Transcription
2022 Provider Resource ManualCLAIMS INFORMATION2022 Provider Resource Materials
2022 Provider Resource ManualClaims Information IndexClaims submission – general . 3MNSure product . 4Peak Plan and Federally Facilitated Marketplace (FFM) Atlas Plan in Wisconsin . 4Questions and answers . 5How to submit a claim to HealthPartners . 7Electronic capabilities . . 7CMS 1500/5010 837 professional claims submission . 8UB04 /5010 837 institutional claims submission . 8Hospice claims submission . 8Submitting a refund to HealthPartners . 9Timely filing of claims . 9COB – Coordination of benefits . 10Present on admission indicators . . 10Remittance advice and template, HIPPA Version 5010 . 10HealthPartners paper remit field descriptions HIPAA version 5010 . 12Commonly used forms . 26Adjustment Request Form . . 26Appeal Request Form . 26Provider recommendation for further services . 27Provider Recommendation Form . 28Service Category List . 29Prompt payment of clean claims . 31Medical cost management . 33ClaimsXten review . 33HealthPartners ClaimsXten review edit categories . 34Clear Claim Connection – C3 . 36Multiple Procedure Payment Reduction (MPPR) Rule – Facility Claims . 37Multiple Procedure Payment Reduction (MPPR) Rule – Professional Claims. 38Casting supplies . . 43Codes for data collection and reporting only procedures . 43Global obstetric package . . .44Services not billable on a professional format . .45Services not separately reimbursable . .461/20221
2022 Provider Resource ManualSurgery . 47Global surgical follow-up care . 47Surgical supplies . 47Additional claims policies . 49Interpreter services for HealthPartners care members . 49MinnesotaCare tax . 49Reporting suspicions of fraud and abuse . 501/20222
2022 Provider Resource ManualClaims submission – generalHealthPartners contracted providers have language in their contracts stating as a condition of paymentthat all claims for services must be submitted within a specified period of the date of service. Claimsrequiring coordination of benefits shall be submitted within sixty (60) days of determining HPI’s or itsAffiliates’ obligation to make payment.HealthPartners follows guidelines outlined in the Minnesota Companion Guides and in the NUCC 1500and NUBC UB04 manual for submission of claims. The Minnesota Companion Guides can be accessedat health.state.mn.us/facilities/auc. The National Uniform Claim Committee website can be accessedat nucc.org. The National Uniform Billing Committee website can be accessed at nubc.org.For information on electronic capabilities visit: healthpartners.com/ElectronicConnectivity.1/20223
2022 Provider Resource ManualMNSure productPeak Plan and Federally Facilitated Marketplace (FFM) Atlas Plan inWisconsinAdvanced Premium Tax Credit (APTC) Grace PeriodMembers who receive an advanced premium tax credit (APTC) to help with their healthcare premiumsare eligible for a grace period of up to three months if they have paid the premium for the first month ofcoverage. These members are the only HealthPartners members eligible to receive a three-month graceperiod.For services provided during month one of grace period:HealthPartners accepts responsibility and processes claims in a timely manner according to thebenefits. HealthPartners claim payment is not dependent on whether or not the member pays thepremium.For services provided during months two and three of grace period:HealthPartners will pend claims with status code 766: Services were performed during a HealthInsurance Exchange (HIX) premium payment grace period.If the member pays the full premium due before the end of the third month of nonpayment,HealthPartners will process pending claims according to the benefits.If the member does not pay the full premium due within the required time frame, HealthPartners willdeny pending claims and cancel the member retroactively, effective the last day of month one of thegrace period. The member is eligible to reenroll at the next open enrollment period.Non-APTC-eligible members who are responsible for their full premium payment are eligible for a 31-daygrace period for nonpayment.HealthPartners will pend these grace period claims with status code 734: Verifying Premium Payment.To check claims status, providers use a 276/277 electronic data interchange (EDI) transaction or theClaim Status Inquiry application on the HealthPartners Provider Portal.Questions and AnswersQ1: Would you provide an example of the three-month grace period in action for an May4
