Transcription
CLASSIFIED d.usP (714) 558-5686F (714) 558-56821601 E Chestnut AveSanta Ana, CA 92701
0102-03Plan ChangesWho Is EligibleOpen EnrollmentMedical HMO Planswith MedicareWho You Cannot CoverRetiree AgreementPlan Comparison ChartWhen Coverage BeginsMedicareFocus on BenefitsWho You Can Cover04Rules for ChangesWhen You Can Enroll05Tools and Resources06TelephoneAppointmentsHeal Teladoc KP4CARE0708Plan Comparison ChartPlan Comparison ChartPrescriptionCoverage with HMOPlans with MedicareMedical HMO Planswith or withoutMedicare1213Plan Comparison ChartPlan Comparison ChartDental PPO PlansDental HMO Plan09PrescriptionCoverage with HMOPlans with orwithout Medicare10Medical PPO Planwith or withoutMedicarePlan Comparison Chart11PrescriptionCoverage with PPOPlans with orwithout MedicarePlan Comparison ChartPlan Comparison ChartPrior AuthorizationPrior AuthorizationStep TherapyStep TherapyDrug Quantity ManagementDrug Quantity Management14Vision15Employee AssistanceProgramsBlue Shield Life Referrals16-17RatesMedicalDentalKaiser Behavioral Health18Key TermsMedical/GeneralPrescriptionDental19Plan Notices andDocumentsBackProvider DirectoryCONTENTSFor your convenience, we’ve provided this table ofcontents for two purposes:It provides you an overview of the document’s contentsand organization and,It allows readers to go directly to a specific section of theonline document.
*While we have made every effort to make sure that this guide iscomprehensive, it cannot provide a complete description of all benefitprovisions. For detailed information, you should refer to your planbenefit booklets provided by your insurance provider or summary plandescriptions that are on our website www.sausd.us/benefits. The planbenefits booklets provided by your insurance provider determine howall benefits are paid.The benefits explained in this summary areeffective July 01, 2019 through June 30, 2020.
Plan ChangesHere are some medical and dental plan highlights for the 20192020 school year.MedicalKaiser Senior Advantage HMORate increase*No changes to medical coverageKaiser Permanente HMORate increase*No changes to medical coverageMembers still receive vision coverage through VSPBlue Shield 65 Plus HMORate increase*No changes to medical coverageBlue Shield Trio ACO HMONow the lowest costing HMO plan*No changes to medical coverageMembers still receive pharmacy coverage through Express ScriptsMembers still receive vision coverage through VSPBlue Shield Access HMORate increase*No changes to medical coverageMembers still receive pharmacy coverage through Express ScriptsMembers still receive vision coverage through VSP01Here at Santa Ana Unified webelieve that you are our mostimportant asset. Helping you andyour families achieve andmaintain good health - physical,emotional, and financial - is thereason we offer you this program.This year, we are pleased toannounce no changes to our plancoverages and minimal increasesto plan cost.However, even though our planare not changing significantly,you may have different needsthan last year.Open Enrollment is your once-ayear opportunity to review yourexisting elections and make anychanges to your plans, add ordrop dependents, or enroll in theFlexible Spending Account withAmerican Fidelity for the 20192020 school year.Blue Shield Spectrum PPORate increase*No changes to medical coverageMembers still receive pharmacy coverage through Express ScriptsMembers still receive vision coverage through VSP*Refer to your Rates on page 13DentalDelta Care USA DHMONo rate increase and no changes to dental coverageDelta Dental Incentive DPPONo rate increase and no changes to dental coverageDelta Dental Network DPPONo rate increase and no changes to dental coverageFOCUS ONBENEFITS
