Transcription
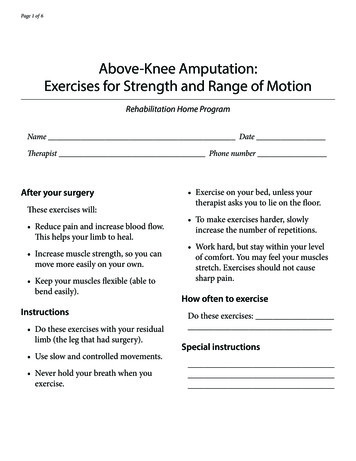
Clinical REVIEWLower limb cellulitis:a dermatological perspectiveSkin disease such as venous eczema and tinea pedis are often overlooked as primary causes of lowerlimb cellulitis. This article will look at the management of these two common skin conditions as wellas the diagnosis and management of lower limb cellulitis. Kilburn et al (2003) acknowledge that thetreatment of cellulitis is multiciplinary stating that no one speciality can claim the condition as theirfield and the Clinical Resource Efficiency Support Team (CREST, 2005) recommend that key staff in anintegrated cellulitis pathway should include dermatologists. The article will give details of a dermatologyled lower-limb cellulitis service which demonstrates a best practice initiative which avoids unecessaryhospitalisation, incorrect diagnoses and also helps to reduce the risk of recurrent cellulitis.Carrie WingfieldKEY WORDSDermatologyLower limb cellulitisVenous eczemaTinea pedisService provisionCellulitis currently accounts for2–3% of hospital admissions(Cox et al, 1998) and is an acute,painful and potentially serious infectionof the skin and subcutaneous tissue(Figure 1), usually involving pathogensStaphylococcus aureus and Streptococcuspyogenes. The average length of inpatientstay for cellulitis is 7.1 days (Departmentof Health [DoH], 2009), a total of30,524 bed days in 2007–2008. Thesefigures do not differentiate which partof the body is affected, but evidencesuggests that lower limb cellulitis isthe most prevalent (Cox et al, 1998;Halpern et al, 2008). Further episodes oftreatment for patients with lower limbcellulitis show that 25–50% have otherassociated morbidity, such as oedema,ulceration and skin disease (Cox et al,1998; Dupuy et al, 1999).Carrie Wingfield is Clinical Lead Senior Nurse ManagerDermatology and Honorary Lecturer, University of EastAnglia, Norfolk and Norwich University Foundation Hospital26WingfieldC.indd 2WoundsUK,Kilburn et al (2003) acknowledge thetreatment of cellulitis as multidisciplinarystating that no one speciality canclaim the condition as their field.Dermatologists often receive tertiaryreferrals to see patients who have beentreated as inpatients on acute medical/surgical wards for lower limb cellulitis.On examination it is not uncommon tofind a differential diagnosis of infectedvenous eczema (Figure 2), or undiagnosedtinea pedis (Figure 3). The consequenceof these skin disorders being overlookedor misdiagnosed and the subsequentneed to treat patients for cellulitis canresult in unnecessary admissions, use ofhospital bed bays, pressure on emergencymedicine resources and the use ofinappropriate intravenous antibiotictherapy. Admission to hospital can bedaunting and unsettling and could alsoplace the patient at risk of hospitalacquired infections and increased risk ofantibiotic resistance (Wingfield, 2008).Both venous eczema and tinea pedisare recognised as risk factors for theopportunistic development of lowerlimb cellulitis.Venous eczema, sometimescalled stasis eczema or varicose eczema islinked to secondary venous hypertension.It is often associated with varicose veins,although they are not always present.Clinical presentation includes pittingoedema, stasis purpura resulting inhaemosiderin deposits, dry itchy skin,Figure 1. Example of lower limb cellulitis.Figure 2. Infected venous eczema with yellowcrusting (impetiginisation).inflammation and induration calledlipodermatosclerosis.The eczema can bemore prominent when coexisting withvenous ulcers (Holden et al, 2004).Tineapedis is a fungal infection presenting mostlyin the interdigital toe web spaces. It is often2009, Vol 5, No 211/6/09 14:47:02
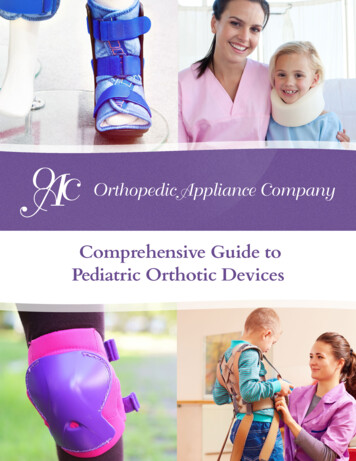
