Transcription
Care Transitions in Action: From Hospitalto Home in Two CommunitiesMarch 30, 2011U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, ADMINISTRATION ON AGING, WASHINGTON DC 20201PHONE 202.619.0724 FAX 202.357.3523 EMAIL AffordableCareAct@aoa.hhs.gov WEB www.aoa.gov
Agenda Introductions/housekeepingChicago: The Bridge Model––––– Robyn Golden, Rush Older Adult ProgramsRobert Mapes, AgeOptionsWalter Rosenberg, Rush Older Adult ProgramsIlana Shure, Aging Care ConnectionsLouise Starmann, Aging Care ConnectionsAkron: Care Transitions Programs– Dr. Kyle Allen, Summa Health System– Carolyn Holder, Summa Health System– Joseph Ruby, Area Agency on Aging 10B Inc. ResourcesNext trainingQuestions & answers2
The Bridge ModelHospital‐Community Partnerships in a Social Work Transitional Care Model
Overview Overview of the aging network in IllinoisIllinois Transitional Care ConsortiumADRC Care Transition GrantBridge ModelConnecting to hospitalsMaking the business case for care transitionsPolicy developments4
The Aging Network in Illinois Illinois Department on Aging (IDOA) ‐‐ first cabinet levelDepartment in the nation Thirteen Illinois area agencies on aging (AAA) – not for profitexcept for the City of Chicago. System reaches over 500,000persons yearly and partners with 300 community basedservice agencies offering meals and a wide variety of servicesand information Care Coordination Units (CCU) established by IDOA and theAAAs to provide universal pre‐screening of home boundpatients, in‐home assessments (under Medicaid WaiverProgram), care planning and often elder abuse and neglectinterventions5
The ITCC was formed to more effectively address needs of olderadults transitioning from the hospital to the community bylinking hospital based services with the aging networkthrough intensive care coordination.6
ITCC members Community‐based organizations– Aging Care Connections– Shawnee Alliance for Seniors– Solutions for Care Hospitals– Rush University Medical Center– MacNeal Hospital– Adventist LaGrange Memorial Hospital– Herrin Hospital– Carbondale Memorial Hospital Research, Evaluation & Policy– University of Illinois at Chicago, School of Public Health– Health & Medicine Policy Research Group7
Advisory Board Jean Bohnhoff ‐ Executive Director, Effingham County Committee on AgingThomas Cornwell ‐ Medical Director, HomeCare PhysiciansBob Clapp ‐ Senior Vice President, Hospital Affairs, Rush University Medical CenterJim Durkan – President & CEO, Community Memorial FoundationKaren Freda ‐ Executive Director, Illinois Council of Case Coordination UnitsMichael Gelder ‐ Senior Health Policy Advisory to Illinois Governor Pat QuinnMichael Koronkowski – Pharmacist and Geriatrics Professor, University of Illinoisat ChicagoJonathan Lavin – President & CEO, AgeOptions, Suburban Cook County AreaAgency on AgingPatricia Merryweather ‐ Vice President, Illinois Hospital AssociationMarta Pereyra ‐ Coalition of Limited English‐Speaking ElderlyCheryl Schraeder ‐ Director of Policy & Practice Initiatives, Institute for HealthcareInnovation, University of Illinois at Chicago College of NursingPatricia Volland ‐ Senior Vice President, Strategy & Business Development, TheNew York Academy of MedicineRebecca Zuber ‐ President, Rebecca Zuber, Inc.8
ADRC Care Transitions Grant Expand the Bridge Program to serve persons withdisabilities under age 60, in addition to older adults60 years and older Implement the expanded Bridge Program at 3 ITCCsites– Mac Neal Hospital (CCU partner: Solutions for Care)– Adventist LaGrange Memorial Hospital (CCU partner:Aging Care Connections)– Rush University Medical Center (CCU partner: CentralWest Case Management)9
ADRC Role in Promoting ImprovedCare Transitions Suburban Cook County ADRC– AgeOptions– Progress Center for Independent Living Training and Programs– Specialized training in working with people with disabilities– Plan, coordinate and fund support services– Evidence‐based health promotion (CDSMP) Coordination– Informed funded agencies about the Bridge model and upcominggrants– Coordinated outreach to hospitals10
