Transcription
Tackling the Dual Economic andPublic Health Crises Causedby COVID-19 in BaltimoreEarly Lessons from theBaltimore Health Corps PilotEmbargoed until 12:01am EDT,Tuesday, April 21, 2020June 2021TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMOREI
AuthorsDylan H. Roby, Ph.D.Neil J. Sehgal, Ph.D., M.P.H.Elle Pope, M.P.H.Melvin Seale, M.A., D.HScEvan Starr, Ph.D.Department of Health Policy and ManagementHealth Systems and Policy Research LabUniversity of Maryland School of Public Healthhealthpolicy.umd.eduThis report is based on research fundedby a consortium of donorsAll views expressed are solely those of the authorsSuggested citation: Roby DH, Sehgal NJ,Pope E, Seale M, Starr E. 2021. Tackling the DualEconomic and Public Health Crises Caused by COVID19 in Baltimore: Early Lessons from the BaltimoreHealth Corps Pilot. Prepared for the Baltimore CityHealth Department by the University of MarylandHealth Systems and Policy Research Lab.University of Maryland School of Public HealthTACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE1
Table of ContentsAcknowledgmentPrefaceAcronyms and Abbreviations346ExecutiveSummaryObjectives and Early FindingsConclusions and Recommendations911BackgroundBHC's theory of changeEvidence Base Supporting the BHC Pilot ModelLocal ContextCreation of the BHC15171920Objectivesand ActivitiesIdentifying Partners for Key Functional RolesOrganizational Structure2326EarlyFindingsObjective 1 – Workforce DevelopmentOutreach, Recruitment and Application ProcessingProgress in Equitable HiringReaching Vulnerable Communities through Additional Training and EngagementResource Allocation and ConstraintsObjective 2 – Contact Tracing and Case InvestigationOnboarding New Contact TracersContact Tracing and Case InvestigationObjective 3 – Care CoordinationHiring and Training of Care CoordinatorsCare Coordination ActivitiesBarriers to Implementation272829343537383841424344Lessons LearnedConclusions45Specific Recommendations for BHC52Broad Recommendations for Developing and Implementing a Similar Program53Appendix A: BHC Funders55Appendix B: Schematic of BHC Hiring Process56Appendix C: BHC Workgroup Structure57Appendix D: Schematic of BHC Training, Performance Support, and CareerDevelopment Process59Appendix E: Jhpiego/BCHD Case Investigation and Contact Tracing Scheduleand Content for all Contact Tracing CHW, Supervisors, and Managers60Appendix F: Methodology61Appendix G: Learning Questions63ReferencesTACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE642
AcknowledgmentsThe authors thank the Baltimore Health Corps management board, leadership team, and staff for theirsupport in conducting this work. The BaltimoreCity Health Department (BCHD), Mayor’s Office ofEmployment Development (MOED), Mayor’s Officeof Performance & Innovation (OPI), Baltimore Corps,HealthCare Access Maryland (HCAM), and Jhpiegohave worked intensely since May 2020 to bring thisprogram to fruition, deliver vital services to BaltimoreCity residents, and address the spreading COVID-19pandemic. Despite the pressures of piloting the HealthCorps and working tirelessly during a pandemic, theleaders and staff were exceedingly generous, providing us with their time, expertise, and backgroundknowledge in helping us complete this Early Lessonsreport.Specifically, we thank our partners for their efforts inhelping us to understand the issues surrounding theprogram’s implementation, and sharing challengesand best practices to inform this report. They include:We also thank our funders for prioritizing dissemination of findings and rigorous evaluation inimplementing the Baltimore Health Corps, and forfacilitating the publication of this report. The fundersinclude:The Rockefeller Foundation – Emilia Carrera,Leah Perkinson, and Shawna HoffmanBaltimore Civic Fund, the program’s fiscal sponsor –HyeSook Chung, Cassandra Sullivan,and Emily DuncanFinally, we thank the Baltimore Health Corps team ofCommunity Health Workers serving as contact tracersand care coordinators, along with supervisors, managers, career navigators, administrators, and staff fortheir work to support the City of Baltimore during thischallenging time. Your efforts to address health equityand help your fellow residents are historic and vitallyimportant.BCHD – Darcy Phelan-Emrick, Jennifer Martin,Anna Schauer, Adena Greenbaum, Sarah Rives,Heang Tan, Elise Bowman, and LaNisha ChildsMOED – Rachel Brash, John Ford, MacKenzie Garvin,Patricia Morfe, and Jason Perkins-CohenOPI – Brendan Hellweg, Dan Hymowitz,and Justin ElszaszBaltimore Corps – Fagan Harris, Sarah Flammang,and Daniel PalmerHCAM – Traci Kodeck and Lynell MedleyJhpiego – Kristina Grabbe, Maya Tholandi,Alisha Smith-Arthur, Jennifer Snyder,and Jennifer Breads.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE3
