Transcription
Internal Medicine ReviewDiagnostic Process for CIRSMay 2018Diagnostic Process for Chronic Inflammatory ResponseSyndrome (CIRS): A Consensus StatementReport of the Consensus Committee of Surviving MoldAuthorsRitchie Shoemaker MD¹Karen Johnson MD¹Lysander Jim MD¹Yvonne Berry MD¹Ming Dooley¹James Ryan PhD²Scott McMahon ,DeerfieldBeach, FloridaCorrespondenceRitchie Shoemakerritchieshoemaker@msn.comAbstract:Clinical management of patients with a complex,multisystem, multi-symptom illness identified as a chronicinflammatory response syndrome (CIRS) has expanded. Oftenassociated with illness due to exposure to low molecularweight biotoxins and inflammagens found (i) inside waterdamaged buildings (WDB); (ii) following exposure to bloomsof cyanobacteria; (iii) following consumption of ciguatoxicfish; and (iv) following confirmed acute Lyme disease,persistent despite reasonable use of antibiotics, CIRS isincreasingly recognized. A need for a formal case definitionand case management protocol has arisen. Patients with CIRSwill have abnormalities in innate responses, reduced levels ofregulatory neuropeptides MSH and VIP, elevatedinflammatory markers of C4a, MMP9 and TGF beta-1.Systemic illness, based on abnormal gene activation andsuppression, as shown by RNA Seq and transcriptomics,requires a multi-factorial, rigorous diagnostic assessment toassist in both differential diagnosis and monitoring responseto therapy. A consensus statement is herein provided to assistpractitioners in case identification and management.Key words: CIRS, water-damaged buildings, transcriptomics,cyanobacteria, Post Lyme syndrome ciguatera, visual contrastsensitivity1Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSIntroduction :As the third decade of CIRS-medicinebegins, the key elements of CIRS arereviewed in a consensus statement toenhance accuracy and reliability of thediagnosticprocess.Thisconsensusstatement has been approved by (i) thediagnostic module consensus statementcommittee of Surviving Mold and (ii)approved by the 65 members of theSurviving Mold list serve.Section 1. What is CIRS?Chronic inflammatory response syndromes(CIRS) are multisystem, multi-symptomillnesses acquired following exposure toenvironmentally produced biotoxins (1, 2, 3,4, 5, 6, 7, 8, 9).CIRS has gone through an evolution ofnames over the years. Initially, in the1990’s, CIRS was called a neurotoxinmediated illness (10, 11). As moreinformation was added, the term waschanged to chronic biotoxin associatedillness (CBAI). The third change to CIRSoccurred following development of acommercial assay for transforming growthfactor beta-1 (TGF-beta-1) in 2008, shortlybefore the development of a commercialassay for acquired T regulatory cells in2009. CIRS was confirmed to involve manyarms of the immune response systems actingsimultaneously and in combination.CIRS itself is modeled after an acutesystemic inflammatory response syndrome(SIRS), an acronym typically used todescribe an acute inflammatory illness, mostcommonly sepsis. In patients with sepsisthere is simultaneous activation of Th1, Th2and Th17 immunity; coagulation factors;and complement in response to anoverwhelming stimulus of infection andendotoxin present in the blood stream. Inthis regard, the illness becomes the hostMay 2018response as eloquently described by Thomas(12).Survivors of sepsis have been well studied;they have a heightened level of innateimmune activation post-sepsis compared tobefore. Survivors have a significant increasein interleukin 10 and go on to suffer agreater incidence of chronic fatiguingillnesses (13, 14).In 2008, followed by a publication in 2010(19), members of the ―mold‖ medicalcommunity began using a jargon term,CIRS-WDB to describe illness seen with thesame activation of Th1, Th2, Th17,coagulation, complement activation andmore. If the illness came from waterdamaged buildings, it was called CIRSWDB. If symptoms came from Post LymeSyndrome, it was called CIRS-PLS. Ifsymptoms came from ciguatera it was calledCIRS-ciguatera. Theoretically, one couldcall the syndrome most anything; possiblythe syndrome would be codified by aregulatory agency, much as the CDCchanged the name, ―Pfiesteria health illnesssyndrome (affecting) humans,‖ PHISH, foracute and chronic illness caused by exposureto blooms of toxigenic, fish-killingdinoflagellates, including Pfiesteria, to―Possible estuarine-associated syndrome‖(PEAS, 11).Section 2. Case definition of CIRSIn 2008, the US General AccountabilityOffice (GAO) published an overview ofpublications from US agencies working onthe problem of damp indoor buildings (20).54 studies were noted, showing nocoordination of efforts across agency lines.But for the first time, a Federal casedefinition for what has become CIRS-WDBwas proposed.1. There must be the potential forexposure to a damp