The Bridge Model11
The Bridge Model Overview of Components–––––Social‐worker Based: Bridge Care CoordinatorInterdisciplinary TeamsHospital Æ HomePatient Focused, Community‐SpecificPartnership between Community‐Based Organization andHospital The Aging Resource Center Urban, Suburban, and Rural applicability12
Patient admitted into a hospitalAfter hospital admission the Bridge Model Care Coordinators receivepatients in one of two ways: Risk‐screen incorporated into hospital electronic medical record (EMR) producing dailyreport of upcoming discharges that fit criteriaDirect referral made by discharge planner or family member walking into an Aging ResourceCenter (ARC) located on‐site at hospitalAfter receiving a referral, a pre‐discharge assessment takes place: Bridge Care Coordinators meet with full or partial interdisciplinary team in charge ofpatient’s hospital care and participate in pre‐discharge rounds, discussing possible post‐discharge needs that may ariseWhere possible, interim in‐home services ordered to decrease time for start of neededservices13
Patient returns homePatient is re‐assessed 48 hours after returning home and Bridge Care Coordinators intervene toaddress identified issues Bridge Care Coordinators coordinate all of the following:– Ability to follow‐up with discharge plan of care– Clarify any confusion over medication regimen– Follow‐up with primary care physician in the community– Help to make and attend follow‐up medical appointment(s)– Promptly set‐up appropriate in‐home services– Communicate with Home Health and/or other community service providers to ensuretimeliness and address mistakes (wrong addresses/times, etc.)– Assist referred patients with psychosocial needs, including depression, adjustment tochange, caregiver burden/stress, etc. with short term counseling or appropriate referral14
Building off Aging Network Conducting Choices for Care Assessments and ComprehensiveCare Coordination Assessments (Standardized casemanagement assessments utilized throughout Illinois) Setting up Medicaid Waiver Interim Services and/or othercommunity‐based services as need– Referrals made to both private and public agencies Providing and referring families for Caregiver Support Servicesand Respite Conducting Benefits Check‐Ups Providing Information & Assistance to Patients and theirfamilies on site (i.e. Medicaid, Food Stamps, Circuit Breaker,Tax Freezes, Medicare Part D, Home Modification, FSS)15
Bridge Care Coordinators16
The Post‐Discharge Environment17
Psychosocial Issues Social isolationDepressionDifficulty coping with changeFinancial stressorsLanguage barriersHealth literacy barriersOlder generations taught to be “goodpatients”18
Bridge Care Coordinators Why Social Workers?– Systems Theory– Biopsychosocialframework– Psychosocialdeterminants ofhealth19
Evidence Base Rush Enhanced Discharge Planning Programrandomized controlled trial N 720– Referrals generated through electronic medical record atdischarge– June 2009 to March 201020
Outcomes 30, 60, 90, 120, 180 days readmission Increase access to formal services Decrease time between discharge and start ofservices Follow‐up physician appointments Increased understanding of purpose of prescribedmedication Greater understanding of responsibilities formanaging own health Decreased mortality21
Aging Resource Center (ARC)22
The Role of the ARC Symbol of hospital‐community collaboration Greater ability to interface with the community– Creates continuity for the patient across healthcare silos Promotes the notion of “systems” approach todischarge planning Maximizes the opportunity for a servable moment23
24
25
Establishing an ARC Time frames for developing the ARC Outreach to hospital– Through existing programs or contracts alreadyestablished Begin contacting individuals at the hospital who aresupportive of the model.26