PrefaceIn the spring of 2020, as the COVID-19 pandemic surged inthe United States, the city of Baltimore, Maryland, confrontedconverging crises in public health and unemployment thatexacerbated persistent inequities there and around the country.In partnership with The Rockefeller Foundation, the city designedand piloted the Baltimore Health Corps (BHC). Among the firstof its kind in the nation, the program sought to recruit, train,and employ 275 new public health workers – Baltimoreans whowere unemployed, furloughed, or underemployed, and livingin neighborhoods hardest-hit by the twin economic andhealth crises.The Rockefeller Foundation, the City of Baltimore, andour partners worked together to ensure that the BHCpilot would be ready-made for adoption and adaptation elsewhere by healthcare and municipal leaders,policymakers, and the organizations and individualswho fund them. We embedded a strong, independent evaluation as part of this work to ensure theprogram could use performance data to continuallylearn and improve, and to ensure that we could buildan evidence base for what works and what doesn’tin building an innovative jobs and community-healthprogram.By the time the program launched, COVID-19 washitting Baltimore hard. Infections and deaths soareddisproportionately among Black and Latino populations while, at the same time, the city experiencedpeak unemployment, reaching 11.6 percent in April2020, compared with 5.5 percent a year earlier. Inthis report, we examine early lessons from work performed by the hundreds of Baltimoreans serving inBHC during this challenging period.In evaluating our progress, we considered three corequestions: Did we hire BHC members in a mannerthat prioritized equity and the make-up of the widerBaltimore community – specifically the communitieshardest hit by COVID-19? Did we improve contact tracing efforts from their prior levels of success? And didwe successfully provide care coordination servicesthat met the community’s needs?By sharing the timely lessons in this report, we hopethe BHC will prove a useful model for cities and othercommunities seeking to draw from this work. Later in2021, our independent evaluator will conduct furtherassessments of its efficacy, effectiveness, and equity.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE4
Finally, we want to acknowledge the many peopleand organizations that made this report possible. Ourevaluation partners Dylan H. Roby, Neil J. Sehgal, EllePope, Melvin Seale, and Evan Starr from the Universityof Maryland’s Department of Health Policy andManagement, Robert H. Smith School of Business,and Health Systems and Policy Research Lab.Our evaluation steering committee includedBrendan Hellweg, Darcy Phelan-Emrick, RachelBrash, Kristina Grabbe, Traci Kodeck, Lynell Medley,Sarah Flammang, Emilia Carrera, Leah Perkinson, andShawna Hoffman. Our partners in the city – includingthe Baltimore City Health Department, the Mayor’sOffice of Employment Development, the Mayor’sOffice of Performance & Innovation, Baltimore CivicFund, Baltimore Corps, Jhpiego, Healthcare AccessMaryland, Maryland Access Point, Baltimore Alliancefor Careers in Healthcare, Catholic Charities ofBaltimore, Maryland Volunteer Lawyers Service, andCities for Financial Empowerment – were essentialto our success. Lastly and crucially, we want to thankthe community health workers, managers, and administrators, working tirelessly, especially with the mostvulnerable in their communities, to flatten the curve ofthe pandemic.Brandon M. ScottMayor of BaltimoreOtis Rolley IIISenior Vice President, Equity and Economic OpportunityThe Rockefeller FoundationTACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE5