02Who You Can CoverYou may enroll the following family members in our health insurance plans.WHO ISELIGIBILEYour SpouseThe person you are legally married to under state law, including a same-sexspouse.Your Domestic PartnerOnly with proof of a Declaration of Domestic Partnership filed with the CaliforniaState Secretary. California state registration is limited to same sex domesticpartners where one is at least 62 and eligible for Social Security based on their age.Any premiums paid for by SAUSD for your domestic partner are taxable and will beincluded in your W-2. Any premiums you pay for your domestic partner will bededucted on an after-tax basis.Your ChildrenIncluding your Domestic Partner’s children, adopted children, and/or stepchildren.Your children must be under 26 years old. They do not have to live with you or beenrolled in school. They can be married and living on their own.Any child over the age of 26 only if they are mentally or physically handicapped.Any children that are named in a Qualified Medical Child Support Order (QMCSO)as defined by federal law.Who You Cannot CoverYou may not enroll the following family members in our health insurance plans.Family members who are not eligible for coverage include, but are not limited to:Your ParentsYour GrandparentsYour Siblings
When Coverage BeginsAny changes you make during Open Enrollment begin July 1.All other changes will go in to effect the first day of the following month you notify our office.If you add a child, their coverage will being the first day of the following month except for newborn children. Newbornchildren will be added effective their date of birth.When You Can EnrollOpen EnrollmentOpen enrollment is usually held in late April or early May and is the one time each year you can make changes to yourbenefits without a qualifying event.Qualifying EventsMake sure to notify our office right away if you have a qualifying event and need to make a change to your coverage.These events include, but are not limited to, the birth or adoption of a baby or child, loss of other coverage, youreligibility for new coverage, a marriage, or a divorce. You have 30-days to make your changes.
Rules for ChangesOther than open enrollment, you can only make changes to your benefits if you have a qualified event or a “ specialenrollment”. If you have a qualified event and are able to make changes to your benefits, you will be required tosubmit proof of that change or evidence of prior coverage.There are four basic types of qualifying events. The following are examples, not a full list:Loss of Health CoverageIf you lose your current coverage, including job-based,individual, and/or a student planIf you are no longer eligible for Medicare, Medicaid, orCHIPChanges in HouseholdLike getting married or a divorceHaving a baby or adoption a childWhen you turn 26 years and loseyour coverage through yourparent’s planExperiencing a death in your familyOther Qualifying EventsChanges in ResidenceIf you move to different ZIP codeor county that affects your accessto network providersChanges in your income that affectthe coverage you qualify forA change in eligibility for Medicare or MedicaidA court order including a Qualified Medical ChildSupport Order (QMCSO)Two rules apply to making changes to your benefits during the year:1. Any change you make must be consistent with the change in status, AND2. You must notify our office and make the change before or within 30-days of the date the event occursYou are responsible for notifying our office of your dependent(s) that become INELIGIBLE because of a divorce orbecoming an overage dependent before or within 30-days of the event. Failure to do so may jeopardize yourdependent’s right to COBRA.04