Establishing a Partnership1. Evaluate Potential Partners2. Make the “ASK”–Identify what you are asking the partner to contribute3. Establish the basic structure of the partnershipprior to launching the project–Keep parameters loose enough to allow for growthdevelopment4. A Memorandum of Understanding (MOU) at aminimum should be in place prior to the start dateof the project27
Establishing a Partnership (continued) Legal agreements should be created broadly definingthe service provision, the recipient of the service andduties of each partner in the relationship including:––––––Purpose of the programResponsibilities of both partiesIndividual responsibilities of the partnersFinancial liabilitiesConfidentiality and data sharingTerminationAnnually review agreement!28
Lessons Learned Integrate at all levels of the hospital system– Front desk reception to Regional Director Be patient and persistent– Guest versus Team Member Troubleshoot challenges before they becomebarriers Learn both cultures and languages– Network, network, network29
Community‐Hospital Partnerships Aging Care Connections (CCU ‐ Suburban Chicago)– Adventist LaGrange Memorial Hospital Shawnee Alliance for Seniors (CCU – Rural,downstate Illinois)– Carbondale Memorial Hospital– Herrin Hospital Solutions for Care (CCU – Suburban Chicago)– Mac Neal Hospital Central West (CMU – Chicago)– Rush University Medical Center30
Building the Business Case The evidence must be translatedinto a business case(M. D. Naylor and J. A. Sochalski, Scaling Up: Bringingthe Transitional Care Model into the Mainstream,The Commonwealth Fund, November 2010)– Identifying clinical and economicoutcomes– Comparing quality and cost outcomes Reduced hospital readmissions andEmergency Department (ED) visits Appropriate outpatient follow‐up– Isolating essential program elements tocreate efficiencies31
Building the Business Case (continued) Making case for improving quality and reducing costto position as “compelling solution for the payercommunity”1– Private purchasers– Insurers– Public payers Providers Get consumer to ask for program– Need to know they should expect transitional care32
Influencing and Interpreting Policy Evidence and business case create platform foradvocacy and policy change New health care policies include transitions, butrequire interpretation and innovation–––––Community Based Care Transitions ProgramsReducing 30‐Day ReadmissionsPiloting Bundled PaymentsCreating Accountable Care OrganizationsEncouraging Medical Homes33
Bundled Payments Bundled payment pilot to begin by 2013– Single Medicare payment will cover all services for anepisode of care to be distributed among care providers: Acute hospital servicesPhysicians’ servicesCare coordination and transitional care servicesPost‐acute services– Home health care– Skilled nursing facility services– Inpatient rehabilitation services34
Accountable Care Organizations Medicare Shared Savings Program creates incentivefor the establishment of Accountable CareOrganizations (ACOs)– Networks of physicians and other providers– Share savings resulting from the ACOs coordinated care Reduced Medicare expenditures Improved beneficiary health outcomes35
Medical Homes Encouraging Medical Homes– Interdisciplinary teams contracting with primary carephysicians to provide supportive services to eligiblepatients: Care coordination Case management Health promotion Transitional care Patient and family support Referral to community services36
CMS and AoA Grants AoA made grant funding available for states– Strengthen the role of Aging and Disability ResourceCenters (ADRCs) in implementing evidence‐based caretransition models– Meaningfully engage older adults and people withdisabilities and their caregivers in care transitions– Illinois is a grant recipient CMS Transitions grant37