indoor space.2Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRS2. There must be a multisystem,multi-symptom illness presentwith symptoms similar to thoseseeninpeer-reviewedpublications.3. There must be laboratory testingresults similar to those seen inpeer-reviewed, published studies.4. There must be documentation ofresponse to therapyThis definition still is used even thoughthere has been an explosion of publicationsin the CIRS community noting variousobjective parameters in wide clinical usenow (1).Symptoms are noted to be al exposures resulting in CIRS(see Table 1). Of interest is the appearanceof clusters of symptoms among the 37symptoms recorded in CIRS (Table 2).Presence of eight or more of the 13 clustersis virtually diagnostic of an unspecified typeof CIRS (US Patent 9,770,170 B2; issued9/26/2017).Section 3. Before the first office visitSeeing a health care provider as a newpatient brings a series of expectations ofstandard medical practice process. Formswill be filled out, insurance data recorded,HIPAA information processed; officepolicies, billing information sheets andmaybe even an overview of the philosophyof the practice will be reviewed. Organsystem-related specialists (heart, lung, GI,neurologist and more) will focus on theirareas of expertise; maybe the appointmentwith a primary care provider might center ontreating the patient as a whole person, not aheart, or a lung, or a colon in isolation.CIRS providers are going to approach firstoffice visits differently. Based on theexperience of thousands of initial officevisits with CIRS providers it is likely thatMay 2018patients will have failed to findimprovement from least 10 physiciansbefore, at least one of whom was apsychiatrist. None made any delineation ofthe abnormalities in physiology, but insteadeach has often made a diagnosisunsupported by objective biomarkers.Review of past medical records remains themost important initial duty of the CIRSprovider to the patient. The patient, in turn,must show due diligence to provide theprovider with every relevant document.When the work involved in providing athorough copy of records is too onerous, areasonable suggestion is to postpone theinitial visit. Regardless of motivation to getbetter, many CIRS patients do not havereliable recall of an exposure time-line,symptom time-line and medication time-line(including supplements and all anti-fungals,even topicals). Laboratory testing ofteninvolves ―cash-only labs‖ which may be notrigorous. Frequently, the basis for clinicaldecision making is inadequately supported.Assumptions and frank guesses are rife:these have no role in CIRS casemanagement.Patients often will insist that their symptomrecall and self-based diagnosis is inherentlyreliable. (As an example, how do CIRShealth care providers analyze chiefcomplaints like, ―I get a spasm in mykidneys when my brain inflammation actsup.‖) Symptoms of CIRS vary from day today and are subject to unnoticedenvironmental exposures. Unfortunately,given the 90% incidence of cognitiveimpairment in CIRS, symptoms lasting morethan a few months are usually lost in timelines as the illness continues.An additional problem for the CIRSprovider is the demand for a ―hurry-up‖appointment. There can be no hurry-upwhen records must be reviewed carefully!3Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSGive the CIRS doctor time to read everypage of the medical record. Organize therecord, get rid of duplicates, make itchronological but do not leave anything out.Organized summaries make some sense butnot at the risk of editing by the patient. Inthe example of 5000 pages of recordsusually there will be one or two pages thathave the answers persistently ill patientshave sought.One might have become frustrated withimpersonal, community-based providers, socalled mainstream physicians, who guessedat what was wrong, but really did not know,so some patients might have ―gonealternative.‖ Maybe a CIRS met some caringdoctors outside the mainstream, but maybeothers met predators who sold snake oil inmodern trappings. Once again, guesses,assumptions and lack of support from peerreviewed literature will dominate themedical record.The first step in diagnosis of CIRS is toknow what has been said about the patient.Ignore the snide innuendo of, ―It’s all inyour head.