Transcription
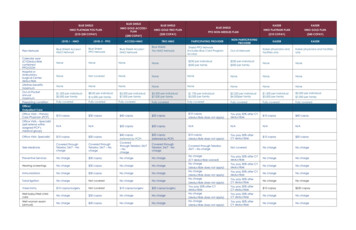
BLUE SHIELDBLUE SHIELDHMO PLATINUM POS PLAN( 10- 30 COPAY)LEVEL I - HMOLEVEL II - PPOHMO GOLD ACCESS PLANBLUE SHIELDHMO GOLD TRIO PLANPPO NON-NEEDLES PLAN( 20 COPAY)( 40 COPAY)ACCESS HMOTRIO HMOPARTICIPATING PROVIDERBlue ShieldTrio HMO NetworkShield PPO Network(includes Blue Card Programaccess)Plan NetworkBlue Shield Access HMO NetworkBlue ShieldPPO NetworkCalendar ospital orAmbulatorySurgical CenterdeductibleNoneNot coveredNoneNoneLifetime maximum 1,500 per individual 3,000 per family 8,00 per individual 16,000 per familyPreexisting conditionFully coveredFully coveredOffice Visits – PrimaryCare Physician (PCP) 10 copay 30 copay 40 copay 20 copayOffice Visits – Specialist(self-referral withinassigned PCP’smedical group)N/AN/A 50 copayOffice Visits -Specialist 10 copay 30 copayTele-MedicineCovered throughTeladoc 24/7 – NochargePreventive ServicesBlue Shield Access HMO NetworkBLUE SHIELDKAISERKAISERHMO PLATINUM PLANHMO GOLD PLAN( 10 COPAY)( 40 NetworkKaiser physicians andfacilities onlyKaiser physicians and facilitiesonly 250 per individual 500 per familyNoneNoneNoneNoneNoneNoneNoneNoneNoneNone 2,250 per individual 4,500per family 1,500 per individual 3,000 per family 3,500 per individual 7,000 per familyFully coveredFully coveredFully covered 10 copay(deductible does not apply)You pay 30% after CYdeductible 10 copay 40 copay 20 copayN/AN/AN/AN/A 40 copay(referred by PCP) 20 copay(referred by PCP) 10 copay(deductible does not apply)You pay 30% afterCY deductible 10 copay 50 copayCovered throughTeladoc 24/7 – NochargeCoveredthrough Teladoc 24/7– NochargeCovered throughTeladoc 24/7 - NochargeCovered through Teladoc24/7 – No chargeNot coveredNo chargeNo chargeNo charge 30 copayNo chargeNo chargeYou pay 30% after CYdeductibleNo chargeNo chargeHearing screeningsNo charge 30 copayNo chargeNo chargeYou pay 30% after CYdeductibleNo chargeNo chargeImmunizationsNo charge 30 copayNo chargeNo chargeYou pay 30% after CYdeductibleNo chargeNo chargeTubal ligationNo chargeNot coveredNo chargeNo chargeNo charge(CY deductible waived)No charge(deductible does not apply)No charge(deductible does not apply)No charge(deductible does not apply)You pay 30% afterCY deductibleNo chargeNo chargeVasectomy 10 copay/surgeryNot covered 10 copay/surgery 20 copay/surgeryYou pay 30% afterCY deductible 10 copay 250 copayWell baby/Well childcareNo charge 30 copayNo chargeNo chargeYou pay 30% afterCY deductibleNo chargeNo chargeWell woman exam(annual)No charge 30 copayNo chargeNo chargeYou pay 20% after CYdeductibleNo charge(deductible does not apply)No charge(deductible does not apply)You pay 30% afterCY deductibleNo chargeNo charge 3,500 per individual 7,000 per familyFully covered 3,500 per individual 7,000 per familyFully covered 250 per individual 500 per family 1,750 per individual 3,000 per familyFully coveredOffice/Outpatient Care
Emergency MedicalCareAmbulanceEmergency room(if admitted to theHospital, seeHospitalization Servicesfor cost share)Urgent careNo charge(for emergency orauthorized transport) 50 copay/visit (doesnot apply if admitted)No charge(for emergency orauthorized transport) 50 copay/visit(does not apply ifadmitted)No charge (foremergency orauthorized transport) 50 copay/visit (doesnot apply if admitted)No charge(foremergency or authorizedtransport) 50 copay/visit (does notapply if admitted)You pay 20% after CYDeductible (for emergency orauthorized transport) 50 copay/visit plus20% after CYdeductible; copaydoes not apply ifadmittedPhysician: 20% after CYdeductible 10 copay 10 copay 40 copay 20 copayYou pay 20% afterCY deductible (foremergency orauthorizedtransport) 50 copay/visitplus 20% afterCY deductible;copay doesnot apply ifadmittedNo charge whenmedically necessary 150 copay when medicallynecessary 50 copay (does notapply