Thanks to The Bridge Model would not be possible without thesupport of:–––––––Administration on AgingCommunity Memorial FoundationSanofi AventisNew York Academy of MedicineHarry and Jeanette Weinberg FoundationMichael Reese Health TrustRetirement Research Foundation38
Contact Robyn Golden, Rush Older Adult Programs robyn golden@rush.edu Robert Mapes, AgeOptions robert.mapes@ageoptions.org Walter Rosenberg, Rush Older Adult Programswalter rosenberg@rush.edu Ilana Shure, Aging Care Connectionsishure@agingcareconnections.org Louise Starmann, Aging Care Connectionslstarmann@agingcareconnections.orgFor more information about the Illinois Transitional CareConsortium, visit http://www.transitionalcare.org39
Questions?40
Care Transitions in Akron
Area Agency on Aging Transitions How did we get here? Acute care setting Nursing facility setting42
How Did We Get Here? With an IDEA!–Identify Key Stakeholders–Develop Relationships–Explore Common Interests–Align efforts to achieve mutually desired outcomes43
Identify Key Stakeholders Consumers Taxpayers Payors– Policy‐makers– Managed Care Organizations Long Term Care Providers (nursing and assisted livingfacilities, home health agencies, AAA providernetwork) Hospitals Physician Leaders44
Develop Relationships Initiate dialogue with key players within stakeholderorganizations (use Board Members to identify andgain entrée) Use Board membership as a vehicle to buildengagement and commitment to mission and vision Make Board Governance (strategic direction andpolicy‐making) a meaningful experience45
Explore Common Interests Historically ––––Promote consumer choiceMedicaid cost containment (taxpayer value)Reduce permanent nursing facility placementIncrease length of stay in home and community‐basedprograms (i.e., waivers)46
Explore Common Interests(continued) Paradigm Shift: New Medicare Initiatives aimed atreducing utilization (Health Care Reform)– Reduce hospital admissions and readmissions– Reduce length of stay– Reduce emergency room visits47
Align Efforts to Achieve MutuallyDesired Outcomes Develop Hospital Transition Programs Develop AAA provider incentive payment plan toachieve desired Medicare outcomes (ACO model) Integrate care planning with Medicare AdvantagePlans Provide I&A to patients at physician practices48
Acute Care Setting TransitionsHospital Based Assessments Building on S.A.G.E. Hospital program success, AAA placednurses in Summa Akron City Hospital Further capitalizing on that success, we have nurseconsultants stationed weekly at 8 acute hospitals and aspecialty hospital and the Cleveland Clinic Wooster Campus, alarge physician practice that sees 800 Medicaid patients a day Nurse consultants work with patient care coordinators,discharge planners, and physicians to create a bridge to homein consultation with the patient and family Nurses also screen older adults for any AAA offered servicesand facilitate the enrollment process as part of dischargeplanning49
Acute Care Setting TransitionsCare Transitions Project Key driving force: Affordable Care Act Provided Health Coaching through a formalcollaboration with two local hospitals to reduceavoidable readmissions Built on the Hospital Based Assessor program toprovide evidence based health coaching50
Nursing Facility Care Setting TransitionsPATH Key Driving Force‐ Limited Waiver Enrollments Building on the 2004‐05 Administration on Aging grant tointegrate care management for common members ofPASSPORT and SummaCare Medicare Advantage Plans This grant allowed AAA to identify and address barriers tosuccessful integration with a Managed Care Organization(MCO) Outcomes of the grant included High Risk Screening tool,Care Management protocols, and a Geriatrician‐ledInterdisciplinary Team51
Nursing Facility Care Setting TransitionsPATH (continued) Building on our care management integration, wedeveloped our PATH Transitions Team which consistsof 3 Medical Social Workers in September of 2009 PATH worked with Summa Care’s in panel NF totransition older adults back to home and communitybased settings Notification sent to all nursing facilities informing ofPATH Team52