REVIEWClinical PRACTICEClinicalDEVELOPMENTTable 1Comparison of clinical features of varicose (venous) eczema and cellulitis of the legadapted from Quartey-Papafio ory of varicose veins or deepvein thrombosis (DVT)May have pyrexiaPainfulNo relevant historySignsErythematous, inflamedNo tendernessVesiclesCrustingOther lesions on bodyErythematous, inflamedTendernessOne or a few bullaeNo crustingNo other lesionsPortal of entryNot applicableUsually unknown but may be ulcerationor associated skin disease such as eczemaor tinea pedisInvestigationsWhite blood count normalBlood culture negativeSkin swabs — S. aureus commonWhite blood count highBlood culture usually negativeSkin swabs usually negative except fornecrotic tissueFigure 3. Tinea pedis.Figure 4. Venous leg ulcer with secondary cellulitis.asymptomatic and is commonly causedby Trichophyton rubrum, T. mentagrophytesand Epidermophyton floccosum. Handsand toenails may also be involved. Clinicalpresentation includes scaling, maceration,fissuring and erythema in the interdigitalarea (Fleischer et al, 2002). If these skinconditions are diagnosed and treatedappropriately, there is both a possibility ofreducing this risk of developing cellulitisand experiencing recurrent cellulitisepisodes which can lead to chronicoedema.The key objective of this articleis to heighten awareness of the diagnosis,treatment, management and investigationof these common skin conditions aspart of the assessment and diagnosis ofsuspected lower limb cellulitis.Recognising and treating skin diseaseassociated with lower limb cellulitisVenous eczemaIt is extremely important to be ableto differentiate cellulitis from otherdermatological and vascular diagnoses(Quartey-Papafio, 1999; Cox, 2002).Others have concluded that 29% ofpatients develop recurrent lower limbcellulitis within a mean of three years afterthe first episode (Jorup-Ronstrom andBritton, 1987).This is frequently associatedwith existing venous insufficiency withdeveloping or existing venous eczemaand/or venous ulcers which also increasethe prevalence of cellulitis episodes(Jorup-Ronstrom and Britton, 1987)(Figure 4).These conditions are recognisedas risk factors for the entry of ‘infectiveorganisms’ (Dupuy et al, 1999). Cox et al’s(1998) retrospective study identified skindisease/broken skin in 51/92 patients, themost common being minor trauma andtinea pedis.This study was conducted asan audit and held across two hospitals. Itlooked at the case notes of 92 patientsadmitted with a diagnosis of lower limbcellulitis under different adult specialities. Italso concluded that pathogens were rarelyidentified.Quartey-Papafio (1999) identifiedthe issue of misdiagnosis and confusionof cellulitis and venous eczema andhighlighted the clinical difference betweenFigure 5. Lipodermatosclerosis.the two conditions in a simple table(Table 1). This table is a useful assessmenttool when assessing the lower limbfor suspected cellulitis. The absence ofpain is a good indicator that there isno subacute soft tissue infection. Fromclinical experience, any applied pressureor handling of a leg with cellulitis is oftenacutely tender and painful for the patientand they will frequently have difficultybearing weight on the affected leg.Although some discomfort is noted ininfected venous eczema, the pain wouldnot be acute and mobility should notbe affected unless the patient had otherWoundsWingfieldC.indd 3UK,2009, Vol 5, No 22711/6/09 14:47:02
Clinical REVIEW7aFigure 6. Atrophy blanche.painful coexisting conditions, for exampleischaemia, ulceration or lymphoedema.It is important to note that infectedvenous eczema and cellulitis can presenttogether.When diagnosing venous eczema thefollowing signs can be clinically indicative:8 Varicose veins/deep vein thrombosis8 Lipodermatosclerosis (Figure 5), alocalised chronic inflammation of theskin and subcutaneous tissues — a signof severe chronic venous disease8 Atrophy blanche (Figure 6)8 Infection may be evident byyellow crusting or small vesicles(impetiginisation) (Figure 2)8 Hyperpigmentation — skin darkens incolour8 Gravitational eczema(autoeczematisation Figures 7a and7b).This condition sometimes occurswhen venous stasis eczema is presenton the lower legs.The eczema canspread to other parts of the body asan autosensitisation reaction8 