2022 Provider Resource ManualPlan is effective01/01/14.Premium forFebruary is notpaid.Premium has beenpaid for this month.Grace periodbegins – monthone.Claims receivedfor January andFebruary servicedates are paid.Claims received forJanuary servicedates are paid.Premium forFebruary andMarch is notpaid.Grace periodcontinues –month two.Claims receivedwith January andFebruary servicedates are paid.Claims receivedwith Marchservice datespend with statuscode 766.Premium forFebruary-Aprilnot paid.Premium foris February-April isnot paid.Grace periodcontinues –month three.Claims receivedwith January andFebruary servicedates are paid.Claims receivedwith March andApril service datespend with statuscode 766.Graceperiodends on last dayof April.No longer inthree-monthgrace period.Claims receivedwith January andFebruary servicedates are paid.Claims withMarch and Aprilservice dates arereprocessed anddenied tomember liability.Member isretroactivelycancelledeffective02/28/14.Q2: Is there a unique timely filing requirement for submitting HealthPartners claims forAPTCeligible members who stop paying their premium, but are eligible for the three-monthgrace period?We look at the service date to determine our liability. For example, let’s say an eligible member pays hisor her premiums for January and February only. Claims submitted for January, February and Marchservices will be covered according to the member’s benefits as long as the claim is received within thetimely filing limit specified in your contract.Q3: Does HealthPartners recoup the money paid for those claims during the first month ofpremium nonpayment?No. HealthPartners assumes liability regardless of whether or not the member pays the premium.Q4: Can providers collect from APTC-eligible members at the time of services if they haven’t paidtheir premium?How providers manage patient collection is up to them. APTC-eligible members who do not pay thepremium in full within three months are financially responsible for paying for their services during thefinal two months of nonpayment. Remember:1/20225
2022 Provider Resource ManualWe assume liability and pay participating providers for services provided during the first monthaccording to the member’s benefits. These claims are paid in a timely manner.If a member eligible for the three-month grace period pays the premium in full before the grace periodends, we process pending claims according to their benefits. Claim payments are sent to participatingproviders.Q5: Could an APTC-eligible member receive more than one premium grace period in a calendaryear?Members are eligible for more than one grace period, regardless of whether they are eligible for a3month or 31-day grace period. However, if a member reaches the end of the applicable grace periodand is terminated for nonpayment of premium, he or she may enroll again with HealthPartners or anyother Qualified Health Plan (QHP) only during an open enrollment period.Q6: How do members present proof of premium payment if requested by our medical facility?Members may create or sign into their secure web account at healthpartners.com and print or obtainproof of payment. If members require assistance with their web account, they may call theHealthPartners Web Support Help Desk at 952-853-8888 or 877-726-0203.How to submit a claim to HealthPartnersSubject: Electronic capabilitiesEffective: January 2000Last Updated: August 2009Reviewed: October 2020Explanation:HealthPartners offers many electronic capabilities for our providers.Administrative process:Minnesota Statute, section 62J.536 requires all health care providers to submit health care claimselectronically, including secondary claims, using a standard format effective July 15, 2009.The law applies to all health care providers that provide services for a fee in Minnesota and who areotherwise eligible for reimbursement under Minnesota Medical Assistance (Medicaid).Please review the FAQ article on the MDH website for more information regarding applicability of thestatute at x.html.For additional information, please visit healthpartners.com/electronicconnectivity.The entire law is available online at the Minnesota Department of Health (MDH) index.html.1/20226