Acronyms and AbbreviationsTERMDEFINITIONBACHBaltimore Alliance for Careers in HealthcareBCHDBaltimore City Health DepartmentBHCBaltimore Health CorpsCCCatholic Charities of BaltimoreCHWCommunity health workerCICase investigatorCMSCenters for Medicare and Medicaid ServicesCRISPChesapeake Regional Information System for Our PatientsCTContact tracerHCAMHealthCare Access MarylandLHICLocal Health Improvement CoalitionMAPMaryland Access PointMDHMaryland Department of HealthMOEDBaltimore City Mayor’s Office of Employment DevelopmentMVLSMaryland Volunteer Lawyers ServiceNORCNational Opinion Research CenterOPIBaltimore City Mayor’s Office of Performance & InnovationREDCapResearch electronic data captureWIOAWorkforce Innovation and Opportunity ActTACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE6
Tackling the Dual Economic and Public Health CrisesCaused by COVID-19 in BaltimoreEarly Lessons from the Baltimore Health Corps PilotAuthorsSupported by a consortium of fundersDylan H. Roby, Ph.D.Neil J. Sehgal, Ph.D., M.P.H.Elle Pope, M.P.H.Melvin Seale, M.A., D.HScEvan Starr, Ph.D.Abell FoundationThe Annie E. Casey FoundationBaltimore City allocation of United States' CoronavirusAid, Relief, and Economic Security Act fundsBaltimore Community FoundationBaltimore Gas and ElectricBaltimore RavensBank of AmericaBloomberg PhilanthropiesCareFirst BlueCross BlueShieldFrance-Merrick FoundationGoldseker FoundationHarry and Jeanette Weinberg FoundationHoffberger FoundationJacob & Hilda Blaustein FoundationJohns Hopkins Bloomberg School of Public HealthKaiser PermanenteLeonard & Helen R. Stulman Charitable FoundationMaryland Department of LaborOpen Society FoundationsPepsiCo FoundationRauch FoundationT. Rowe Price FoundationThe Rockefeller FoundationDepartment of Health Policy and ManagementHealth Systems and Policy Research LabUniversity of Maryland School of Public Healthhealthpolicy.umd.eduDesign: Ahoy.Image: Jhpiego/Juliana AllenCopyright Copyright by the University of MarylandCollege Park 2021Commissioned by the City of Baltimoreand a consortium of funding andimplementing partners listed -corps-pilotThis report is based on research funded bya consortium of funders listed above. The findings,views, and conclusions contained within are thosesolely of the authors.https://healthpolicy.umd.edu/TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE7
Executive summaryOn March 12, 2020, the first case of coronavirus disease 2019(COVID-19) was diagnosed in Baltimore City. Its infection rateincreased rapidly through March and into April and May, provingto be 4 times higher among Latino residents and 1.5 timeshigher among Black residents than the city’s White population.At the same time, the city’s unemployment rate surged from4.9 percent in March to a peak of 11.6 percent in April 2020.†In June, Baltimore City government launched the Baltimore Health Corps (BHC), a pilot program to recruit, train,and employ 275 new community health workers who were unemployed, furloughed, or underemployed, livingin neighborhoods hardest hit by the health crisis and especially those residents unemployed as a result ofCOVID-19. BHC used equitable recruitment and hiring practices to employ contact tracers, care coordinators,and support staff, with a focus on good jobs, fair pay, training, skill-building, and support to improve careertrajectories. The city leveraged its existing partnerships to move quickly.IMPLEMENTING PARTNERROLEBaltimore City Health Department Hiring, contact tracing, call center, outbreak investigation, older adult care(BCHD)coordination, and program administrationBaltimore Civic FundProgram administration and fiscal sponsorshipBaltimore CorpsRecruitment, screening, and referralHealthCare Access Maryland(HCAM)Care coordination, vaccination and testing support, program administration,and addressing social determinants of healthJhpiegoHiring and onboarding, contact tracer training, program planning, and technicalsupport for contact tracingMayor’s Office of EmploymentDevelopment (MOED)Recruitment, career navigation, financial counseling, post-BHC job placement,and management of supports from Catholic Charities of Baltimore, MarylandVolunteer Lawyers Service, and Baltimore Alliance for Careers in HealthcareMayor’s Office of Performance& Innovation (OPI)Program coordination, management, analysis, and design support† U.S. Bureau of Labor Statistics. Unemployment Rate in Baltimore City,MD. FRED, Federal Reserve Bank of St. Louis; FRED, Federal ReserveBank of St. Louis. ING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE8