if admitted) 150 copay (does not apply ifadmitted)Physician: 20% afterCY deductible 10 copay (deductible doesnot apply)30% after CYdeductible 10 copay 40 copayYou pay 20% after CYdeductibleYou pay 30% afterCY deductibleNo charge 10 copay.Diagnostic ServicesLaboratory andPathology TestsDiagnostic Tests and XRayNo chargeNo chargeCovered only whenperformed inphysician’s officeNo chargeNot covered for CT,MRI, MUGA, PET, andSPECTOutpatientdepartment ofHospital – No chargeOther – You pay 40%Outpatient departmentof Hospital – No chargeOther – You pay 40%Outpatientdepartment ofHospital – No chargeOther – You pay 40%Outpatient departmentof Hospital – No chargeOther – You pay 40%You pay 20% after CYdeductibleYou pay 30% afterCY deductibleNo charge 10 copayMRI, most CT and PET: 100copaySee “Prescription Drugs”See “Prescription Drugs”See “PrescriptionDrugs”See “PrescriptionDrugs”See “Prescription Drugs”Diabetes CareCovered Diabeticdrugs and testingsuppliesSee “PrescriptionDrugs”See “PrescriptionDrugs”No charge 30 copayOffice Visit: 40copayOffice Visit: 20 copay 10 copay (deductible doesnot apply)You pay 30% afterCY deductibleNo chargeNo chargeNo chargeNot coveredYou pay 40%You pay 40%You pay 20% after CYdeductibleYou pay 30% afterCY deductibleSee Durable MedicalEquipmentSee Durable MedicalEquipmentPrenatal andPostnatal officevisitsNo chargeYou pay 20%coinsuranceNo chargeNo charge 10 copay after CYdeductibleYou pay 30% afterCY deductibleNo chargeNo chargeDelivery (ProfessionalServices)No chargeNot coveredNo chargeNo chargeYou pay 20% after CYdeductibleYou pay 30% afterCY deductibleNo chargeNo chargeNewborn CareNewborncovered 30days; must enrollthrough theTeamsters 1932Health TrustCovered underHMO, Level I BenefitNo charge. Newborncovered 30 days;must enroll throughthe Teamsters 1932Health Trust within 60days of birthNo charge. Newborncovered 30 days; mustenroll through theTeamsters 1932 HealthTrust within 60 days ofbirthNewborn covered 30days; must enroll throughthe Teamsters 1932 Trustwithin 60 days of birthNewborn covered30 days; must enrollthrough theTeamsters 1932 Trustwithin 60 days ofbirthNewborn covered30 days; mustenroll through theCounty within 60days of birthNewborncovered 30days; mustenroll throughthe Countywithin 60 daysDiabetes SelfManagementTraining &EducationDevices, Equipment,and Non-TestingSuppliesSee “PrescriptionDrugs”Maternity Care
within 60 days ofbirthof birthHospital ServicesHospital care(Hospital and Physiciancharges)No chargeNot coveredHospital: 100/admission plus20%Physician: No chargeHospital: 100/admissionplus 20%Physician: No chargeYou pay 20% after CYdeductibleYou pay 30% afterCY deductibleNo charge 500copay per dayNo charge(Facility andPhysician)Facility: 500 copay per dayFacility: 10 copayper procedureFacility: 250 copay perprocedurePhysician: You pay30% after CYdeductiblePhysician: No chargePhysician: No chargeNot coveredNo charge upto 100 visitsperaccumulationperiodNo charge up to 100 visits peraccumulation periodNot coveredNo chargeNo chargeYou pay 20% afterCY deductible up100 days per Benefitperiod - combinedPPO/Non-PPOmaximumNo charge up to100 days perbenefit periodNo charge up to 100 daysper benefit periodSurgical ServicesHospital – In-PatientSurgical ServicesOutpatient /Ambulatory SurgeryCenterNo charge(Facility andPhysician)No charge(Facility andPhysician)Not coveredNot coveredFacility: 100admission plus 20%Physician: No chargeFacility: You pay 40%Physician: NochargeFacility: 100 admissionplus 20%Physician: No chargeFacility: You pay 40%Physician: No chargeFacility: You pay 20% after CYdeductiblePhysician: You pay 20% afterCY deductibleFacility: You pay 20% after CYdeductiblePhysician: You pay 20% afterCY deductibleFacility: You pay 30%after CY deductiblePhysician: You pay30% after CYdeductibleFacility: You pay 30%after CY