Tools and ResourcesBefore you make any decision about your coverage, there is some important information you need to know about yourbenefits. Below is a list of tools and resources that will give you the information you need to make informed decisionsduring this plan year.MedicareOpen Enrollment AnnouncementThis announcement includes information that retireesneed to consider when selecting their benefits for2019-2020 plan year.Retiree AgreementThe Retiree Agreement you signed when you retiredgives you an overview of the benefits you are eligiblefor and how long.You and/or your spouse must enroll into Medicareparts A and B once you and/or your spouse becomeeligible for Medicare.Medicare becomes your primary insurance and theDistrict coverage becomes your secondary coverage.Make sure to tell your doctor’s office that Medicare Iyour primary insurance.When you visit your doctor’s office, tell the Medicare isyour primary insurance, give them your Medicare card,and your provider I.D. card; the doctor’s office shouldtake care of the rest.Telephone AppointmentsAvailable to all Blue Shield members, Heal and Teladoc let you see a doctorat a time and place that is best for you.Heal is only available for Blue Shield PPO members in Los Angeles, OrangeCounty, San Francisco, Oakland, Berkeley, San Diego, and the Peninsula to SanJose.The cost for Heal is the same as your plan’s co-pay and Teladoc has a 5co-pay for both HMO and PPO members.Heal Teladoc 8 a.m. to 8 p.m. dailyPhone: 1-844-644-4325getheal.comPhone: 1-800-835-2362teladoc.com/bscSmartphone app also availableKaiser members can get care from a doctor wherever they are. If you have aminor health condition or need a follow-up, you may be able to talk to a doctorby video or phone.You need an in-person appointment and need to register on kp.org before youcan receive a video or phone appointment.Monday - Friday7 a.m. to 7 p.m.Phone: 1-800-954-800005
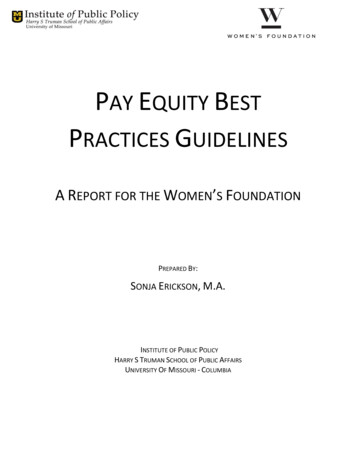
-Medical HMO Plans with MedicareMedical coverage provides you with benefits that keep you healthy like preventative care screenings and accessto urgent care. It also provides important financial protection if you have a serious medical condition. Thefollowing chart shows two plans available to self-pay subscribers who have Medicare Parts A and B.Kaiser SeniorAdvantage HMOBlue Shield65 Plus HMO 190.70 292.98 381.40 581.45NoneNone 1,500 per Individual 3,000 per Family 6,700 per IndividualUnlimitedUnlimitedPrimary Provider 20 Co-pay 20 Co-paySpecialist Office Visit 20 Co-pay 20 Co-payPlan Pays 100%Plan Pays 100% 20 Co-pay 20 Co-paySingle(Subscriber Only)2 Party(Subscriber 1)Annual DeductibleAnnual Out-of-PocketMaxLifetime MaxOffice VisitsPreventive ServicesChiropractic CareMedicare Covered 15 Co-payAmerican Specialty Health Covered(Limit of 20 visits per year)Labs and X-RaysPlan Pays 100% 20 Co-payInpatientHospitalization 250 Co-pay 250 Co-payOutpatient Surgery 20 Co-payPlan pays 100%Urgent Care 20 Co-pay 25 Co-payEmergency Room 50 Co-pay 50 Co-payHospitalizationPer admissionPer admissionEmergency Services06Waived if admittedWaived if admitted
If you enroll in medical coverage, you will receive coverage for prescription drugs. The following chart showsthe prescription coverage offered to self-pay subscribers who are with Medicare and enrolled in our withMedicare medical HMO plan.Blue Shield65 Plus HMONoneNone 1,500 per Individual 3,000 per FamilyN/AGeneric 10 Co-pay 10 Co-payPreferred Brand-Name 20 Co-pay 20 Co-payN/A 40 Co-pay30 Days30 DaysGeneric 20 Co-pay 20 Co-payPreferred Brand-Name 40 Co-pay 40 Co-payN/A 80 Co-pay100 Days90 daysPrescription DrugDeductibleAnnual Out-of-PocketLimitCombined with MedicalPharmacy Co-paysNon-PreferredBrand-NameSupply LimitMail Order Co-paysNon-PreferredBrand-NameSupply LimitRx Coverage with HMO Plans with MedicareKaiser SeniorAdvantage HMO07