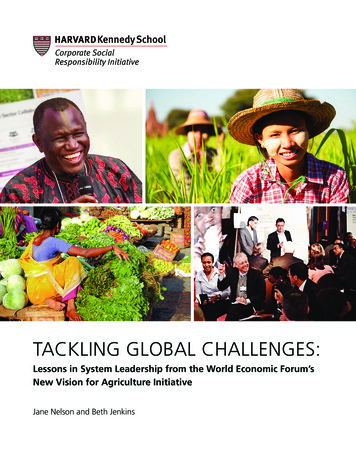
Objectives andearly findingsThree core objectives guide the work of the BHC pilot,and an early-findings evaluation of its first six monthshas indicated progress on all three. The evaluationalso identified where to focus ongoing efforts toimprove each objective.1CREATE JOBS WITHEQUITABLE HIRING AND CAREERDEVELOPMENT POSSIBILITIES2INCREASE CAPACITY FORCOVID-19 CONTACT TRACINGOBJECTIVE 1Create jobs with racially equitable hiringand career development possibilitiesLaunch hundreds of community health worker (CHW)jobs in contact tracing, care coordination, andprogram operation, while building sustainable employment and economic stability paths for those hiredboth during and after the pandemic.Early findingsBHC reached its hiring target of 275 as of January 31,2021, providing new roles as contact tracers and carecoordinators to residents. Of these new employees,more than 85 percent were previously unemployed,furloughed, or underemployed, about 70 percentlived in Baltimore City, and at least 65 percent wereBlack, Indigenous, and People of Color (BIPOC). BHCmet equity targets in hiring staff that roughly reflectedBaltimore’s racial and geographic diversity. The programoffered training to selected applicants who were notinitially hired to increase their possibility of being hiredin another cycle or by another employer. The new staff,primarily hired through the city’s health department,expanded the size of the department by over 15 percentin six months – much faster than the usual pace of hiringand growth for a special project. BHC also hired fivecareer navigators and one navigation supervisor to support the new staff and provided behavioral health andlegal services through contractors.DEMOGRAPHICS OF BALTIMORE CITY RESIDENTS63% BLACK30% WHITE6% LATINO3% ASIAN2% OTHERHIRES AND ACTIVE OFFERS AS OF JAN 31, 20213PROVIDE ESSENTIAL CARECOORDINATION52% BLACK21% WHITETACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE7% LATINO7% OTHER3% ASIAN9
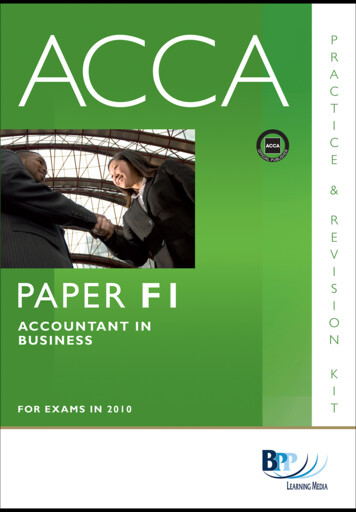
OBJECTIVE 2Increase capacity for COVID-19 contact tracingDevelop and implement an effective COVID-19 caseinvestigation and contact tracing program usingtrained CHWs to meet the upsurge in demand.Early findingsThe first BHC contract tracers were onboarded onAugust 6, with additional capacity added through thefall of 2020. By November, BHC had hired more than80 people to conduct contact tracing and was alreadyoperating at 60 percent of capacity, but the surge wasstill challenging to manage, especially when the cityfaced a 350 percent case increase from October toNovember. Test turnaround time – the time from testspecimen collection to test result – also increasedduring that period, which made timely contact tracingeven more challenging. However, by January 31, 2021,the contact tracing team was fully staffed and BHC wasable to operate at full capacity to address surges. Therate of positive cases who completed interviews rosefrom 67 percent at BHC’s August inception to 73 percentin January. The number of contacts who were contactedwithin 24 hours increased from 67 percent to 80 percent, while those who completed interviews rose from50 percent to 78 percent over the same time period.Contact tracers operated on a “call center” model untilmid-December, then moved to a “case management”model designed to allow for more relationship buildingand continuity. An early lesson was the importance ofincluding Spanish-speaking corps members who couldserve Baltimore’s Latino NTACTEDWITHIN 24 HOURSOBJECTIVE 3Provide essential care coordinationAddress the needs of the most vulnerable populationsthrough enhanced care