deductiblePhysician: No chargeAlternatives toHospital CareHome health servicesHospiceSkilled nursing facilities(SNF)Mental Health Careand Substance AbuseTreatmentOutpatient servicesInpatient servicesNo charge upto 100 visitsper calendaryearNo charge;includes routinehome care, 24-hourcontinuous homecare, short-term IPcare for pain/symptommanagementNo chargeMHSAParticipating Provider 10 copayNo chargeNot coveredNo charge up to 100visits per calendaryearNo charge up to 100visits per calendar yearNot coveredNo charge; includesroutine home care,24- hour continuoushome care, shortterm IP care forpain/symptommanagementNo charge; includesroutine home care, 24hour continuous homecare, short-term IP carefor pain/symptommanagementNot coveredMHSANon-ParticipatingProviderNo charge up to 100days per BenefitPeriodNo charge up to 100days per Benefit PeriodYou pay 20% after CYdeductible up to 100 visits percalendar yearNo charge (deductible doesnot apply)24-hr continuous homecare/Short-term inpatient carefor pain and symptom mgmt.:You pay 20% after CYdeductibleYou pay 20% after CYdeductible up 100 days perBenefit period - combinedPPO/Non-PPO maximumMHSAParticipating ProviderHospital based SNF:You pay 30% after cipating ProviderMHSAParticipating Provider 10 copay 40 copayAll other services areno charge 20 copayAll other services are nochargeOutpatient: 10 copay(deductible does not apply)All other services: You pay20% after CY deductibleYou pay 30% after CYdeductibleNot coveredPhysician: No chargeHospital services andresidential care: 100/ admission plusPhysician: No chargeHospital services andresidential care: 100/admission plus 20%You pay 20% after CYdeductibleYou pay 30% after CYdeductible 10 copay perindividual 5 copay per groupNo charge 40 copay individual; 20 copay groupSubstance abuse: 5 copaygroup 500 copay per day
20%Prescription DrugsPrescription drugs (perfill)Includes Diabeticdrugs and testingsuppliesRetail Pharmacy (30day supply):Tier 1- 5 copayTier 2 - 10 copayTier 3 - 25 copayTier 4 - 10 copay(excluding specialtydrugs)Not coveredRetail Pharmacy (30day supply):Tier 1- 5 copayTier 2 - 10 copayTier 3 - 25 copayTier 4 – 20% up to 200/Rx (excludingspecialty drugs)Retail Pharmacy (30-daysupply):Tier 1- 5 copayTier 2 - 10 copayTier 3 - 25 copayTier 4 – 20% up to 200/Rx(excluding specialtydrugs)Specialty Pharmacy:Tier 4 - 10 copay(Specialty Drugs 30day supply)Specialty Pharmacy:Tier 4 – 20% up to 200/Rx (SpecialtyDrugs 30- day supply)Specialty Pharmacy:Tier 4 – 20% up to 200/Rx(Specialty Drugs 30- daysupply)Mail order(90-day supply):Tier 1- 10 copayTier 2 - 20 copayTier 3 - 50 copayTier 4 - 20 copay(excluding specialtydrugs)Mail order(90-day supply):Tier 1- 10 copayTier 2 - 20 copayTier 3 - 50 copayTier 4 – 20% up to 400/Rx (excludingspecialty drugs)Mail order(90-day supply):Tier 1- 10 copayTier 2 - 20 copayTier 3 - 50 copayTier 4 – 20% up to 400/Rx (excludingspecialty drugs)Pharmacy (retail andmail order) copaysdo not apply towardthe out-of- pocketmaximum.PARTICIPATING PHARMACYRetail Pharmacy (30-daysupply):Tier 1- 15 copayTier 2 - 30 copayTier 3 - 30 copayTier 4 - 15 copay (excludingspecialty drugs)Specialty Pharmacy:Tier 4 - 15 copay (SpecialtyDrugs 30- day supply)Mail order(90-day supply):Tier 1- 30 copayTier 2 - 60 copayTier 3 - 60 copayTier 4 - 30 copay (excludingspecialty drugs)Pharmacy (retail and mailorder) copays do not applytoward the out-of- pocketmaximumNONPARTICIPATINGPHARMACYRetail Pharmacy (30day supply):(Member pays 25% ofbilled amount pluscopay)Tier 1- 15 copayTier 2 - 30 copayTier 3 - 30 copayTier 4 - 15 copay(excluding specialtydrugs)Pharmacy (up to a100-day supply):Generic – 10 copayBrand – 15 copayMost specialty items 15 copay (up to a30-day supply)Mail order (up to a100-day supply):Generic – 10 copayBrand – 15 copayPharmacy (up to a 30-daysupply): Generic – 15 copayBrand – 35 copayMost specialty items: 30%, notto exceed 200 (up to a 30day supply)Mail order (up to 100-daysupply):Generic – 30 copayBrand – 70 copaySpecialty Pharmacy:Not coveredMail order:Not coveredPharmacy (retail andmail order) copaysdo not applytoward the out-ofpocket maximumOther ServicesAllergy testingChiropractic careDurable medicalequipment (DME)Breast PumpOrthoticEquipment/devicesProsthetic EquipmentPhysical andOccupational Therapy 10 copayAllergy Serum: NochargeNot covered Discountprogram available 30 copayAllergy Serum: NochargeNot coveredDiscount programavailableNo chargeNot coveredOffice Location: 10copayOffice Location: 30copay (up to 12 visitsper calendar yearOutpatient Dept. of aHospital: No chargeOutpatient Dept. of 40 copayAllergy Serum: Youpay 40% copayNot coveredDiscount programavailable 20 copayAllergy Serum: You pay40% copayYou pay20%(deductibledoes notapply)Allergy Serum: 20%after CY deductibleYou pay 30% after CYdeductibleNot coveredDiscount programavailable20% after CY deductible upto 30 visits per calendar yearcombined PPO/Non-PPOmaximum30% after CYdeductible up to 30visits per calendaryear combinedPPO/Non-PPOmaximumDME: You pay 40%No chargeNo chargeNo chargeDME: You pay 40%No chargeNo chargeNo charge 40 copay 20 copayYou pay 20% after CYdeductibleBreast Pump: No chargeYou pay 20% (deductibledoes not apply)You pay 30% after CYdeductibleBreast Pump: NotcoveredYou pay 30% after CYdeductibleAllergy serum: 10copayNot coveredAllergy serum: 5 copayNot coveredNo chargeYou pay 50% 10 copay 40 copay
a Hospital: NotcoveredOffice Location: 10copaySpeech TherapyVision (exam only)Outpatient Dept. of aHospital: No charge 10 copay(one exam in aconsecutive 12month periodprovided throughcontracted VPA)Office Location: 30copayOutpatient Dept. ofa Hospital: Notcovered 0 up to 60/yearplus 100% ofadditional charges(one exam in aconsecutive 12month periodprovided throughcontracted VPA) 40 copay(Not covered) 20 copay(Not covered)You pay 20% (deductibledoes not apply)You pay 20% self-referredexam per 12 consecutivemonths, no age limit (Visionplan administrator’s providersonly)You pay 30% after CYdeductible 10 copay 40 copayYou pay 20% selfreferred exam per 12consecutive months,no age limit (Visionplan administrator’sproviders only)No chargeNo chargeKaiser facilities in theUS.Claim formsrequired for Out ofArea Urgent andER careKaiser facilities in the US.Claimformsrequiredfor Out ofAreaUrgentand ERcareTravelNetwork(For urgent careservices)Inside of US: BlueCard ProgramOutside of US: BlueShield Global CoreProgramRefer to your EOCInside of US: BlueCard ProgramOutside of US: BlueShield Global CoreProgramRefer to your EOCInside of US: BlueCard ProgramOutside of US: BlueShield Global CoreProgramRefer to yourEOCImmunizations forpurposes of ForeignTravel 10 copay/injection 30 copay/injection 10 copay/injectionInside of US: Blue CardProgram Outside of US:Blue Shield Global CoreProgramRefertoyourEOCInside of US: Blue CardProgram Outside of US: BlueShield Global Core ProgramRefer to your EOCInside of US: BlueCard ProgramOutside of US: BlueShield Global CoreProgramRefer toyour EOC 10 copay/injectionYou pay 20% after CYdeductibleYou pay 30% after CYdeductibleNo chargeNo chargeprovider.bcbs.combcbsglobalcore.comkp.org (search for“Travel Health”)kp.org (search for .comAdditional ore.comNote! This is a Brief Comparison. Please refer to the Healthplan's Evidence of Coverage or Summary of Benefits for a detailed description of coverage, limitations and exclusions.
KAISER HMO GOLD PLAN ( 40 COPAY) LEVEL I - HMO LEVEL II - PPO ACCESS HMO TRIO HMO PARTICIPATING PROVIDER . Vasectomy 10 copay/surgery Not covered 10 copay/surgery 20 copay/surgery You pay 20% after CY . for cost share) 50 copay/visit (does not apply if admitted) admi 50 copay/visit copay (does not apply if