2022 Provider Resource ManualHealthPartners offers electronic capabilities for our providers in the following areas:Electronic Claims SubmissionElectronic Remittance AdviceElectronic Eligibility InquiryElectronic Claims InquiryOnline Member Eligibility and Co-Payment Information OnlineClaim Status InquiryOnline Referral Entry and InquiryOnline Provider Reference InformationPlease contact your provider representative at HealthPartners for more details or ect: CMS 1500/5010 837 professional claims submissionEffective: January 2000Last Updated: August 2009Reviewed: October 2020Explanation:HealthPartners follows guidelines outlined in the Minnesota Companion Guides and in the NUCC 1500manual for submission of claims. The Minnesota Companion Guides can be accessed athealth.state.mn.us/facilities/auc. The National Uniform Claim Committee website can be accessedat nucc.org.Subject: UB04/5010 837 institutional claims submissionEffective: January 2000Last Updated: August 2009Reviewed: October 2020Explanation:HealthPartners follows guidelines outlined in the Minnesota Companion Guides and in the NUBCUB04 manual for submission of claims. The Minnesota Companion Guides can be accessed athealth.state.mn.us/facilities/auc. The National Uniform Billing Committee website can be accessedat nubc.org.Subject: Hospice claims submissionEffective: February 1, 2021Last Updated: January 2021Reviewed: January 20211/20227
2022 Provider Resource ManualExplanation:The preferred methods to submit claims for HealthPartners Hospice are by:Fax: 1-651-430-8505Email: tners Hospice claims can also be mailed to:5803 Neal Avenue NorthAttention: HealthPartners Hospice Billing OfficeOak Park Heights, MN 55082For any claim inquiries please call 952-883-6877.Subject: Submitting a Refund to HealthPartnersEffective: January 2021Last Updated: January 2021Reviewed: January 2021Explanation:When an overpayment is received and a refund needs to be submitted to HealthPartners, please includethe following information:Member nameMember numberEncounter/Claim numberBilled amount of claimReason for refundSubmit the refund to:HealthPartners Attn: Refund/RecoveryPO Box 1289, Minneapolis, MN 55440-1289Subject: Timely filing of claimsEffective: January 2000Last Updated: April 2003Reviewed: October 2020Explanation:HealthPartners contracted providers must submit claims within the specified period of the date of serviceas outlined in their provider contract.Administrative process:HealthPartners contracted providers have language in their contracts that state as a condition ofpayment, they must submit all claims for services, other than claims pended for coordination of benefits,to HPI or its Affiliate within a specified period of the date of service. Claims requiring coordination of1/20228
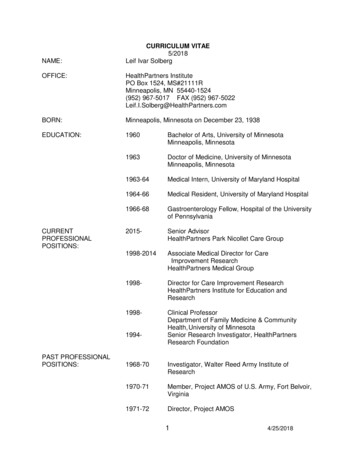
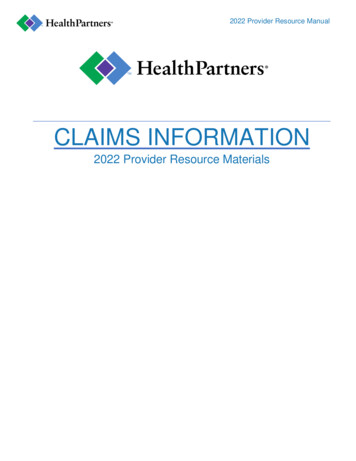
2022 Provider Resource Manualbenefits shall be submitted within sixty (60) days of determining HPI’s or its Affiliates’ obligation to makepayment. In HealthPartners’ appeal guidelines, a provider has 60 days from the remit date of the originaltimely filing denial to submit an appeal. If the appeal is received after the 60 days, a letter will be sentto the provider stating the appeal was not accepted.Subject: COB – Coordination of benefitsEffective: January 2000Last Updated: August 2009Reviewed: October 2020Explanation:HealthPartners follows guidelines for Coordination of Benefits that are outlined in the MinnesotaCompanion Guides. The Minnesota Companion Guides can be accessed athealth.state.mn.us/facilities/auc.Subject: Present on admission indicatorsEffective: January 1, 2009Last Updated: November 2008Reviewed: October 2020Explanation:HealthPartners requires acute care hospitals that are contracted under a DRG methodology to submita Present on Admission (POA) indicator for all claims involving inpatient admissions. This policy iseffective with admissions on or after January 1, 2009.Administrative process:POA values and submission requirements should follow NUBC billing guidelines.Subject: Remittance advice and template, HIPAA version 5010Document Added: October 2011Reviewed: October 2020See next page for sample remittance.For more information on HIPAA Remittance codes visit wpc-edi.com.1/20229
2022 Provider Resource Manual
1/202211