coordination, including helpin quarantining and providing financial aid and support for caregivers.Early findingsInitially, fewer residents were actively requesting carecoordination services than originally anticipated.Thus, BHC worked to improve referral coordinationwith the contact tracing team, while also redeploying resources to testing sites, flu clinics, andhousing complexes. After these changes occurred inNovember, care coordination experienced a 126 percent increase in referral volume. The majority of carecoordination clients (77 percent) came through directcalls to health care phone lines. The most commonrequests of these referrals were: access to food (33percent), commodities/supplies (14 percent), quarantine support (13 percent), help with utilities(11 percent), and housing (8 percent).ACCESSTO P 20JAN2021TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE10
Conclusions and RecommendationsFlexibility, dedicated staff, buy-in from leadership, strong existingpartnerships, and a determination to use data to drive decisionshelped BHC adapt to the changing needs of city residents. Itgrew and developed through an iterative approach to incorporatelessons in real-time. However, gaps and challenges need tobe addressed by Baltimore and by any other localities seeking toset up similar programs. The following recommendations shouldbe considered during program budgeting, design, andimplementation. The “specific recommendations” relate toBHC’s concerns as it refines its program, while the “broaderrecommendations” are for a wide audience of organizations thatmay consider designing and deploying a similar program.Specific recommendations for BHCBased on Baltimore City’s experience with theBHC pilot, several opportunities were identified toimprove and leverage new resources to support thecontinuation and adaptation of the pilot.Invest in the CHW workforce by taking advantage offunding available through H.R. 1319, the AmericanRescue Plan (ARP) Act of 2021. Transition the BHC workforce into roles to support the COVID-19 vaccine roll-outor other community health work in Baltimore as supported by federal funds in Section 2501 of the ARP Act.Develop a centralized information technology infrastructure to collect and share data across partners,both to facilitate performance improvement and toserve as a proof of concept for future interdisciplinary projects. Funding to support these activities isexpected to be available through Section 2401(b)(5) ofthe ARP Act.Consider revisiting the original goals of the programby assessing newly available data and gaps uncoveredor exacerbated during the pandemic.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE11
Broad recommendations for developingand implementing a similar programBaltimore City’s experience in developing andimplementing the BHC offers an exemplar for statesand localities. The following guidance draws onBHC’s successes and lessons learned.OPEN COLLABORATION AND COMMUNICATIONUse existing contractors and relationships where possible, which will facilitate the work. Familiarity, opencommunication, and the ability to quickly executecontracts and start funds flowing will be vital.Use a multidisciplinary team-based approach forplanning and execution that dissolves traditional silosbetween economic development and public healthto ensure buy-in across agencies and leverage variedexpertise.Allocate resources for a dedicated project managerwith experience working across the city, county, orstate with the partners involved.Delineate leadership and decision-making authorityfor workgroups and the overall program.Develop strong linkages and coordinate with departments or programs not involved in the contact tracingand care coordination activities. Communicating withlocal leaders and industry partners focused on testing, patient care, and other aspects of disease controlwill be vital to success.PREPARE THE WORKFORCEEnsure existing staff and leaders have necessarytraining and learn the values needed to engage inequitable review and hiring practices.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE12