Nursing Facility Care Setting TransitionsPATH (continued) Began meeting with staff at targeted nursing facilities todiscuss our agency being an extension of their dischargeplanning team Follow individuals identified by Pre‐Admission Review asbeing 60 years of age and Medicaid eligible The PATH Team spends time in nursing facilities talking withresidents who wish to return to the community regardless ofage and assessing them for eligibility into PASSPORT andAssisted Living programs53
Results of PATH54
Next Steps SummaCare/Summit Physicians, Inc.‐Geriatric Medicine/AreaAgency on Aging Health Coaching partnership Additional transitions staff certified in Dr. Coleman’sevidence‐based model Evaluate impact on discharge to permanent nursing facilityplacement, hospital admissions and readmissions, emergencydepartment visits, etc. Continue developing relationships with nursing facilities andother partners55
Improving Care through Collaboration:Integration of the Aging Network andAcute and Post Acute Medical CareServices
The Partnership57
The S.A.G.E. Project(Summa Health System/Area Agency onAging, 10B/Geriatric Evaluation Project: ASuccessful Health Collaborative(Est. 1995)58
The SAGE Project A 15 year collaboration partnership Multiple initiatives, a “cast of thousands” (well, maybe 100s, but you getthe point) Common goal to improve the health, well being and functional status ofAkron region frail older adult population Identified major gaps in the continuum and care processes from eachpartner Searched and defined mutual benefits Shared mutual threats and concerns Built trust Grew and multiplied to other regional systems Communication, communication, communication Vision, Vision, Vision, Vision59
SAGE Goal Goal: To integrate acomprehensive geriatrichospital‐based clinicalprogram with thecommunity aging networkto improve the health,functional status, and toprevent institutionalizationof older adults at risk fornursing home placement. S.A.G.E. Project is anexample of how to partnerwith a community agency:– Acute hospital and medicalcare services and– A community‐based AreaAgency on Aging60
Area Agency on Aging Programs Mission: To provide older adults andtheir caregivers long‐term care choices,consumer protection and education sothey can achieve the highest possiblequality of life. Aging Resource Center PASSPORT Home Care Medicaid Waiver Assisted Living Medicaid Waiver Community Services Division– Care Coordination– Alzheimer’s Respite Program– Family Caregiver Support Elder Rights Division61
Who were the partners?Summa Health System Geriatric Medicine Department 6 Hospital SystemSumma Akron City HospitalSumma St. ThomasHospital– 2,027 licensed beds– 61,800 admissions Level 1 Trauma– 113,059 ED visits Community Locations– 4 outpatient health centers– Wellness Institute – medically‐based fitnessHealth Plan– 110,000 Covered Lives– 16,000 Medicare Risk HMO Major Teaching Residency andFellowship ProgramPost Acute/Senior Service LineSummaCare, Inc.Summa Western ReserveHospital– 10 Certified Geriatricians– 12 Geriatric Certified APNs Continuum of Care– Acute Care/Acute Rehab/ LTAC/SNF Beds– Home Care/ Hospice/ HomeInfusion/ HME62
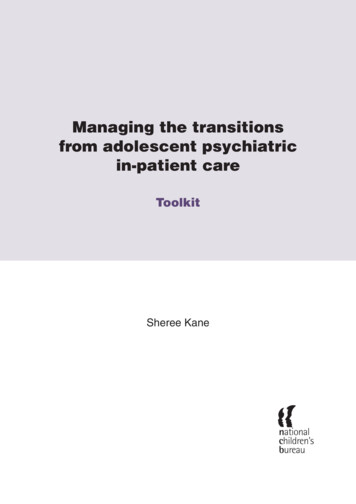
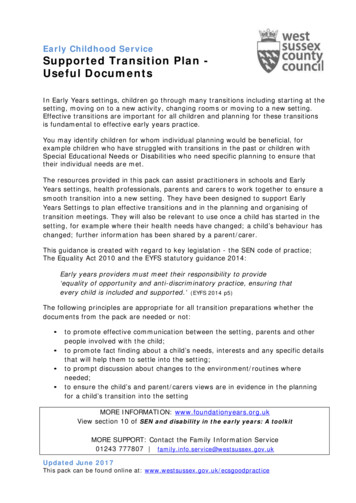