Medical HMO Plans with or without MedicareMedical coverage provides you with benefits that keep you healthy like preventative care screenings and accessto urgent care. It also provides important financial protection if you have a serious medical condition. Thefollowing chart shows the medical HMO plans available to self-pay subscribers who are with or without Medicare.Blue ShieldTrio A.C.O. HMOSingleBlue ShieldAccess HMOKaiser PermanenteHMOw/o Medicarew/ Medicarew/o Medicarew/ Medicare 514.14 457.12 661.10 582.02 678.22 1,062.25 943.95 1,356.29 1,203.11 1,351.74 1,597.83 1,360.91 1,953.81 1,733.53 1,917.40(Subscriber Only)2 Party(Subscriber 1)Family(Subscriber 2 or more)Refer to the Rates page to view 1 with 1 without Medicare ratesAnnual DeductibleAnnual Out-of-PocketMaxLifetime MaxNoneNoneNone 1,000 per Individual 3,000 per Family 1,000 per Individual 2,000 per Family 1,500 per Individual 3,000 per FamilyUnlimitedUnlimitedUnlimited 20 Co-pay 20 Co-pay 20 Co-pay 20 Co-pay 20 Co-payOffice VisitsPrimary ProviderSpecialist Office Visit 20 Co-payWhen you are referred by your primarycare physician 20 Co-payPreventive ServicesChiropractic CareWhen you are referred by your primarycare physician 30 Co-payWhen you self-refer office visits andconsultations within your Trio providergroupWhen you self-refer office visits andconsultations within your Access provider groupPlan Pays 100%Plan Pays 100%Plan Pays 100%Up to 30 visits per yearUp to 30 visits per year 10 Co-payNot CoveredPlan Pays 100%Plan Pays 100%Plan Pays 100% 250 Co-pay 250 Co-pay 250 Co-payPlan pays 100%Plan pays 100% 20 Co-payUrgent Care 20 Co-pay 20 Co-pay 20 Co-payEmergency Room 100 Co-pay 100 Co-pay 100 Co-payLabs and X-Rays 10 Co-payHospitalizationInpatientOutpatient SurgeryPer admissionPer admissionPer admissionEmergency Services08Waived if admittedWaived if admittedWaived if admitted
If you enroll in medical coverage, you will receive coverage for prescription drugs. The following chart showsthe prescription coverage offered to self-pay subscribers who are with or without Medicare and enrolled in oneof our medical HMO plans.Blue ShieldAccess HMOKaiser PermanenteHMOExpress Scripts1Express Scripts1Kaiser Pharmacy 150 per Individual 150 per IndividualNone 5,600 per Individual 10,200 per Family 5,600 per Individual 10,200 per FamilyCombined with MedicalGeneric 10 Co-pay 10 Co-pay 10 Co-payPreferred Brand-Name 25 Co-Pay* 25 Co-Pay* 20 Co-payNon-PreferredBrand-Name 40 Co-Pay* 40 Co-Pay*N/A30 Days30 Days30 DaysGeneric 20 Co-pay 20 Co-pay 20 Co-payPreferred Brand-Name 50 Co-pay* 50 Co-pay* 40 Co-payNon-PreferredBrand-Name 80 Co-pay* 80 Co-pay*N/A90 Days90 Days100 DaysPrescription DrugDeductibleAnnual Out-of-PocketLimitFor a brand-name RxFor a brand-name RxPharmacy Co-PaysSupply LimitMail Order CopaysSupply Limit*After Deductible1Express Scripts Advantage Plus Utilization Management ProgramThis Express Scripts program uses strategies to help manage the high-cost and high-utilization of specialty andnon-specialty medications.Subscribers may be required to participate in the following programs when filling their prescriptions:Drug Quantity ManagementStep-TherapyPrior AuthorizationDrug quantity management isrequired for medicationsprescribed, “as needed” for whichthe days of supply cannot beinferred from the prescription(migraine medication, inhalers,creams, ointments).Step-therapy is required for mostnon-specialty drugs, includingtherapies for diabetes, high bloodpressure, depression, and ulcers.Prior authorization is required formost specialty drugs.Rx Coverage with HMO Plans with or without MedicareBlue ShieldTrio A.C.O. HMO09
Medical PPO Plan with or without MedicareMedical coverage provides you with benefits that keep you healthy like preventative care screenings and accessto urgent care. It also provides important financial protection if you have a serious medical condition. Thefollowing chart shows the medical PPO plan available to self-pay subscribers who are with or without Medicare.Blue ShieldSpectrum PPOSinglew/o Medicarew/ Medicare 987.38 869.87 2,051.33 1,806.64 2,945.72 2,594.82(Subscriber Only)2 Party(Subscriber 1)Family(Subscriber 2 or more)Refer to the Rates page to view 1 with 1 withoutMedicare ratesIn-NetworkOut-of-Network 