Supplement initial training with a supportive mentorship initiative and on-the-job training that allow forcontinuous skill-building.Remove barriers where possible for applicants andnew hires related to criminal history backgroundchecks and drug-testing requirements to encourageworkforce equity and facilitate faster hiring.Leverage existing training models and adapt thecurriculum to meet specific program needs. Also,repurpose training when needed to support eventualvaccine outreach, uptake, and administration.Involve community-based organizations that canprovide additional resources such as computer literacy and interview preparation. These organizationscan both help remove technology barriers during thepre-interview process and identify potential applicants.IMPLEMENT AND MAINTAIN FLEXIBILITYBe flexible during the program’s design and implementation, so leaders and staff feel empowered topivot quickly in addressing challenges.Facilitate hiring of data analysts to manage multipledata sources, do near-time performance tracking, andfacilitate data access for partners to help improve theprogram while it is ongoing.Offer support to encourage post-program placementopportunities, such as career navigation, behavioralhealth, legal services, job placement assistance, andfinancial empowerment training.Work with employers in the region to create a pipelinefor referrals into longer-term positions for employees.ADDRESS VULNERABLE GROUPSAttempt to analyze data on the race/ethnicity of theunemployed population to ensure targets are representative of those most likely to suffer from loss ofwork or chronic unemployment.Conduct focus groups or interviews with communitymembers to better understand their needs and theimpact of programs on their employment and healthoutcomes.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE13
BackgroundBaltimore City and its partners launched the BaltimoreHealth Corps (BHC) on June 4, 2020, to equitablyaddress the dual economic and public health crisescreated by the coronavirus disease 2019 (COVID-19)pandemic. By January 31, 2021, BHC employed 240residents of the city and surrounding counties who hadbeen unable to find jobs due to the pandemic, introducingthem to new roles as contact tracers, outbreak investigators,care coordinators, managers, and support staff. TheBaltimore City Health Department (BCHD) and the Mayor’sOffice of Employment Development (MOED) jointly ledthe pilot by leveraging existing partnerships, capacity,and expertise in equitable recruitment and hiringpractices, workforce support activities, public healthcapacity-building and training, and care coordination.UNEMPLOYMENTRATE SURGEDFROM A LOW OF4.9% IN MARCHTO A PEAK OF11.6% BYAPRIL 2020On March 12, 2020, the first COVID-19 case wasdiagnosed in Baltimore City, resulting in closures, aslowing of economic activity, and implementation ofpublic health measures. As the case rate and positivityrate increased through March and into April and May,the unemployment rate surged from a low of 4.9 percent in March to a peak of 11.6 percent by April 2020.aA second case surge in December 2020 and January2021 threatened to destabilize the economy andoverwhelm local hospitals.a. U.S. Bureau of Labor Statistics. Unemployment Rate in Baltimore City,MD. FRED, Federal Reserve Bank of St. Louis; FRED, Federal ReserveBank of St. Louis. ING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE14
BHC’s theory of changeBaltimore developed a new workforce of trainedcommunity health workers (CHWs) by deployingBHC, a unique transitional jobs program launched inresponse to the COVID-19 pandemic, which:Used innovative methods torecruit and hire an equitableworkforce with the potential tosucceed as contact tracers andcare coordinators based upontheir previous experiences,community involvement, empathy, and interest in helping theircommunityAddressed critical COVID-19needs in vulnerable communities and provided employmentto persons who werejobless as a direct or indirectresult of COVID-19Increased short-term employment opportunities inpublic health for residents andattempted to improve theirlong-term career paths andeconomic mobilityEnabled BCHD to do neededcontact tracing and case investigation workEnabled HealthCare AccessMaryland (HCAM) and