‖ A NeuroQuant will show whatiswrongcognitively.Ignorethefibromyalgia diagnosis and the gabapentinprescription. The lab results tracking CIRSand transcriptomic findings are the light inthe darkness. Once one sees objective,proven, reliable scientific findings that leadto a proven treatment protocol, a CIRSprovider will usually show the patientsomething long-lost: Hope.Hope is based on data. Hope is based onpublished work, validated by CIRSphysicians over the past 22 years. The Hopein CIRS is supported by favorable Daubertand Frye decisions in courts across the US.Patients will likely be asked to stopunneeded medications immediately. Throwthe amitriptyline bottles into the ―worthlesspsych nostrum‖ drawer.Eliminate theunneeded bags of supplements andantibiotics possibly sold to patients by thoseMay 2018who prescribed them. Patients will beadmonished to stop nasal, oral andintravenous anti-fungals, as they are creatingresistant mutant MARCoNS that are alreadythreatening desperately ill infectious .Outside learning will be included; one willprobably be instructed to read severalhundred pages of documents found (free) onwww.survivingmold.com,understandingthat few will remember everything. MostCIRS patients have difficulty assimilatingnew knowledge, but possibly loved oneswill read and learn more as well. In time,patients must become an expert in the jargonand pathophysiology of CIRS. Why?Simple: the illness is real. CIRS protocolswork to correct the physiology and theunderlying transcriptomic abnormalities.Section 4. Evolutionparadigm of CIRSofthePatients may also be asked to review thehistory of CIRS. Knowing the past is an allyfor expansion of future understanding. Thehistory of the case definition of CIRS ismarked by a series of ―spike events.‖ Aspike occurs when there is a publication or abreakthrough that adds exponentially toprior thought. Initially, CIRS was felt to besimply an inflammatory response toexposure to the environmentally producedneurotoxins. Dinoflagellate illnesses, such asPfiesteria and ciguatera were the afflictionsmost relied upon to develop the casedefinition in the late 1990’s. Later a (1997) and then to the interiorenvironment of water damaged buildings(WDB, 1998), showed that an uncannysimilarity of symptoms was shared by eachof these diverse sources of inflammatoryillness.4Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSBecause the initial sources of illness in someinstances could not be identified reliably, thecase definition in 2003 simply included: i)the potential for exposure; ii) presence of amulti-system, multi-symptom illness and;iii) absence of confounding exposures ordiagnosis.When objective lab studies could be added,first including visual contrast sensitivity(VCS), HLA DR by PCR and melanocytestimulating hormone (MSH), a commonalityof inflammatory abnormalities together withsimilarity of symptom groups within subsetsof this neurotoxin mediated illness mine (CSM) after removal fromexposure (or treatment of underlyinginfectious disease) together with clearanceof multiply antibiotic resistant coagulasenegative staph (MARCoNS), resident indeep nasopharyngeal space.In 1998, Lyme researchers Donta andCartwright patented the identification of abiotoxin made by Borrelia burgdorferi(Publication number CA2365424 A1), thecausative agent in Lyme disease. Since CSMworked well to treat other biotoxins, its usein Lyme patients followed. The unexpectedand precipitous untoward reactions ofpatients with Post Lyme Syndrome to CSMcaused a stunning rethinking of concepts ofbiotoxin illnesses. The observed group werepeople with confirmed Lyme disease asshown either by (i) a physician witnessederythema migrans rash in association with arecent tick bite or (ii) clear evidence of asignificant antibody response as shown byWestern Blot testing done in reliablelaboratories. These patients, when givencholestyramine after a reasonable course ofantibiotics,didnotimproveasdinoflagellate, cyanobacteria and WDBpatients did. They got worse.This never-before-seen adverse reaction,labeled ―intensification,‖ was quickly shownMay 2018to be due to a massive pro-inflammatorycytokine response as manifested MMP-9).Thissyndrome was recognized initially asshowing a fall in VCS scores beginning inrow E, followed by a fall in row D. This wasnot a ―Herxheimer‖ reaction; it had nothingto do with antibiotics. It simply was a proinflammatory cytokine event.While Post Lyme Syndrome patientspresented treatment difficulties, thesechallenges were the source of new therapiesfor pro-inflammatory cytokine responsesadded to the simple cholestyramine andMARCoNS protocol.As the intensification reaction becameamenable to diagnosis, treatment andprevention, there were a series of patientswho improved beyond what we had seenwhile others still were ill.In rapid fire order in the early 2000’sphysicians were able to see the (i) low levelsof vascular endothelial growth factor(VEGF) and (ii) elevated levels of splitproductsofcomplementactivation,especially C4a, which would becomeadditional targets for sequential treatment.Melanocyte stimulating hormone (MSH)was the first regulatory neuropeptide to beidentified as deficient in the early CIRScases. Because MSH exerts a regulatory roleon production of other hormones, especiallyincluding gonadotropins, it was not asurprise to find that androgens together withestrogens were affected by MSH deficiency.To this day, physicians are attempting to―balance‖ androgens and estrogens; thisapproach remains surprising in that aproximal step, that being correction of MSHdeficiency, is mandatory in correctingandrogens and estrogens.Researchers also saw that MSH interactedwith antidiuretic hormone (ADH) in thehypothalamus to regulate other hormoneactivities in addition to salt and water5Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSbalance. MSH controls tight junctions in thegut, a fact often overlooked by those whodiagnose ―leaky gut.