Transcription
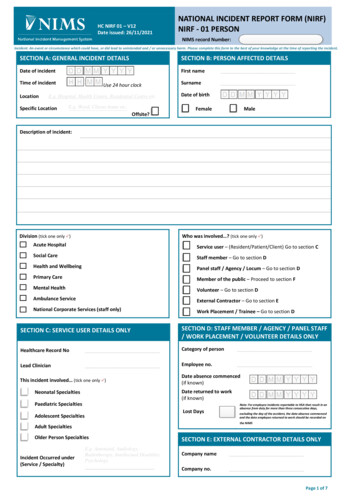
HC NIRF 01 – V12Date issued: 26/11/2021NATIONAL INCIDENT REPORT FORM (NIRF)NIRF - 01 PERSONNIMS record Number:Incident: An event or circumstance which could have, or did lead to unintended and / or unnecessary harm. Please complete this form to the best of your knowledge at the time of reporting the incident.SECTION A: GENERAL INCIDENT DETAILSSECTION B: PERSON AFFECTED DETAILSDate of incidentFirst nameSurnameTime of incidentLocationUse 24 hour clockE.g. Hospital, Health Centre, Residential Centre etc.Specific LocationE.g. Ward, Clients home etc.Date of birthFemaleMaleOffsite?Description of incident:Division (tick one only )Who was involved ? (tick one only )Acute HospitalService user – (Resident/Patient/Client) Go to section CSocial CareStaff member – Go to section DHealth and WellbeingPanel staff / Agency / Locum – Go to section DPrimary CareMember of the public – Proceed to section FMental HealthVolunteer – Go to section DAmbulance ServiceExternal Contractor – Go to section ENational Corporate Services (staff only)Work Placement / Trainee – Go to section DSECTION C: SERVICE USER DETAILS ONLYSECTION D: STAFF MEMBER / AGENCY / PANEL STAFF/ WORK PLACEMENT / VOLUNTEER DETAILS ONLYHealthcare Record NoCategory of personLead ClinicianEmployee no.This incident involved (tick one only )Date absence commenced(if known)Date returned to work(if known)Neonatal SpecialtiesPaediatric SpecialtiesLost DaysAdolescent Specialtiesexcluding the day of the accident, the date absence commencedand the date employee returned to work should be recorded onthe NIMSAdult SpecialtiesOlder Person SpecialtiesIncident Occurred under(Service / Specialty)Note: For employee incidents reportable to HSA that result in anabsence from duty for more than three consecutive days,SECTION E: EXTERNAL CONTRACTOR DETAILS ONLYE.g. Antenatal, Audiology,Radiotherapy, Intellectual Disability,PsychologyCompany nameCompany no.Page 1 of 7
SECTION F: WHAT WAS THE OUTCOME AT THE TIME OF THE INCIDENT? OutcomeNear Miss e.g. Nearly given wrong drugNo Injury e.g. Wrong drug given but no harmoccurredInjury not requiring first aidBody Part AffectedCategory 3Injury or illness, requiring first aidInjury requiring medical treatmentE.g. Arm, Spine, Lung, Other PhysiologicalCategory 2Long-term disability / Incapacity (incl. psychosocial)Permanent Incapacity (incl. Psychosocial)Category 1DeathSECTION G: TYPE OF INJURY (tick one only )Birth Specific Injury(Baby)Birth Specific Injury(Mother)Blood Specific InjuryDiagnosed DiseaseDisorder or Cond.Diagnosed InfectionGeneral InjuriesHearing / Sight InjuryMisdiagnosisMusculoskeletal/ Soft TissuePersonal LossSurgery SpecificInjuryTraumatic/EmotionalHC NIRF-01Apgar score 5@ 1 min &/or;7@5mins &/or pH 7.0AspirationCerebral irritability / neonatalseizureHIE - Hypoxic IschaemicEncephalopathy with HypoglycaemiaHIE Grade 1 - Hypoxic IschaemicEncephalopathyHIE Grade 2 - Hypoxic IschaemicEncephalopathyHIE Grade 3 - Hypoxic IschaemicEncephalopathyHypoglycaemia - severeKernicterusNeonatal deathNerve Injury - brachial plexus (incl.Erbs Palsy)Nerve Injury - faceOther unexpected deteriorationStillbirthSub-galeal / ctomy (Perinatal)Incontinence (faecal)Incontinence (urinary)Excessive BleedingFaintingImmunological haemolysisAsbestosisCancerAcute Radiation SyndromeNarcolepsy/CateplexyPerineal