Family history of venous disease,history of leg ulceration. Existing orhealed leg ulcer.Examine the rest of the body asuntreated venous eczema may gravitateto the upper thighs, trunk and upper limbs,a phenomenon known as gravitationaleczema (autoeczematisation/Id reaction).The rash often occurs at a site distal to theoriginal onset.The existing venous eczemaon the lower leg acts as a stimulus causinga reaction to the body’s immunologicalresponse (Evans and Bronson, 2009).Assessment and treatment of venous eczema,gravitational eczema and lipodermatoslerosisThe pathophysiology of venous eczema isnot clear. It is classed as an inflammatorydermatoses that responds to emollients28WingfieldC.indd 4WoundsUK,Figure 8. Contact dermatitis — the identifiedallergen in this case is a paste bandage containingparabens.7bFigures 7a and 7b. Gravitational eczema(autoeczematisation/Id reaction).and topical steroids (Quartey-Papafio,1999; Smith, 2006; Middleton, 2007).Inflamed lipodermatosclerosis has a slowresponse to topical treatments and mayrequire use of very potent topical steroids(Duffill, 2008). It is not uncommon forcontact dermatitis to present with venouseczema (Figure 8).The literature showsthat patients with chronic venous legulcers are more prone to sensitisationto topical applications such as creams/ointments, primary dressings and bandages(Barron et al, 2007; Middleton, 2007).There is insufficient evidence on theuse of compression stockings in treatingvenous eczema and lipodermatosclerosis.The general view is that compressionplays an important role in reducingvenous hypertension, therefore improvingand slowing down skin changes whichmay contribute to venous eczema. Legelevation and exercise can improvevenous return and reduce venouspressure and this may help to improvethe skin. However, there is no trialevidence regarding the benefits of theseinterventions (Wounds UK, 2002; Partsch,2003; Barron et al, 2007; Duffill, 2008).The management of infected venouseczema will require skin assessmentand interventions involving frequentapplications of topical treatments suchas corticoid steroids, emollients anddressings. Some patients may needintensified treatment application to bringthe eczema under control. Assessmentwould include exclusion of cellulitis, pain,skin integrity, choice and implementationof topical or systemic therapy. Dailyapplication may be required, in particularif the legs are weeping and dressings havebeen necessary or if the patient is notable to apply their topical treatments. Ifa moderate-to-potent steroid has beenused a review will be required to stepdown the strength according to response.If there is coexisting leg ulceration,redressing of the ulcer may have to beincreased in the short term to access theeczema and treat accordingly.There is little evidence to support theuse of topical antiseptics.The NationalInstitute for Health and Clinical Excellence(2007) recommends that these productscan be used as adjunct therapy to reducebacteria levels on the skin. It advises thattopical and systemic antibiotics should notbe used where no clinical signs of infectionare observed.Tinea pedisTinea pedis, also known as athlete’sfoot (Figure 3), is a dermatophyteinfection and is recognisable as acurable, dermatological primary cause ofrecurrent lower limb cellulitis, but is rarelydiagnosed in clinical areas other thandermatology (Pierce and Daugird, 1992).Tinea pedis affects the interdigital webspace, commonly between the fourthand fifth toe. Cox et al (1998) concludethat the treatment and diagnosis of tinea2009, Vol 5, No 211/6/09 14:47:04
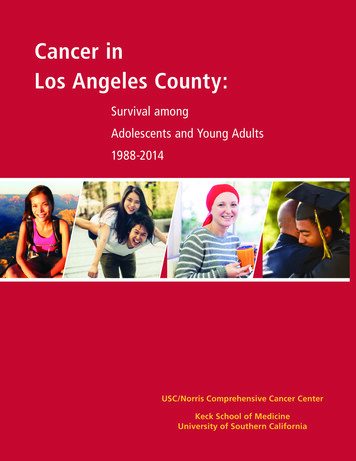