‖The discovery that vasoactive intestinalpolypeptide (VIP), another regulatoryneuropeptide, was deficient in 90% ofpatients with the syndrome set off anotheravenue of inquiry in the physiology of theillness. Providers now know thatmeasurements of VIP receptors 1 and 2 arealso important to fully understand VIP’sefficacy. Transcriptomics shows us how VIPreceptors are intimately tied to the activitiesof a family of nuclear transcription factors,Ikaros.As objective lab parameters began to beassociated loosely with some specificgrouping of symptoms, it was the sequentialtreatment method that enabled providers toapproach symptom reduction in adisciplined manner. By correcting oneobjective parameter at a time, patients couldidentify symptoms that were improved,implying that there were objectiveparameters correlating with specific lababnormalities.Symptoms reported by patients, bydefinition, are subjective. However, whensymptoms are collected as part of a medicalhistory, the subjective aspect is nowfunneled through the trained mind of anexperienced health care provider to yield anobjective picture of symptoms. Symptomrecording has shown a lack of reliabilitywhen performed by the patients using acheck list or (even less reliable) using theirmemory alone.Symptoms, however, remain vitallyimportant in understanding the multisystem, multi-symptom elements that arecrucial to the differential diagnostic processof this illness. Even though symptoms aresubjective, accurate collection of a medicalhistory remains the single most importantaspect of the differential diagnostic processof any illness.May 2018As the number of CIRS patients seen andtreated has expanded; and the number ofphysicians and healthcare providers who arecompetent to treat this complicated illnesshas grown, there was little variation insymptoms recorded from patients livingaround the globe. There were also specificand reproducible elements in lababnormalities that suggested that each ofthese illnesses must have an underlyingbasis reflecting differential gene activationor suppression.The concept of the ―final commonpathway,‖ began to emerge following the2010 Physician Consensus Statement (15) inwhich this inflammatory illness finally wasnamed chronic inflammatory responsesyndrome (CIRS). In other words, a CIRScaused by chronic exposure to WDB, wasnearly indistinguishable from a CIRS causedby Post Lyme Syndrome, ciguatera,Pfiesteria or cyanobacteria. The initialinciting triggers might differ in each case,but the end clinical presentation was similar.Since providers could not rely on VCSdeficits, lab abnormalities or symptomsalone to adequately distinguish one illnessfrom another, all physicians had to support adiagnosis was potential for exposure. Eventhis reliable method of history takingbecame confounded when say, someonewho had a dinoflagellate illness then movedinto a moldy apartment creating two sourcesof biotoxin exposure. Even worse, someindividuals would be residing next to freshwater areas, lakes or ponds for example, inwhich there would be cyanobacteria bloomsin addition to moldy buildings and sick fish.Clearly, physicians needed a diagnosticmethod that would (i) specify individualillness and provide the (ii) basis formonitoring results of treatment.With papers published in 2015, 2016, 2017and 2018, the importance of transcriptomicsin the diagnostic process of CIRS ismanifest.6Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSAs transcriptomics is added to CIRS casemanagement, based on case-controlledstudies and based on prospectiveintervention trials, there is a molecular basisfor the final common pathway suggested bycommonality of symptoms in sources ofCIRS. While there is an old expression that―All roads lead to a final common path thatleads to Rome,‖ what providers are seeing inthe approach to CIRS is more like that of aspider web. The greatest movement of theweb is in the very center, but the tetherscould attach variously to corners around awindow or to an object that was stableproviding a mechanism for the spider web tosurvive wind and rain. Whatever came to thecenter of the web could come from anyseemingly unrelated tether.Genomics can be regarded as the center coreof the spider web. Here is the source of allthe objective laboratory abnormalities; hereis the source of all the confusingcomplexities of symptoms and theirgroupings called clusters. Here is the basisfor CIRS illness.ToquoteacurrentPrimerinTranscriptomics (16):―Transcriptomics has now crossed fromresearch to application. It not only serves asa diagnostic aid but it also providesprecision in monitoring the complexitiesfound in many immune-based illnesses, suchas chronic inflammatory responses acquiredfollowing environmental exposures. We seetranscriptomics as an ideal mechanism tofine tune therapies aimed at correction ofinflammatory abnormalities.