2022 Provider Resource ManualHealthPartners paper remit field descriptionsHIPAA version 5010ElementAField namePayer Nameand Address,LabelnoneUsageHealthPartners name, address835 ElementN102 whereN101 PRN3,N4BPayer contactCONTACTHealthPartners name of businesscontact area and contact phonenumbers for local and longdistance.PER wherePER01 CXCPayer IDPAYER ID1 followed by TINBPR10TRN03DSupplementalIDSUPPLEMENTALIDField contains the BANK IDassociated to the payment. BANKcan be used to identify product lineand to reconcile multiple remits tothe same vendor.TRN04EPayee Nameand AddressPAYEEDefines the entity to which payment N102 whereis directed.N101 PEN3,N412
2022 Provider Resource ManualFPayee Tax IDPAYEE TAX IDFederal Tax ID or SSN assigned topayee.N104 whereN103 FI orREF02 whereREF01 TJ1/2022ElementField nameLabelUsage835 ElementGPayee NPIPAYEE NPINPI associated to payee.N104 whereN103 XXHPAYEE IDPAYEE IDPayer assigned ID – Payee IDassigned by HealthPartners. Thisprovides additional identificationinformation critical to vendorbalance that is not accommodatedby the NPI. A single NPI may havemultiple HPFIN’s associated to it.REF02 whereREF01 PQ1/202213
2022 Provider Resource ManualIProductionEnd CycleDatePROD DATEThe last date HealthPartnersadjudicated claims appearing onthis remittance advice.JCheck/EFTDateCHECK/EFT DTThis is the check issue date or inBPR16the case of a non-paymentremittance, the date the remittancewas generated. Required on the topof each page of a multipageremittance.ElementField nameLabelUsageDTM02 whereDTM01 405835 ElementKCheck/EFTtrace NumberCHECK/EFTThis is a trace number which isTRN02used to re-associate payments andremittances; must be a uniquenumber for this business purposebetween the payer and the payee.This is the check number, EFTpayment ID or in the case of a nonpayment remittance, a unique IDassigned to the remit.LPaymentAmountPAYMENTThis is the total amount of paymentthat corresponds to the remittanceadvice.BPR02The total payment amount for thisremit cannot exceed elevencharacters, including decimals(99999999.99). Although the valuecan be zero, the remit cannot beissued for less than zero dollars.MPaymentmethodPAYMENTMETHODDefines the way payment istransmitted: Check, EFT ornopayment.BRP04Values: CHK, ACH, NONN1/2022Page numberRemittance page numberNa14
2022 Provider Resource Manual1PatientControlNumberPAT CTRL #This is the first 20 bytes of theprovider assigned identifiersubmitted on the claim (CLM01). Ifan identifier was not submitted thevalue is defaulted to‘0’.CLP01This data element is the primarykey for posting the remittanceinformation into the provider’sdatabase.ElementField nameLabelUsage835 Element2Payer ClaimControlnumberCLM #This is the identifier assigned byHealthPartners that identifies theclaim submission. For 5010 formatthis value will be the same on theoriginal, void and the replacement.CLP073Claim statusCLM STATUSClaim status code and narrativedefinition.CLP02Usage of Denied status changed for5010-it is only used if the patient isnot recognized and the claim is notforwarded to another payer.Status 23 – not our claim,forwarded to additional payer(s)requires usage of crossover carrierStatus 1-3 processed as primary,secondary or tertiary are usedregardless of whether any part ofthe claim was paid.4Claim ChargeAmountCLM CHGThis is the total submitted chargesfor the claim. This amount can bepositive, zero or negative.CLP035Patient NamePATIENTIf claim was submitted in the 5010837 format, then this is thesubmitted patient name. Else this isthe name that identifies the patienton the claim. Format is last, firstmiddle initial. Field will be in bold.NM103,04,05,07 whereNM101 QC1/202215
2022 Provider Resource Manual6StatementFrom and ToDateCLAIM DTThis is the service date range thatapplies to the entire claim.7ClaimPaymentAmountCLM PAYMENTThis is the total amount paid on this CLP04claim by HealthPartners. Thisamount can be positive, negative orzero.ElementField nameLabelUsageDTM02 whereDTM01 232and 233835 Element8PatientIdentifierPATIENT IDIf claim was submitted in the 5010837 format, then this is thesubmitted patient ID. Else this isthe identifier assigned byHealthPartners that identifies thepatient. Field will be in bold.NM109 whereNM101 QC9Group orPolicyNumberGRPThis is the HealthPartners groupnumber associated to the patient’scoverage.REF02 whereREF01 1L10Claim filingindicatorCLM FILING INDCoded value, used to identifydifferent product lines within apayer.CLP0611PatientResponsibilityAmountPAT RESPThis is the total patientCLP05responsibility amount for this claim.Amounts correspond to adjustmentswith grouping code of PR.12ProviderliabilityPRV LIABTotal provider liability amountapplied to the claim other than theMNTAX or withhold amounts. Thetotal of claim and line leveladjustment amounts where theclaim adjustment grouping codeequals CO (excluding adjustmentreason codes 137 and 104).1/2022na16