A ComprehensiveApproachHealth Services Research Care Innovations Institute ACE Project STEPS Care Trial AD-LIFE Trial Elder Abuse PEACE TrialEducation Geriatric Medical Education Geriatrics and Palliative MedicineFellowships Geriatric Education for Nursing andother disciplines Provide interdisciplinary teamtraining and support Geriatric Concepts OrientationProgram ACE Site Visits and ConsultationThe InstituteClinical Care The Center for Senior Health* Comprehensive Geriatric Assessment* Geropsychiatry* Falls and Balance Clinic* OT- ADL and Drivers Assessment* Urinary Incontinence* Neuropsychology InpatientACE UnitStroke UnitACE of HeartsPalliative Care Unit and ConsultsGeriatric Consult ServiceGeropsychiatry Unit Summa HomeCare & Home Infusion Palliative Care and Hospice Services SNF-Geriatric Rehabilitation Units House Call Program Transitional Care - “Bridge to Home”Community Collaborations Care Coordination Network SAGE Project: Area Agency on Aging Alzheimer’s Association Akron Regional Hospital Association Interdisciplinary Consortium for AgingResearch and Education (ICARE) Geriatric Mental Health Coalition Care Giver Institute
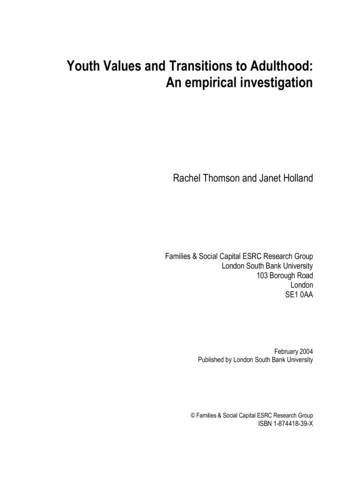
Wagner’s Chronic Illness Model:Change That WorksytiiesnciulomPdnasComceruoHealth SystemResOrganization of Health ePractice TeamImproved Functional and Clinical Outcomes64
Key Historical Collaborative Programs Interdisciplinary Community Aging NetworkCommittee (ICAN) ‐ forms and communicationprocesses. (1995) Imbedding AAA care managers in clinical sites, i.e.,Center for Senior Health and Acute Care for Elders(ACE) Unit. (1998) Widespread AAA RN Assessor Program. (2000)65
Key Historical Collaborative Programs(continued) Area Agency and ODA Grant: Integrated care planningfor Medicare Advantage health plan and AAA casemanagers. Used Appreciative Inquiry technique to buildrelationship. (2003) Care Management Interdisciplinary Team at the AAoAwith geriatrician and pharmacist (CMIT). (2006) Use of Extended Care Information Network (ECIN)between hospital and AAA case managers. (2008)66
Key Historical Collaborative Programs(continued) Integration of AAA RN assessor and case manager tolarge rural primary care office (2008) AHRQ funded ‐ After Discharge Management of LowIncome Frail Elderly (AD‐LIFE) Randomized Control Trial(RCT) (2005‐2009) NPCRC funded ‐ Promoting Effective Advance Care inthe Elderly (PEACE) RCT Pilot Trial. (2009)67
The AD‐LIFE Trial:After Discharge Care Management of LowIncome Frail ElderlyKyle R. Allen, DO, Summa Health System Health Services Research and Education InstituteKathy Wright, MSN, Summa Health System Health Services Research and EducationInstituteSusan Hazelett, MS, Summa Health System Health Services Research and EducationInstituteLynn Clough, MA, Summa Health System Health Services Research and Education InstituteDave Jarjoura, PhD, The Ohio State UniversityEugene Pfister, MD, Akron General Medical CenterAgency for Healthcare Research and QualitySupported by Grant # R01 HS014539Supported by Summa Foundation68
AD‐LIFE: A Model of Integrated CareThe AD‐LIFE Trial will test theeffectiveness of interdisciplinary caremanagement that integrates medical andsocial care to improve patients’ overallhealth and well‐being.69
PEACE TRIALPromoting Effective AdvancedCare for EldersKyle R. Allen, DO, Summa Health System, Health Services Research and Education InstituteSteven Radwany, MD, Summa Health System, Health Services Research and Education InstituteSusan Hazelett, MS, RN, Summa Health System, Health Services Research and Education InstituteDenise Ertle, MSN, RN, CNS, Area Agency on Aging 10B, IncSusan Fosnight, RPh, CGP, BCPS, Summa Health System, Health Services Research and EducationInstitutePamela Moore, PharmD, BCPS, Summa Health System, Health Services Research and EducationInstitutePatricia Purcell, MSN, RN, CN, The University of AkronBarbara Palmisano, MA, Northeastern Ohio Universities Colleges of Medicine and PharmacyRuth Ludwick, PhD, RN.C, CNS, Summa Affiliate, Robinson Memorial HospitalThe PEACE Trial is supported byThe National Palliative Care Research Center& the Summa FoundationArea Agency on Aging, 10B, Inc. Summa Health System NEOUCOMKent State University The University of Akron70
Purpose of the PEACE Pilot Study This randomized pilot study will determine thefeasibility of a fully powered study to test theeffectiveness of an in‐home interdisciplinarygeriatric‐ palliative care management intervention toimprove the quality of palliative care for consumersof Ohio’s community‐based long‐term care Medicaidwaiver program, PASSPORT.71