Clinical REVIEWTable 2Management and assessment of infected venous eczema (adapted from NICE, 2007)Characteristics8888Weeping, crusting pustulesFailure to respond to treatmentWorsening eczemaFever/malaiseInterventions/investigation8 Wash skin with a suitable soap substitute at eachdressing change8 Antiseptic emollients can be usefulMedications/treatments8888Daily topical treatment and assessment may be requiredAssess and document the extent of skin surface affectedIf extensive, swab skin and prescribe first-line antibioticsIf the infection responds poorly to antibiotic treatment, considerresults of the swab and treat according to sensitivities, or seekspecialist advice8 If there are localised areas of infection, consider prescribing a topicalantibiotic8 Creams or ointments containing antibiotics can be used as separateproducts or combined with a corticosteroid8 Advise that the ointments should be used for no longer than 7–14 daysand should not be used as a stand-alone therapy for more extensiveinfected eczemaMaintenance8 If not already performed, assess arterial circulation, ankle brachialpressure index (APBI) using a hand-held Doppler8 If the APBI is 0.8, consider compression hosiery once infected eczemahas been treated. APBI should be considered with the patient’s historyand other comorbidties as part of the decision process. If it is 0.8,refer the patient to a vascular surgeon8 Class 2 (medium) hosiery suits most people. Use class 1 (light) if nottolerated. Class 3 (high) may be difficult to tolerate8 Consider topical skin regimen that patient or carers may be ableto continue and sustain and educate the patient about the signs ofinfection/cellulitisEvaluation8 If not responding to treatment, refer to swab results for antibioticsensitivity8 If the condition deteriorates despite correct antibiotic therapy, considercontact dermatitis or inadequate control and refer the patient to adermatologist8 Reassess ongoing management with topical treatment tailored to theindividual8 Issue new topical treatment supplies after the infection istreated and discard old treatment to avoid the possibility of crosscontamination by old suppliespedis in combination with treatmentof chronic oedema, for example withcompression, can reduce subsequentcellulitis episodes. This supports the needfor dermatologist input within a lowerlimb cellulitis pathway (Wingfield, 2008).Dermatophytes are fungi that cancause infections of the skin, hair, and nails.Common dermatophyte infections are30WingfieldC.indd 6WoundsUK,caused by trichophyton, microsporum,and epidermophyton species. Tinea pedisis most commonly due to T rubrum, butalso caused by T interdigitale (ClinicalKnowledge Summary, 2008a). Clinicalsigns are:8 Itching8 Burning8 Irritation over site8 Skin scaling9a9bFigure 9a. Dermapak and size 15 blade fordistribution of tinea pedis. Figure 9b. Fungaltoenails and moccasin skin scrapings/toenailclippings.8 Maceration8 Fissuring.Diagnostic investigations for athlete’sfoot or other fungal skin infections are notalways required if the presenting clinicalpicture is clear. Recommendations are totake skin scrapings for microscopy andculture if the diagnosis is not clear, the skinhas not improved or has deterioratedwith standard topical treatment, or if oralantifungal medication is indicated as firstline treatments have failed or condition isbecoming more widespread (Loo, 2004;Andrews and Burns, 2008). It shouldbe highlighted that microscopy/cultureresults from scrapings and clippings cantake a few weeks to come back.Thereis also a significant false-negative ratefor microscopy and culture.Therefore, anegative result does not always excludefungal infection and the diagnosis mayneed to be made clinically if signs aresignificant (Higgins et al, 2000).Tinea pedis can become moreextensive affecting the plantar and dorsumsurface of the foot; lateral borderscan also be involved giving a moccasindistribution. Fungal toenails (Figure 9b) aresometimes evident and were thought tobe commonly associated with tinea pedis.However, evidence involving a large studyof patients with tinea pedis (n 5,143)showed that only 20% of patients werefound to have coexisting fungal toenails(Burzykowski et al, 2003).2009, Vol 5, No 211/6/09 14:47:05