300 per Individual 600 per Family 600 per Individual 1,200 per Family 1,300 per Individual 2,600 per Family 2,600 per Individual 5,200 per FamilyUnlimitedUnlimitedPrimary Provider 20 Co-payPlan pays 70%*Specialist Office Visit 20 Co-payPlan pays 70%*Preventive ServicesPlan Pays 100%Plan pays 70%*Chiropractic CarePlan pays 80%*Plan pays 70%*Labs and X-RaysPlan pays 80%*Plan pays 70%*InpatientPlan pays 90%*Plan pays 70%*Outpatient SurgeryPlan pays 90%*Plan pays 70%* 20 Co-payPlan pays 70%* 150 Co-pay 10% 100 Co-pay 10%Annual DeductibleAnnual Out-of-PocketMaxLifetime MaxOffice VisitsUp to 50 visits per yearUp to 50 visits per yearHospitalizationUp to 1,500 per dayUp to 1,500 per dayEmergency ServicesUrgent CareEmergency RoomWaived if admittedWaived if admitted*After Deductible10
If you enroll in medical coverage, you will receive coverage for prescription drugs. The following chart showsthe prescription coverage offered to self-pay subscribers who are with or without Medicare and enrolled in ourmedical PPO plan.Express Scripts1Prescription DrugDeductibleAnnual Out-of-PocketLimitIn-NetworkOut-of-Network 150 per Individual 150 per Individual 5,300 per Individual 10,600 per Family 4,000 per Individual 8,000 per FamilyFor a brand-name RxFor a brand-name RxPharmacy Co-PaysGeneric 10 Co-payPreferred Brand-Name 25 Co-Pay* 25 Co-Pay*Non-PreferredBrand-Name 40 Co-Pay* 40 Co-Pay*30 Days30 DaysGeneric 20 Co-payNot CoveredPreferred Brand-Name 50 Co-pay*Not CoveredNon-PreferredBrand-Name 80 Co-pay*Not Covered90 DaysNot ApplicableSupply Limit 10 Co-payThen plan pays 75%Mail Order CopaysSupply Limit*After Deductible1Express Scripts Advantage Plus Utilization Management ProgramThis Express Scripts program uses strategies to help manage the high-cost and high-utilization of specialty andnon-specialty medications.Subscribers may be required to participate in the following programs when filling their prescriptions:Drug Quantity ManagementStep-TherapyPrior AuthorizationDrug quantity management isrequired for medicationsprescribed, “as needed” for whichthe days of supply cannot beinferred from the prescription(migraine medication, inhalers,creams, ointments).Step-therapy is required for mostnon-specialty drugs, includingtherapies for diabetes, high bloodpressure, depression, and ulcers.Prior authorization is required formost specialty drugs.Rx Coverage with PPO Plan with or without MedicareBlue ShieldSpectrum PPO11
Dental PPO PlansSAUSD gives you a choice of two dental DPPO plans. When you enroll in a Delta Dental DPPO plan, you have thechoice of visiting any dentist you chose, including in-network providers, non-network premier providers, and outof-network providers. Members receive the highest level of benefits when they visit a preferred provider.Contact Delta Dental at 1-866-499-3001 or visit their website at www.deltadentalins.com to find a provider nearyou.Delta DentalNetwork DPPODelta DentalIncentive DPPO 45.81 57.27 127.35 159.19 173.20 216.54Single(Subscriber Only)2 Party(Subscriber 1)Family(Subscriber 2 or more)Annual DeductiblePreferred ProviderPremier ProviderPreferred ProviderPremier ProviderNoneNoneNone 25 per Individual 75 per FamilyWaived for diagnostic andpreventative services 2,000 perIndividual 1,200 perIndividual 2,000 perIndividual 1,500 perIndividualWaiting PeriodNoneNoneNoneNoneDiagnostic andPreventativePlan pays 100%Plan pays 50%Plan Pays 70-100%Plan Pays 70-100%FillingsPlan pays 100%Plan pays 50%Plan pays 70-100%Plan pays 70-100%Root CanalsPlan pays 100%Plan pays 50%Plan pays 70-100%Plan pays 70-100%Diagnostic andPreventativePlan pays 100%Plan pays 50%Plan pays 70-100%Plan pays 70-100%ProsthodonticsPlan pays 50%Plan pays 50%Plan pays 50%Plan pays 50%Other MajorServicesPlan pays 100%Plan pays 50%Plan pays 70-100%Plan pays 70-100%OrthodontiaPlan pays 50%Plan pays 50%Plan pays 50%Plan pays 50%Lifetime Max 1,000 1,000 500 500DependentsCoveredCoveredCoveredCoveredAnnual Plan MaxBasic ServicesAfter deductibleAfter deductibleAfter deductibleMajor ServicesAfter deductibleAfter deductibleOrthodontia ServicesThe Incentive plan pays 70% for diagnostics,preventative, basic and major services for thefirst year. This percentage increases by 10%each year to a max of 100% as long as you usethe coverage at least once a year. If you donot use the plan at least once during the year,your percentage will remain at the levelattained the previous year.12