tearPost-Partum HaemorrhageRhesus iso-immunisationIncontinence (faecal & urinary)Febrile non-haemolytic transfusionreactionUnknownUterine nownDermatitisTBPleural PlaquesOtherClostridium BLAllergic Reaction (incl. anaphylaxis)Cut / Laceration / Graze / scratchBrain Injury / ConcussionDeathBurn / scald / corrosionDental injury &/or lossChoking / asphyxiaDeteriorationCirculatory / volume depletionHaemorrhageCirculatory / volume overloadBlisterPain/DiscomfortHearing Impairment / lossTinnitusSight Impairment / nFractureBruisingRepetitive Strain Injury (RSI)CrushingSlipped / Prolapsed DiscDental Fracture / Tooth lossSprain / StrainDislocationSoft tissue injuryP. Ulcer Stage 1: Intact skin with non-blanchable redness over bony prominenceP. Ulcer Stage 2: Part thickness dermis loss: blister/open ulcer/no sloughP. Ulcer Stage 3: Full thickness tissue loss: /- visible subcutaneous fatP. Ulcer Stage 4: Full thickness tissue loss/necrosis: exposed bone/tendon/muscleAdditional / Further SurgeryLoss of Wages / Income /Limb DeformityBusinessDefamation of CharacterLoss of ConsortiumDamage to organ / body partLoss of organ / body partDental Damage / LossNerve injury / Loss ofForeign body left in situFunctionUnknownInadequate anaesthesiaAnxiety / TraumaStressPTSDUnknownNon-immunological haemolysisOtherVREVRSAOtherMalaise / NauseaNerve injury / Loss of FunctionPuncture / biteRash / irritationUnknownOtherOtherOtherSwelling / InflammationUnknownWhiplashOtherUnknownOrgan RetentionOtherUnexpected complication /deteriorationOtherWorried WellOtherPage 2 of 7
SECTION H WHAT TYPE OF HAZARD DID THIS INCIDENT RELATE TO? (Tick one option from Steps 1, 2, 3 & 4)Step 1.DiagnosisStep 2.Diagnosis TypeDelayed DiagnosisMisdiagnosis/Incorrect DiagnosisMissed tage of CareCommunityOutpatient/EDInpatientStage of CarePre ProcedureIntra ProcedurePost ProcedureStep 3.Care st InterpretationCare eatment/InterventionCare eatment/InterventionName of Initial Proceduree.g. cannulation, colonoscopyClinical CareName of Subsequent Procedure (e.g if required return to theatre)e.g. EUA, hysterectomyLabour/DeliveryHC NIRF-01Delivery typeCaesarean Section (Elective)Caesarean Section (Emergency)Instrumental Delivery (Forceps)Instrumental Delivery (Vacuum/Ventuse/Kiwi)Instrumental Delivery (MultipleInstruments)Non Instrumental DeliveryCare eatment/InterventionStep ntationEquipmentUnknown/otherLack of availabilityNot performed when indicated/DelayedAdverse event/patient safety DocumentationEquipmentUnknown/otherLack of availabilityNot performed when indicated/DelayedPre-existing medical conditionRetained foreign objectWrong body part/site/sideWrong patientWrong process/treatment/procedureAdverse event/patient safety DocumentationEquipmentUnknown/otherLack of availabilityNot performed when indicated/DelayedRetained foreign objectWrong body part/site/sideWrong patientWrong process/treatment/procedureAdverse event:Cord ProlapseEclampsiaLow Apgars/Cord PHPlacental AbruptionPPHShoulder DystociaUterine RuptureOtherAdverse event requiring transfer/return to theatre:Cord ProlapseEclampsiaLow Apgars/Cord PHPlacental AbruptionPPHShoulder DystociaUterine sentDocumentationEquipmentUnknown/otherLack of availabilityNot performed when indicated/DelayedRetained foreign objectWrong process/treatment/procedurePage 3 of 7