―The initial finding by Ryan, et al (5)showed that intranasal use of VIP in CIRSpatients, part way through their treatmentprotocols, modulated expression of bothnuclear encoded mitochondrial genes andribosomal genes. We later confirmed thatpatients naïve to treatment had profoundsuppression of these same genes. TheseMay 2018genes usually recover with the first ten stepsof the Shoemaker Protocol; they oftenbecome higher than normal controls. Atantalizing possibility for the overshoot lieswith genes important in glycolysis(breakdown of glucose into two 3-phosphate dehydrogenase(GAPDH), also functions to regulateinflammatory gene suppression after initialactivation in the presence of interferongamma.―What we think is happening is an attack onthe basic cellular metabolic elements. It iswell documented that microbial toxins (i)attack protein production at the level of theribosome and (ii) energy production in themitochondria. Patients with CIRS will notrecover unless exposure to these microbesand their cellular toxins ceases. Further, it iswell documented that in the face ofinfectious diseases, especially from viruses,that cells become ―hypometabolic‖ toprevent viral ―takeover‖ of cellular function.―This idea is relevant for the abnormalimmune responses we see in CIRS.Hypometabolic immune cells activateprimordial mechanisms: innate immunity,complement, defensins. These protectiveinflammatory elements do not requireparticipation of cells. When cells begin theprotectivemechanisms of innate immunity begin towane. Cells then upregulate proteinproduction, energy production and begin touse sugar properly. Call it a ―synchronizedreboot,‖ of cellular systems. Re-exposuresimply means a recall of innate immunityand all its protective mechanisms.―The sequence of hypometabolism andrecovery are shown by changes intranscriptomics. Certainly, the CIRSprotocol could prime ribosomal and7Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
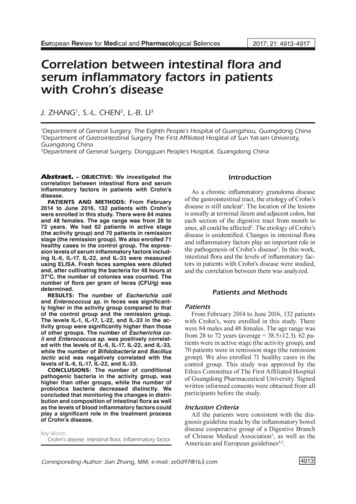
Internal Medicine ReviewDiagnostic Process for CIRSmitochondrial gene expression. Then VIPcould upregulate GAPDH gene expression.Could increased pyruvate from glycolysisfire up the mitochondrial furnace for energyproduction and then protein expression?‖ Orwill it stay suppressed as to not increaselactate production?‖With a genomics basis established for CIRS,physicians began to see application of theprinciples of CIRS to other illnesses thatinvolve inflammation but did not have allthe elements of CIRS. For example, in asmall number of patients with impendingheart transplant for dilated cardiomyopathy,gene expression of adrenoceptors and―contractility receptors‖ found in peripheralblood cells respond to CIRS protocols. If itis confirmed that cardiac myocytes alsoimprove like white blood cells do, perhapsproviders will see dramatic changes inquality of life if further myocardial injuryfrom genomic abnormalities can beprevented.Atherosclerosis is increasingly shown to bean inflammatory illness. Oxidized LDL is apotent nuclear transcription factor. Insulinand insulin resistance are the inflammatorybases of diabetes and obesity. Alzheimer’sof particular types, specifically Type III, isshown to be an inflammatory illness.Inflammation is now recognized as theunderlying mechanism, not just a source ofthe symptoms and not just the cause of lababnormalities. For further information, seethe Transcriptomic Primer (16).As the next decade of CIRS approaches, theexpansion of application of the principles ofCIRS to other illnesses, possibly ome (PANS), is becoming clear. AnMay 2018important field is the TH17/Treg imbalance.T-regulatory cell abnormalities also arerelated to abnormalities of genomics andabnormalities in some of the elements ofCIRS but not all.CIRS is now one end of the spectrum ofinflammation, with each new element as it isbeingdescribedcontributingtounderstanding of each other elementpreviously described. By adding oneinflammatory feature of an illness on top ofanother, much as blocks laid on a foundationwall, we begin to recognize that our attemptsto define diseases by organ system will fail.Physiciansrecognize,howeverthatinfectious diseases often set off systemicinflammation that will persist beyondclearance