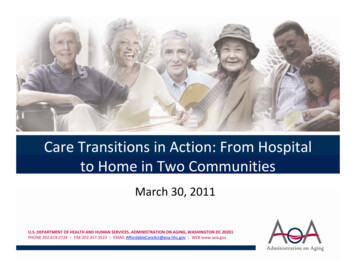
Transitions of CareAD‐LIFE, PEACE, and Bridge to HomeThe Center for SeniorHealth and SeniorServicesThe PrimaryCarePhysician Medical model Limited time with patientAD-LIFE,PEACE, & Consult and support acrossthe continuum includingoutpatient, inpatient, housecalls and skilled/long- termcareBridge toHomeThe Area Agency on Aging Social service model but nowbecoming more integrated Addresses medical andpsychosocial Post‐discharge caremanagement of low incomefrail elderly Nurse care manageractivation of client Collaboration between ahospital‐basedinterdisciplinary team, AreaAgency on Aging, and PCP Integration of acute andlong‐term care Transitional care to reducereadmissions Care management and services forlong-term care Limited interaction with PCP Addresses functional abilities/geriatricsyndromes but challenged with highrisk enrollees with multiple chronicillnesses AD-LIFE trial is supported by the Agency for Healthcare Researchand Quality Grant # R01 HS014539. PEACE is funded by theNational Palliative Care Research Center. Both are supported by theSumma Foundation. Bridge to Home is funded by SummaCare.72
Key Points No single organization can tackle complex social,community, human service problems in a silo Working in effective collaboration can overcomemany obstacles and barriers that lie beyond thescope of any single entity through sharing andcombining talents and creative solutions When done effectively “the whole is more than sumof the parts”– Outputs are greater– Synergy builds– Energy builds Effective collaboration is a team sport between twoor more organizations73
Good to Great and the Social Sectors:Why Business Thinking is Not the Answer (Jim Collins) Defining “Great”‐ Calibrating Success without business metrics Level 5 Leadership‐ Getting Things Done within a Diffuse PowerStructure First Who ‐ Getting the Right People on the Bus within SectorConstraints The Hedgehog Concept‐ Rethinking the Economic Enginewithout Profit Motive– What are you deeply passionate about?– What can you be the best in the world at?– What Drives your Resource Engine (time, money and brand) Turning the Flywheel‐ Building Momentum by Building theBrand74
Contact Kyle Allen, Summa Health System,allenk@summahealth.org Carolyn Holder, Summa Health System,holderc@summahealth.org Joseph Ruby, Area Agency on Aging 10B, inc.,jruby@services4aging.org75
Resources: Care Transitions ail.asp?itemID CMS1239313 (Community‐based Care TransitionsProgram) http://www.adrc‐tae.org/tiki‐index.php?page CareTransitions(AoA’s Aging and Disability Resource Centers and caretransitions) http://www.cfmc.org/caretransitions/Default.htm (CareTransitions Quality Improvement Organization Support Center) Final‐0216111.pdf (InnovativeCommunities report from the Long‐Term Quality Alliance)76
Resources: Affordable Care Act http://www.aoa.gov/Aging Statistics/Health care reform.aspx (AoA’s Health Reform web page – wherewebinar recording, transcripts and slides are stored) http://www.healthcare.gov (Department of Healthand Human Services’ health care reform web site) /temp/ bdsYKv:: /home/LegislativeData.php?n BSS;c 111 (Affordable CareAct text and related information)77
Next Training We will continue our webinar series in Aprilwith a continued focus on care transitions– Watch your email for date, time andregistration information78
Questions?79
Questions/Comments/Stories/Suggestions for Future WebinarTopics?Send them to:AffordableCareAct@aoa.hhs.gov80
- Ilana Shure, Aging Care Connections - Louise Starmann, Aging Care Connections Akron: Care Transitions Programs - Dr. Kyle Allen, Summa Health System - Carolyn Holder, Summa Health System - Joseph Ruby, Area Agency on Aging 10B Inc. Resources Next training Questions & answers