2022 Provider Resource Manual1314ElementRenderingprovideridentifierREND PROV IDClaim received CLM RECEIVEDdateDTField nameLabelThis is the payer assigned IDnumber or the National ProviderIdentifier of the provider whoperformed the service. Required ifthe rendering provider identifier isdifferent than the payee ID.Element should contain the NPI orthe payer assigned ID number foratypical providers. Field containseither NPI or UMPI.NM109 whereNM108 XXDate claim was received by HPI.DTM02 whereDTM01 050UsageOrNM109 whereNM108 PC835 Element15Facility typeFACILITY TYPEFor the 5010-remit format, thisCLP08element is populated on all claimtypes. Required when theinformation was received on theoriginal claim. Professional anddental default to POS from first line.16ClaimFrequencyFREQSubmitted claim frequency.CLP09For 5010 remit format this elementis used on all transaction types andis required if submitted on theoriginal claim.171/2022Other liabilityOTHER LIABTotal other liability amount appliedto the claim. The total of claim andline level adjustment amountswhere the claim adjustmentgrouping code equals OA.na17
2022 Provider Resource Manual18PROVIDERTAXPRV TAXTotal MNTax payment amountapplied to the claim. The sum of allclaim and line level adjustmentsassociated to adjustment reasoncodes 137. For this field, the MNtaxpayment amount is not reflected asa negative, unless it is a voidedclaim.AMT02 whereAMT01 TIf no MNtax amount, then the valuewill equal zero.19MedicalRecordNumberMED REC #This is the provider assignedmedical record number that wassubmitted on the claim.REF02 whereREF01 EA20DiagnosisRelatedGroup CodeDRGThis element is specific toinstitutional claims and is presentwhen the adjudication consideredthe DRG code.CLP11ElementField nameLabel21DiagnosisRelatedGroup WeightDRG WGHTThis element is specific toinstitutional claims and is presentwhen the adjudication consideredthe DRG code.CLP1222CoverageCOV EXP DTexpiration dateIf claim is denied because of theexpiration of coverage, this is thedate coverage expired.DTM02 whereDTM01 03623WithholdTotal withhold amount adjustedfrom the claim. Sum of claim andline level amounts associated toadjustment reason 104.naWITHHOLDUsage835 ElementIf no withhold amount, then thevalue will equal zero.1/202218
2022 Provider Resource Manual24CoveredamountCOVEREDThis is the amount of chargesconsidered as eligible for coverage.AMT*AUThis is the sum of the originalsubmitted provider charges that areconsidered for payment under thebenefit provisions of the healthplan. This excludes chargesconsidered not covered (i.e., perday television or telephonecharges) but includes reductions topayments of covered services (i.e.,reductions for amounts over feeschedule and patient deductibles).25CORRECTED CORRECTEDPATIENTPATIENTNAMENM1*74If claim was submitted in the 5010837 format and the patient info doesnot match HealthPartnerseligibility, then this field contains thevalues that are different. Only theelements that are different arepopulated not necessarily the fullname.26Correctedpatient IDNM109If the claim was submitted in the5010 837 format and the patient IDdoes not match HealthPartnerseligibility, then this field contains thevalue from HPI eligibility.ElementCORRECTEDPATIENT IDField nameLabelUsage835 Element27CorrectedPriority PayerCORRECTEDPRIORITY PAYERThis is the name of the payer thatNM103 wherehas priority over HealthPartners inNM101 PRmaking payment. For 5010 remitformat, this element is onlypopulated when HealthPartners hasidentified a payer primary to theHPI coverage, and the COB loopwas not submitted on d for 5010 when a prioritypayer has been identified.NM103 NM104WhereNM101 GB1/202219