SECTION H WHAT TYPE OF HAZARD DID THIS INCIDENT RELATE TO? (Tick one option from Steps 1, 2, 3 & 4)Step 1.MedicationStep 2.Route of administrationOralIntravenousSub CutaneousIntra MuscularTopicalRectalInhalationOther / UnknownStep 3.AdministrationMonitoringOrdering / Supply / TransportPreparation / geClinical CareWhat medication was involved?Medication OneMedication TwoNutritionParenteralEnteralSpecial DietGeneral DietOtherBlood / BloodProductWhole BloodRed CellsPlatelet (Apheresis)Platelets (Pooled)OtherDiagnosticRadiology (DR)& NuclearMedicine (NM)Bio HazardsRadiotherapyHC NIRF-01BiologicalHazards /AcquiredInfectionsChecking Patient IDprocedureClinical Details onReferralCommunication /ConsentDocumentation /RecordsEquipmentPerforming procedurePregnancy StatusUnknownBacteriaFungus / MouldPrionVirusOrganism UnknownStep 4.Adverse Drug ReactionContra-indicatedDrug InteractionFailure / Malfunction of equipmentIncomplete / InadequateNot preformed when indicated /delayedOmitted/Delayed DoseWrong Dose / StrengthWrong DrugWrong Formulation / RouteWrong FrequencyWrong Label / InstructionsWrong PatientWrong Quantity / DurationCommunication / ConsentPrescribing / RequestingPreparation / DispensingAdministrationStorageDocumentation / RecordsEquipmentSupply / Ordering / TransportPresentation / PackagingTransfusing bloodOtherDiagnostic Exposure intendedX-ray Over ExposureWrong body part / sideDose to comforters / carersAdverse EffectIncomplete / InadequateNot performed when indicated / DelayWrong ConsistencyWrong Diet / Wrong Blood ProductWrong Process / Treatment / ProcedureWrong PatientLack of AvailabilityWrong dispensing label / instructionsInappropriate for task / Wrong deviceOtherWrong PatientInadvertent dose to foetus 1mSv 1mSvTotal dose or Volume VariationDose (NM) or Volume Variation(1 fraction)Wrong DrugWrong DoseWrong Process / Treatment /InterventionFailure / MalfunctionInadvertent deterministic effects 10%10-20% 20%Please Specify, if knowne.g COVID-19, MRSA, etcAbove Notifiable levelsBelow Notifiable levelsExposure to Bite (Human)Exposure to Bite (Insect / Animal)Exposure to Bodily FluidsExposure to Ingestion/Food/WaterExposure to Needle StickExposure to Skin ContactInhalation/AirborneEquipment, Implements, Facilities, Sharps(Non Needle)UnknownOtherPage 4 of 7
SECTION H CNTD: WHAT TYPE OF HAZARD DID THIS INCIDENT RELATE TO? (Tick one option from Steps 1, 2 & 3)Step 1.Behavioural HazardsSelf-InjuriousBehaviourViolence,Harassment andAggressionChild AbuseAdult AbuseStep 2.IntentionalUnintentionalBy a Family Member / RelativeBy a Member of the PublicBy a Peer / StudentBy a PrisonerBy a Service UserBy a Staff MemberPlease specify name ofinstigator/aggressorSlip / Trip / FallPhysical HazardsNon Mechanical(Incl. Person /Animal)Ergonomics(Incl. manual /people handling)MechanicalComponentsTemperature(Excluding Fire)FireVibrationElectricalNoiseRadiationHC NIRF-01From HeightFrom Equipment / FurnitureSame Level / GroundOn StairsOn StepsOtherObject / Tools (Non Sharps)Sharps (Non Needle)OtherPersonManual HandlingOtherPatient HandlingPhysical InterventionCatering equipmentDoor / Gate / BarrierHealthcare EquipmentLifting Equipment / AccessoriesOffice / Business equipmentHotColdPlease SpecifyStep 3.Absconsion / MissingAttempted SuicideBanging Self Against Walls/Furniture/SurfacesHitting Body/Slap/Punch Self incl. Scratching & PickingInappropriate EatingInappropriate