthe overall working environment.Hendrick (1986) argued that while itis possible to do an outstanding jobdesigning a specific aspect within aworking system i.e. at a micro-level,an Ergonomist might fail to achieveoverall system effectiveness if there isa lack of attention to the larger pictureor the design of the complete system.oPeInterpretationdecisionMACHINEHence macroergonomics isconcerned with the optimisation oforganisational and work-systemdesign through consideration ofrelevant personnel, technological andenvironmental variables. It examinesthe interactions and interdependenceof all facets of the workingenvironment and considers the wayorganisations are managed.Externatl environmenFigure 5 M ACROERGONOMICS – Top down systems approachrecognising the need for general, overall organisationand control. Adapted from Hendrick 1998APPLICATION OF ERGONOMICS Organisational designMACROOrganisationalarrangements Facility design Job design Training/education EnvironmentMICROWorkerequipmentinterface Workstation Task design Equipment/products ToolsFigure 6 A pplication of ergonomics. From McPhee 200815
Using ergonomicsprinciples to create asafer and more efficientwork environmentThe control of risks associated with poorworking conditions is like the controllingof many other hazards in OHS in that itrequires a systematic approach and acommitment to continual improvement.Most of the ‘people’ issues relating toareas such as safety and the designof tasks, machinery, tools and worksystems require the ongoing assessmentand application of ergonomicsinvestigation and intervention. Jobrequirements, and the way in whichthey are done, are constantly changingtherefore any system needs to be flexibleand continuously monitored.The solutions to workplace problemsneed not be costly or complicated.However, they must involve a processthat systematically identifies risks,determines how important each oneis and then controls them by thebest means possible. It also involvesmonitoring the situation to ensurethat the process continues and issuccessful. The process of managingrisks is relatively easy to initiate butmust always focus on finding the rightsolution, implementing it and reviewingits effectiveness.Much ergonomics information relatingto the workplace is straight forwardrequiring the thoughtful application ofbasic principles. Often it may only benecessary to create an awareness ofthese basic principles, acknowledgesound practices which many workersalready use and encourage and rewardworker initiative.Worker participationin applying ergonomicsprinciplesEmployees should be encouraged tobecome actively involved in the processof identifying problems and to makesuggestions for improvement. Workers’experience can and should be used toplan, implement and refine changes inorder to achieve more workable solutionsfor identified problems and to prevent thelikelihood of future problems.This involvement of the workers isknown as ‘participatory ergonomics’and is widely used for disseminatingergonomics information and successfullyachieving change. It is based on thepremise that the people who do the worktend to know the best way to carry it outin practice.Participatory involvement ideallyshould include managers, workers,trade unionists, OHS personnel andsupervisors, i.e. participants from the fullspectrum of employees and employers.However, smaller groups can be just aseffective in some workplaces as long asmanagers commit to change and supportthe group’s activities.Success has been achieved withinsome organisations by forming a smallteam of committed people called an‘Ergonomics Facilitation Team’.A notice board of Ergonomics Hints andBest Practices can be used to great effectand input from all should be encouraged.A “co-operative co-responsibility” canbe developed whereby employers andemployees interact on a regular basisto discuss problems and to implementappropriate solutions.By involving a cross section of personnelwithin the company, one can create an“Ergonomics ethos” at all levels, whichcan have a positive effect on the companyas a whole.If non-ergonomics personnel identify amajor or complex problem that requiresexpert knowledge and skill they shouldseek further advice from a qualifiedprofessional Ergonomist. With thegrowth of electronic communication16 ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
such as emails and the Internetprofessional support is now moreeasily accessible for people in differentcountries and in remote locations.If this is not possible, an experiencedoutsider with some knowledge ofergonomics may be able to observethe situation from a differentperspective, with ‘fresh eyes’,making note of all the relevantfeatures of the job and the worker.Often such people can provide amore objective evaluation of hazardsand risks.Benefits of ergonomicsThe focus generally should beon simple, low-cost methods ofidentifying and solving commonproblems in workplaces withinIDCs. While the health and safetyprofessionals’ emphasis is onmaintaining and improving workers’health, safety and well-being, theapplication of ergonomics can provideother benefits. These include: Minimising wasted effort Reduced damage to equipment Less waste of product Analysis of individual taskrequirements Assessment of worker capacityand abilities Balancing task demands, bothphysical and mental, withworker capabilities Improved workplace design Enhanced overallorganisational managementCost-benefit of ergonomicsErgonomics interventions in IDCsneed to be at a minimal cost, even‘no-cost’, but they also must beeffective in alleviating the stressplaced on so many workers involvedin demanding work. (See Figures7 to 10). This in turn can assist inimproving worker efficiency and havea positive influence on cost benefitsto the company. Improved productivityIn a well-designed workplace workerscan achieve more output with lesseffort and fewer risks to their healthand safety. Good design often costsno more than poor design but, tobe effective, it does require goodorganisation and careful planning inconsultation with the workers.The benefits of ergonomics can beachieved through: Adaptations whichaccommodate local workersFigure 7 E xcessive and unnecessary reaching.17
Figure 8Heavy, awkward loads canbe much more effectivelypicked up, carried andlowered using team lifts ormechanical aids.Figure 9Fixed work postures andlack of task variety can bealleviated by regular breaksaway from the task.18 ERGONOMICS GUIDELINES FOR OCCUPATIONAL HEALTH PRACTICE IN INDUSTRIALLY DEVELOPING COUNTRIES
Figure 10 Unbalanced work posture and use of excessiveforce such as in this task can be the result of localconditions. Local solutions may be relatively easyonce the problem is acknowledged.Justifying expenditure to improve OHShas been difficult in the past. Oftendirect compensation and medicalexpenses were the only indicatorthat poor OHS practices were costly.These may not be good indicators inIDCs. However, reduced productivityand increased re-work rate are costlycompared with the costs of manysimple ergonomics changes.In those companies where thereis adequate data it is possible tocalculate the real costs of injuriesand illness to companies usingmethods and programs that areavailable commercially. These rangein complexity from full companyaccounting systems to methods thatapply to individual jobs or groups of workers.Consider the feasibility, availabilityand cost of changes needed toimprove working conditions in relationto the size and cost of the problem.Sometimes it may be necessaryto justify the cost of change, or ofdifferent changes, or the costs ofdoing nothing at all. This is whereconducting a cost-benefit or costeffectiveness analysis c
eRgonomiCs foR oCCuPational health PRaCtiCe At the workplace, ergonomics is applied to the design of work equipment and tasks and to work organisation. It is often referred to as occupational ergonomics as it is an important part of occupational health and safety. As such, it aims to promote health, efficiency and