of infectious agent. In others, notso much. For the illnesses that do effectchanges in genomics, physicians andpatients alike are in the middle of arevolution of understanding and a revolutionin treatment.Section 5. Specific symptomsFrom a list of 37 different symptoms, thereare eight main categories estinal, cognitive, hypothalamic andneurologic) formed in an effort to classifysymptoms. Cluster analysis provides amechanism to take subjective symptoms,pass them through a skilled medical historyand then convert them to objective elementsusing abstruse statistical methods, includingcluster analysis. Clusters can take theseemingly endless roster of symptoms tomake their use amenable to a scoringsystem.8Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSMay 2018Table 1 - Percent incidence of symptoms in various CIRS CiguateraLymeN 239101562882142100352Fatigue61008983100709194Weak 580757084-8389Ache890776895437781Cramp 580665663146877Unusual Pains 550625142-8286Ice Pick Pain 5404941--4582Headache990786684737888Light Sensitivity 590716689686785Red Eyes 550524863684861Blurred Vision 540615663-5366Tearing 271Sinus Congestion860796574417068Abdominal Pain 560613937417942Diarrhea 550483921577251Joint Pain1170755384-6288Morning Stiffness6707244--5980Memory Impairment 580836668848180Difficulty Concentrating 570816253358382Confusion 540755726246672Decreased Word Finding 580816611-8084Decreased Assimilation 580726537-7888Disorientation 530514011-28339Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSMay 2018Mood Swings 5206965--4265Appetite Swings 5505858--6177Sweats (Night) 5506154--4268Difficulty Reg. Body Temp 5506360--6772Excessive Thirst 5606954--5971Increased Urinary Frequency 5606658--6675Increased Susceptibility toStatic Shocks 5404144--3832Numbness 540484437-7466Tingling 540615147-7871Vertigo 540394842162937Metallic Taste 540453647-4638When physicians use persistent healthsymptoms as a group of 37, recorded by atrained health care provider in a medicalhistory (never rely solely on patientcompleted checklists), individual symptomscan collate individual symptoms into groups,called clusters. Statistically, these clusters ofsymptoms, 13 in number, yield a diagnosticcapability to separate out CIRS fromessentially all diseases. If an adult patienthas 8 or more clusters of symptoms, thelikelihood of CIRS exceeds 95%.When combined with VCS deficits,symptom clusters can yield an accuracy indiagnosis of 98.5% (that means the sum offalse positives and false negatives is lessthan 2%). In the formal case definition ofCIRS, however, cluster analysis isperformed as an additional analysis to totalsymptoms reported.Cluster Analysis of SymptomsIndividual clusters (one or moresymptom in a group counts as a cluster)1. Fatigue2. Weakness, assimilation, aching,headache, light sensitivity3. Memory, word finding4. Concentration5. Joint, morning stiffness, cramps6. Unusual skin sensations, tingling7. Shortness of breath, sinus congestion8. Cough, thirst, confusion9. Appetite swings, body temperatureregulation, urinary frequency10. Red eyes, blurred vision, sweats,mood swings, icepick pains11. Abdominal pain, diarrhea, numbness12. Tearing, disorientation, metallic taste13. Static shocks, vertigoTable 2 - Cluster analysisA positive cluster analysis for biotoxinillness is presence of 8 or more of 13clusters. For pediatric patients, 6 clusters areadequate to support a CIRS diagnosis.10Copyright 2018 Internal Medicine Review. All Rights Reserved. Volume 4, Issue 5.
Internal Medicine ReviewDiagnostic Process for CIRSCIRS providers have looked at symptomsdescribed by character, including fatigue,weaknessandexecutivecognitivedysfunction. The results are underwhelming,except for pain.In a medical history, the physician is notusing a check list. Symptoms questioning isperhaps better understood after observinghow a skilled attorney will question awitness. Essentially, he will likely be askingfor the same information from multipledifferent angles trying to have a clear idea ofwhat the witness says. Similarly, a physicianwill follow the line of thought of a patient indiscussing symptoms but will circle back topin down any possible vagaries that mightbe present. In this manner, a physician willlearn to a reasonable degree of medicalcertainty, more likely than not, on a day today basis, does a patient have muscleaching? Does a patient have muscle cramps?Are there unusual pains, sharp stabbingpains that seemingly come unexpectedly andlancinate in one area of the body only todisappea
the darkness. Once one sees objective, proven, reliable scientific findings that lead to a proven treatment protocol, a CIRS provider will usually show the patient something long-lost: Hope. Hope is based on data. Hope is based on published work, validated by CIRS physicians over the past 22 years. The Hope