Clinical REVIEWTable 3Presentation/management of lower limb cellulitisClinical presentationRisk factorsObesityLymphoedemaDiabetesVenous disease/ulcerationPrevious episodes of cellulitisImmunocompromisedIntravenous drug usersSymptomsSpreading erythema (redness)Painful, tender skinHot, swollenBlister or bullaeoPyrexiaMalaise, nausea, rigorsLymphangitis/lymphoedema (Figure 10)Diagnosis/clinical assessmentConsider differentialsIdentify primary cause if possibleSwab if there is an obvious portal of bacterial entryMark any tracking erythema with a skin markerTake baseline observations (refer on if there are two or more signs of sepsis)Biochemistry: the following blood tests although none specific are nearly always elevated in patientswith cellulitis — ESR (erythrocyte sedimentation rate), CRP (C-reactive protein) and WBC (whichblood cell count). Normal results make a diagnosis of cellulitis less likelyCheck lymph glands. They may be swollen, tenderDetermine or initiate investigation or referral if differential diagnosisTake patient history, date of onset, first or recurrent episode of lower limb cellulitisMedications, past history, allergies, social circumstancesIntervention (Class I)If diagnosed as lower limb cellulitis and systemically well, commence high-dose oral antibiotic for 7 daysTreatment: primary careFlucloxacillin (500mg qds)Erythromycin (500 mg qds) — if allergic to penicillinClarithromycin (500mg bd) — if erythromycin not toleratedConsider adding on a second antibiotic if the cellulitis has arisen from a wound contaminated withwater: doxycycline (100mg once a day) for saltwater contamination; ciprofloxacin (750mg twice a day)for freshwater contaminationTreat any co-existing skin condition, venous eczema, tinea pedisAdvise on appropriate analgesia if requiredAdvise to drink plenty of water to avoid dehydrationLeg elevation to ease pain and help reduce swellingReviewAsk patient to contact if symptoms deteriorate in the next seven daysPlan and organise a review appointment to monitor progressAssess skin and any treated skin conditionMonitor erythema markings on review. If erythema is below the original line it is a useful indicatorthat the infection is subsiding. If erythema is spreading above the original line consider referral tosecondary careRepeat baseline observationsDoppler if compression is to be considered and cellulitis resolvedIf the patient has deteriorated consider referral to secondary careIf resolved educate patient to possible cause, and educate to recognise signs and symptoms ofrecurrence and to avoid injury, burns and bitesReferral class II–III refer tosecondary careComplex comorbiditiesFailure to respond to treatment32WingfieldC.indd 8WoundsUK,Refer to secondary care for:Systemically unwell/toxic symptomsFurther investigationUncertain/differential diagnosisAdmissionIntravenous therapyTreatments8 Advise good foot hygiene to patient/carer/nurse and ensure that they drythoroughly between the toes afterwashing8 Treat with a topical imidazole,undecenoate, or terbinafine. Imidazoles:treat for 2–4 weeks to clear thelesions.Terbinafine (adults only): treatfor 1–2 weeks to clear the lesions.Undecenoates (adults only): treat for2–4 weeks to clear the lesions8 Continue topical treatment for 1–2weeks after the skin has healed8 Preparations combining a topicalanti-fungal agent with corticosteroidare usually unnecessary. Considerdoing this if the infection is particularlyinflamed and irritated8 Failure to respond to treatmentand if the condition becomes moreextensive may indicate a need forsystemic treatment. Consider referringthe patient to a dermatologist.Lower limb cellulitis — diagnosisand managementCellulitis is an acute bacterial infectionof the dermis and subcutaneous tissues,and typically affects one limb and is rarelybilateral (Swartz, 2004) (Figure 10). Itis important to make a diagnosis andexclude other differentials such as:8 Deep vein thrombosis8 Infected venous eczema(usually bilateral)8 Erythema nodosum8 Pyoderma gangrenosum8 Vasculitis8 Necrotising fasciitis8 Gangrene8 Acute gout8 Drug reactions8 Metastastic cancer.Assess the limb for possible primarycause, for example:8 Venous eczema8 Tinea pedis8 Trauma8 Ulcerations8 Burn/bites.Take a swab for bacteriology ifappropriate.Assessing the severity of the cellulitisis important as the presence and signs of2009, Vol 5, No 211/6/09 14:47:06