2022 Provider Resource Manual29BILLINGPROVIDER:BILLINGPROVIDER:Subsidiary provider ID, used whenpayment is made to other than thebilling entity. For the 5010-remitformat this element is populatedwhen the submitted billing NPI isdifferent than the payee NPI.30Crossovercarrier nameCROSSOVERCARRIERRequired when the claim isNM103 wheretransferred to another carrier orNM101 TTcoverage (CLP02 19,20,21 or 23).31Crossovercarrier IDIDRequired when the claim istransferred to another carrier orcoverage (CLP02 19,20,21 or23).NM109 whereNM101 TT32PatientsMedicaidIdentifierPMIMEDICAL ASSISTANCE NUMBERREF 02 whereREF01 1W33Contract Code ContractThe contract that was usedbetween the payer and the providerto determine payment. Populatewith CIGNA misdirect messagewhen claim should have beensubmitted under the CIGNAcontract or the PMAP programcode.REF01 whereREF02 CEElement34Field nameLabelRemark codes REMARK CODESUsageTS301835 ElementMIA/MOAThis is a code used to relayinformational messages that cannotbe expressed with a claimadjustment reason code alone orare not associated to a dollaradjustment. Claim can contain up tofive claim level remark codes.For Non-MN providers, field maycontain an internal remit remarkcode.1/202220
2022 Provider Resource Manual35.1Element1/2022ClaimadjustmentamountField nameCLM ADJ AMTLabelThis is the adjustment amountCASassociated to the adjustmentgrouping code and reason code.There can be multiple adjustmentamounts per claim. The totalsubmitted charges minus the sumof the claim level adjustmentamounts and the line leveladjustment amounts must equal theClaim payment amount. Note:positive adjustment amountdecreases payment and a negativeadjustment amount increasespayment.Usage835 Element21
2022 Provider Resource Manual35.2ClaimAdjustmentgroup codeGRP CDThis code categorizes theCASadjustment amount. The values areas follows:CO Contractual Obligations – Usethis code when a joint payer/payeecontractual agreement or aregulatory requirement resulted inan adjustment.OA Other adjustments – avoidusing OA except for businesssituations defined in HIPAA guide.PI payer Initiated Reductions – Usethis code when, in the opinion of thepayer, the adjustment is not theresponsibility of the patient, butthere is no supporting contractbetween the provider and thepayer.PR Patient Responsibility35.3Claimadjustmentreason codeCLM ADJ RSN CD This code defines the reason for the CASadjustment amount.a)Line ItemcontrolnumberLINE CTRL #Line item identifier submitted by the REF02 whereprovider to identify the line or, ifREF01 6Rcontrol number is not submitted,then the claim line number.b)Dates ofServiceDOSThis is the date range of services for DTM02each line. Format isMMDDCCYY-MMDDCCYY.Element1/2022Field nameLabelUsage835 Element22
2022 Provider Resource Manualc)RevenueCodeREVElement applies to institutionalclaims only. This is the revenuecode submitted on the claim line.SVC04 sADJUDICATEDPROD/SVC/MODThis is the adjudicated procedurecode and modifiers. Values can beHCPC or ADA sSUBMITTEDPROD/SVC/MODIf the code used for adjudication isdifferent than the submitted value,then the submitted value iscontained in this element.SVC06f)Line ItemCharge orBilled AmountCHARGEThis is the line item charge/billedamount that was submitted on theline.SVC02g)Units#This is the number of paid units ofservice.SVC05h)APCAPCElement applies to institutionalonly. A value is present ifadjudication considered the APC.REF02 whereREF01 APCi.1ClaimAdjustmentAmountADJ AMTThis is the adjustment amountassociated to the adjustmentgrouping code and reason code.There can be multiple adjustmentamounts per line. The totalsubmitted charges minus the sumof the claim level adjustmentamounts and the line leveladjustment amounts should equalthe Claim payment amount. Note:positive adjustment amountdecreases payment and a negativeadjustment amount increasespayment.CASElement1/2022Field nameLabelUsage835 Element23
2022 Provider Resource Manuali.2ClaimAdjustmentGroupingCodeGRP CDThis code categorizes theCASadjustment amount. The values areas follows:CO Contractual Obligations – Usethis code when a joint payer/payeecontractual agreement or aregulatory requirement resulted inan adjustment.OA Other adjustments – avoidusing OA except for businesssituations defined in HIPAA guide.PI payer Initiated Reductions – Usethis code when, in the opinion of thepayer, the adjustment is not theresponsibility of the patient, butthere is no supporting contractbetween the provider and thepayer.PR Patient n CodeField nameCLM ADJ RSN CD This code defines the reason for the CASadjustment a
2022 Provider Resource Manual 1/2022 3 Claims submission - general HealthPartners contracted providers have language in their contracts stating as a condition of payment