MarylandAccess Point (MAP) to delivercare coordination for vulnerable members of the community.In order to improve the ability of these BHC employees to pursue longer-term sustainable careerpathways and economic mobility, the BHC pairedefforts to prepare and train the new workforce hireswith support services, such as behavioral health,legal services, career navigation, and financialempowerment. By drawing contact tracers and carecoordinators from local communities and neighborhoods affected by the dual economic and publichealth threats, the BHC attempted to improve bothhealth and economic outcomes for city residents.Cities, counties, states, and the federal governmentwill benefit from early lessons and recommendationsfrom the BHC in responding to increases in unemployment, COVID-19 cases, and COVID-19-related deaths.BHC’s focus on hiring and training community healthworkers to serve vital roles in local COVID-19 responsesaligns with the recently passed American Rescue PlanAct of 2021, which allocates funding for approximately100,000 public health workers to address COVID-19vaccine outreach and contact tracing, and later to transition into long-term roles supporting the needs of theircommunities.1This report describes the formation and implementation of the BHC pilot program and explains itsobjectives and key components. Further, it gleansinformation from observations, program documents,existing data used for reporting and tracking purposes,and interviews analyzed by the University of Maryland(UMD) School of Public Health and Robert H. SmithSchool of Business. These combine to provide earlyfindings, describe challenges, and document lessonslearned, and in turn, make recommendations basedon its first six months (see Appendix F for details of themethodology). UMD, as the independent evaluator forthe BHC, has assessed the pilot program’s abilityto achieve its main objectives and answer specificlearning questions (see Appendix G for full list oflearning questions). It also has developed early lessonsand recommendations from the pilot.TACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE15
FIGURE 1Summary of BHC logic modelPROBLEMSOLUTIONACTIVITIESEXPECTED OUTCOMESCOVID-19 increasesCreate equitableemploymentopportunitiesWorkforce supports,including carer navigation,legal supports, behavioralhealth, financialempowerment counselingShort-term employmentOngoing training andperformance supportto improve programoutcomes and qualityImproved health outcomes UnemploymentNeed for publichealth programsto contain diseasespread RecruitmentScreeningHiringTrainingConduct contact tracingand case investigationProvide care coordinationservicesLong-term sustainablecareer pathways andeconomic mobilitySocial needs addressedContainment of COVID-19Economic impacts andunemploymentCOVID-19 incidence,testing, and test turnaround timeCOVID-19 vaccineavailability & distributionLocal and state policychanges or mandatesEXTERNAL FACTORS THAT CAN IMPACT BROADER OUTCOMES OR REQUIRE PROGRAM ADAPTATIONTACKLING THE DUAL ECONOMIC AND PUBLIC HEALTH CRISES CAUSED BY COVID-19 IN BALTIMORE16
Evidence Base Supporting the BHCPilot ModelBHC used an equity-based transitional jobs programmodel to identify motivated candidates who showedempathy, enthusiasm, and an interest in helping theircommunities through contact tracing and care coordination. Transitional jobs programs result in positiveshort-term employment and long-term employmentoutcomes.2 As there is no evidence around their usein pandemic response and mitigation, BHC relied onevidence from previous efforts to develop and adapt itsown unique approach.Rather than providing subsidies to employers to hire eligible workers, BHC offered an intentional hiring model.Its model prioritized an inclusive, unbiased recruitmentand application process, coupled with systematiccandidate screening. BHC aimed
and employ 275 new community health workers who were unemployed, furloughed, or underemployed, living in neighborhoods hardest hit by the health crisis and especially those residents unemployed as a result of COVID-19. BHC used equitable recruitment and hiring practices to employ contact tracers, care coordinators,