Delta Care is a dental DHMO plan and automatically assigns you and your dependents a dentist when you enroll.You can always change your dentist by contacting Delta Care and letting them know the office you prefer withinthe Delta Care network.Delta Care USA D.H.M.O.Single 16.76(Subscriber Only)2 Party 27.66(Subscriber 1)Family 40.88(Subscriber 2 or more)Annual DeductibleAnnual Plan MaxWaiting PeriodDiagnostic and Preventative*NoneUnlimitedNone 0- 45 Co-pay then the plan pays 100%Dental HMO PlanVisit www.deltadentalins.com to find a provider near you.Basic ServicesFillings*Plan pays 100%Root Canals*Plan pays 100%Diagnostic and Preventative*Plan pays 100%Major ServicesProsthodonticsOther Major Services*N/A 0- 195 Co-pay than the plan pays 100%Orthodontia ServicesOrthodontia* 1,700- 1,900 Co-payLifetime MaxUnlimitedDependentsCovered*Co-pays vary by the type of services you receive. Toreceive a list of Delta Care’s fee schedule, you shouldcontact Delta Care at 1-800-422-4234 and request a copyof the plan’s contract.13
14V.S.P.In-Network CoverageOut-of-Network Coverage 15 Co-payPlan pays up to 45Event 12 monthsEvery 12 monthsSingleVision LensPlan pays 100% of basic lensPlan pays up to 30Bifocal LensPlan pays 100% of basic lensPlan pays up to 50TrifocalLensPlan pays 100% of basic lensPlan pays up to 65Every 12 monthsEvery 12 monthsPlan pays up to 130Plan pays up to 70Office VisitThen the plan pays 100%FrequencyEyeglass LensesVisionCoverageFrequencyFramesBenefitRoutine vision exams areimportant, not only for correctingvision but because they can detectother serious health conditions.All SAUSD subscribers and familymembers enrolled in our medicalplans will receive vision benefitsfrom VSP.On select framesPlan pays up to 150On featured framesFrequencyEvery 24 monthsEvery 24 monthsPlan pays up to 130Plan pays up to 105Every 12 monthsEvery 12 monthsContactsBenefitFrequencyWith up to 60 co-pay for fitting and evaluationVisit vsp.com to find a V.S.P. provider near you.
Blue Shield Life Referrals 24/7Because we want our employees to have a well-balanced life, Blue Shieldmembers will receive EAP benefits through Blue Shield’s Life Referral 24/7program.This program provides referrals to professional counselors for up to three freeface-to-face confidential visits every6-months and live 60-minute telephone consultations.You can access this program 24 hours, 365 days to help you resolve emotional,health, family, and work issues.This benefit is included in your Blue Shield medical plan and is available to allhousehold members.Life Referrals 24/71-800-985-2405Kaiser Behavioral HealthKaiser takes care of the whole you. Your personal physician coordinates your carewith a mental health specialist, or team, that can diagnose mental health issuesthat affect your health and well-being.Depending on your needs, you can choose from a wide range of services; call oremail your doctor, make non-urgent appointments online, call to make anappointment for therapy and other counseling services, talk to an advice nurse,speak with a wellness coach or enroll to take a class.Behavioral Health Hotline1-800-900-3277Wellness (EAP)It is the District’s goal to offersubscribers and their familiesprograms, resources and activities tosupport and encourage healthylifestyles. These resources includerelational, nutritional, physical, andemotional wellbeing.