TouchingSelf-HarmStripping Clothes in Public AreaSuicideThrowing objectsOtherAggressive towards inanimate objectDiscrimination/Prejudice/RacialIntimidation / ThreatNeglectNon-Compliant / Obstructive / RudeDirect Physical AssaultPhysical HarassmentSexual Assault / AbuseSexual HarassmentUnintentional Aggressive BehaviourBullyingVerbal Assault / AbuseVerbal HarassmentOtherUnknownPre Existing Medical ConditionInadequate supervision gen health / post opObstruction / protruding objectSurface contaminantsRough terrain / irregular surfaceInappropriate equipment useFailure / malfunction of equipmentHorseplayPhysical training / sportWeather ConditionInadequate Lighting / designOtherHuman Use / ErrorObstruction / Protruding ObjectPhysical Training / SportDefective EquipmentUnsafe / Inappropriate systemUnknownTaskLoadWorking EnvironmentIndividual CapabilityOtherLiquid / Food / SteamEquipment / UtensilsAtmosphere / EnvironmentDefective EquipmentHuman Use / ErrorUnknownUnsafe SystemExplosionExposureElectrical Wiring / installationPage 5 of 7
SECTION H CNTD: WHAT TYPE OF HAZARD DID THIS INCIDENT RELATE TO? (Tick one option from Steps 1, 2, & 3)Chemical HazardsStep 1.Step 2.Acid / AlkalineAgri ChemicalsGasOther ChemicalProductsParticulatesPetroleum / SyntheticOil Based ProductsSanitation / CleaningChemicalsToxic MetalsAnimal RemedyArsenicAsbestosBleachCadmiumCarbon DioxideCarbon MonoxideChemical FertilizerCrystalline SilicaDetergentDiesel / KeroseneDisinfectantDrain / Oven CleanerDrugsFungicideGlue / AdhesiveGreaseHerbicideHydrochloric AcidSECTION I: IMMEDIATE ACTIONS TAKENotherwise stated within the organization, this person is responsible for completing the NIRF.SurnameSECTION K: WITNESS DETAILS (Name, Contact No. etc.)Date notifiedCategory of personLack of SupervisionUnknownHuman / User ErrorUnsafe System(For entry on Incident Review screen on NIMS)SECTION J: REPORTED BY: person who discovers the incident and unlessFirst nameStep 3.InsecticideLeadMetallic DustMotor / Gear / Hydraulic OilNatural GasOrganic DustPaint / Paint ProductPetrolPolishRadonRodenticideSoapSodium HydroxideSolventsSpent / Used Oil ProductSulphuric AcidWrong PatientOtherE.g. Nurse, Catering Staff, CleanerLocal system referenceno.DateContact DetailsHC NIRF-01Page 6 of 7
SECTION L: TO BE COMPLETED BY LINE/DEPARTMENT MANAGERHas open disclosure happened? * (tick one only )Yes(For entry on Incident Review screen on NIMS)NoIf No, please specify*:CATEGORY 1 INCIDENTS ONLYSAO Name:SAO Email and Contact Details:Is there a requirement to report this incident to any externalregulators/agencies/insurers (other than the State Claims Agency)?YesDate notified to SAO:NoIf Yes: Name regulator(s)/agency(ies) reported/notified to:Date Notified:123Line/Department Manager name:Title:Date:SECTION M: TO BE COMPLETED BY QUALITY AND PATIENT SAFETY OFFICEIs this incident a Serious Reportable Event (SRE)? * (tick one only )QPS Advisor Name:Yes(For entry on Incident Review screen on NIMS)NoDate:*Mandatory FieldsHC NIRF-01Page 7 of 7
NATIONAL INCIDENT REPORT FORM (NIRF) NIRF -01 PERSON NIMS record Number: Page 1 of 7 Incident: An event or circumstance which could have, or did lead to unintended and / or unnecessary harm. Please complete this form to the best of your knowledge at the time of reporting the incident. SECTION A: GENERAL INCIDENT DETAILS. Date of incident