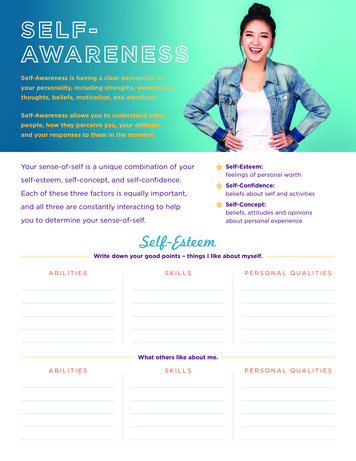
Medical16Kaiser Sr.AdvantageYou PayKaiser HMOYou PayRatesBlue Shield65 PlusRates are effectiveJuly 01, 2019throughJune 30, 2020Subscribers are billed a month inadvance, on the third Monday everymonth, and their payments are due onthe second Friday of the following month.2 PartyBlue ShieldTrio A.C.O.You Pay1 w/ 1 w/o Medicare 190.70 381.40 755.68Single2 PartySubscriber 1Subscriber 2 or more 565.18 1,126.45 1,597.83Subscriber OnlySingle2 Party2 Party2 with Medicare1 w/ 1 w/o Medicare 292.98 581.45 807.12 954.08Without MedicareYou Pay2 PartySubscriber 1Subscriber 2 or more 514.14 1,062.25 1,530.99 457.12 943.95Blue Shield Without MedicareSingleAccess HMOSubscriber OnlyYou PayBlue ShieldAccess HMOYou Pay 661.10With MedicareFamily2 PartyFamily1 w 1 w/o MedicareSubscriber 2 or more 1,005.23 1,360.912 PartyFamilySubscriber 1Subscriber 2 or more 1,356.29 1,953.81Single2 PartySubscriber 11 w 1 w/o MedicareSubscriber 2 or more 582.02 1,203.11 1,288.05 1,733.53Subscriber OnlyBlue Shield Without MedicareSingleSpectrum PPOSubscriber OnlyYou Pay1 on Access SingleSubscriber Only 987.38 869.872 Party2 PartyFamilyFamilySubscriber 1Subscriber 2 or more 2,051.33 2,945.72Blue Shield With MedicareSingle2 PartySpectrum PPO Subscriber OnlySubscriber 1Blue Shield rates include medical, ExpressScripts pharmacy and VSP vision coverage.FamilySubscriber OnlyBlue Shield With MedicareSingle2 PartyTrio A.C.O. Subscriber OnlySubscriber 1You PayKaiser rates include medical, pharmacy, and VSPvision coverage.2 Party2 with Medicare1 on TrioYou PayThe following tables summarize theamounts our self-pay subscribers pay fortheir health insurance coverage.SingleSubscriber Only 1,806.642 PartyFamily1 w 1 w/o MedicareSubscriber 2 or more 1,933.83 2,594.82
DentalDelta CareUSA DHMOYou PayDelta DentalNetwork DPPOYou PayDelta DentalIncentiveDPPOYou PaySingle2 PartySubscriber 1Subscriber 2 or more 17.31 28.48 42.09Single2 PartySubscriber 1Subscriber 2 or more 45.81 127.35 173.20Single2 PartySubscriber 1Subscriber 2 or more 57.27 159.19 216.54Subscriber OnlySubscriber OnlySubscriber OnlyFamilyFamilyFamily
Key TermsMedical/General TermsAllowable ChargeOut-of-NetworkBalancing BillingNon-network providers are allowedto charge you more than the plan’sallowable charge. This is calledbalance billing.Services received from yourproviders (doctors, hospitals, etc.)who are not a part of your healthplan’s network. Out-of-networkservices generally cost more thanin-network services. With someplans, such as HMOs and EPOs, outof-network services are notcovered.CoinsuranceOut-of PocketThe most an in-network providercan charge you for an office visit orservice.The cost between you and theinsurance company. Coinsurance isalways a percentage totaling 100%.For example, if the plan pays 70%,you are responsible for 30% of thecost.Healthcare costs you pay using yourown money, whether from yourbank account, credit card, healthreimbursement account (HRA),health savings account (HSA), orflexible spending account (FSA).CopayOut-of-Pocket MaximumThe fee you pay to a provider at thetime of service.DeductibleThe amount you have to pay out-ofpocket for expenses before theinsurance company will cover anybenefits costs for the year (exceptfor preventative care and otherservices where the deductible iswaived).Explanation of Benefits (EOB)The statement you receive from theinsurance carrier that explains howmuch the provider billed, how muchthe plan paid (if any), and howmuch you owe (if any). In general,you should not pay a bill from yourprovider (except copays) until youhave received and reviewed yourEOB.Family DeductibleThe maximum dollar amount anyone family will pay out in individualdeductibles in a year.Individual DeductibleThe dollar amount a member mustpay each year before the plan willpay benefits for covered services.In-NetworkServices received from providers(doctors, hospitals, etc.) who arepart of your health plan’s network.In-network services generally costyou less than out-of-networkservices.18The most you would pay out-ofpocket for covered services in ayear. Once you reach your out-ofpocket maximum, the plan covers100% of eligible expenses.Preventative CareA routine exam, usually yearly, thatmay include a physical exam,immunizations, and test for certainhealth conditions.Prescription TermsDental TermsBrand Name DrugBasic ServicesGeneric DrugDiagnostic and PreventativeServicesA drug sold under its trademarkedname. A generic version of thedrug may be available.A drug that has the same activeingredients as a brand name drug,but is sold under a different name.Generics only become availableafter the patent expires on a brandname drug. For example, Tylenol isa brand name pain relievercommonly sold under its genericname Acetaminophen.Generally includes coverage forfillings and oral surgery.Generally, includes routinecleanings, oral exams, x-rays,sealants, and fluoride treatmentsEndodonticsCommonly known as root canaltherapy.ImplantsA prescription that does not allowfor substitution of an equivalentgeneric or similar brand drug.An artificial tooth root that issurgically placed into your jaw tohold a replacement tooth or bridge.Many dental plans do not coverimplants.Maintenance MedicationsMajor ServicesDispense as Written (DAW)Medications taken on a regular basisfor an ongoing condition such ashigh cholesterol, high bloodpressure, asthma, etc. Oralcontraceptives are also considered amaintenance medication.Non-Preferred Brand DrugA brand name drug for whichalternatives are available fromeither the plan’s preferred branddrug or generic drug list. There isgenerally a higher copayment fornon-preferred brand drugs.Preferred Brand DrugA brand name drug that the planhas selected for its preferred druglist. Preferred drugs are generallychosen based on a combination ofclinical effectiveness and cost.Specialty PharmacyGenerally, includes restorativedental work such as crowns,bridges, dentures, inlays, andonlays.OrthodontiaSome dental plans offer orthodontiaservices for children (andsometimes adults too) to treatalignments of the teeth.Orthodontia services are typicallylimited to a lifetime maximum.PeriodonticsDiagnosis and treatment of gumdisease.Pre-Treatment EstimateAn estimate of how much the planwill pay for treatment. A pretreatment estimate is not aguarantee of payments.Provides special drugs for complexconditions such as multiplesclerosis, cancer, and HIV/AIDSbilling.Step
Kaiser Senior Advantage HMO Rate increase* No changes to medical coverage Kaiser Permanente HMO Rate increase* No changes to medical coverage Members still receive vision coverage through VSP coverages and m Blue Shield 65 Plus HMO Rate increase* No changes to medical coverage Blue Shield Trio ACO HMO Now the lowest costing HMO plan*