Clinical REVIEWsystemic symptoms may indicate sepsis orosteomylitis which could lead to a speedydeterioration in the patient’s condition.Patients with two or more signs of sepsisshould not be managed in primary careand will require hospital assessment andadmission. Signs of septicaemia include:8 Pyrexia8 Tachycardia8 Increased respiration8 Elevated white blood cell count8 Hypotension8 Reduced urine output8 Diarrhoea8 Cold/clammy8 Confusion/disorientation.Table 3 outlines assessment process,intervention, treatment and recommendedreview for lower limb cellulitis.Grading is recommended usinga classification system from class I–IV(Eron, 2000) (Table 4). Only patientswith Class I cellulitis should remain inprimary care.These patients wouldhave no uncontrolled comorbidities orTable 4Grades of cellulitis (Eron, 2000; CREST, 2005)Key Points8 Cellulitis accounts for 2–3% of allhospital admissions.Figure 10. Lower-limb cellulitis withassociated lymphoedema.systemic symptoms and can be managedwith oral antibiotics (CREST, 2005).Refer to secondary care if diagnosisis not clear or the patient has alreadyreceived first-line antibiotics and isdeteriorating. Other comorbidities maycomplicate the diagnosis and delay healing.These multiplex cases should also beconsidered for referral to secondarycare. Consider routine referral if thepatient is experiencing recurrent episodesof lower limb cellulitis with associatedlymphoedema (Figure 10).LymphoedemaClass IPatients have no signs of systemic toxicity, haveno comorbidities and can usually be managedwith oral antimicrobials as outpatients.Class IIPatients are either systemically ill orsystemically well but with a comorbidity suchas peripheral vascular disease, chronic venousinsufficiency or morbid obesity which maycomplicate or delay resolution of their infection.Class IIIPatients may have a significant systemic upsetsuch as acute confusion, tachycardia, tachypnoea,or may have unstable comorbidities that mayinterfere with a response to therapy, or havea limb-threatening infection due to vascularcompromise.Class IVPatients have sepsis syndrome or severe lifethreatening infection such as necrotising fasciitis.34WingfieldC.indd 10WoundsUK,Recommendations vary for antibiotictherapy in the management of cellulitiswith lymphoedema.The BritishLymphology Society (BLS) recommendsprophylactic antibiotic treatment forpatients who have two or more attacksa year.They have published a consensusdocument giving concise guidance onmanagement and treatment (BritishLymphology Society and LymphoedemaSupport Network, 2007).Following an episode of cellulitis ofthe leg evidence suggests 7% of patientsgo on to develop chronic oedema(lymphoedema), known as secondarylymphoedema (CREST, 2005).The cellulitisinfection causes damage to a previouslyfully functioning lymphatic system. A recenthypothesis suggests a predispositionto cellulitis in patients with previousunpresenting, undiagnosed primarylymphatic abnormality.The cellulitis thencauses further damage and symptomsbecome apparent (Keeley, 2008). Patientswith primary or secondary lymphoedema8 Recurrent episodes of lowerlimb cellulitis can be associatedwith primary skin disease such asvenous eczema and tinea pedisand it is important to treat theseconditions appropriately whenthey are first encountered.8 Venous eczema is oftenmisdiagnosed and treatedas cellulitis.8 The treatment of cellulitis ismultidisciplinary and benefitsfrom the involvement ofdermatologists.are high-risk candidates for recurrentcellulitis due to local immune deficiency(Dupuy et al, 1999).Suggested service provisionand developmentThere is limited evidence-basedresearch supporting dermatology as anappropriate specialist team to manageuncomplicated lower limb cellulitis.However, in the available publishedwork, dermatology is highlighted asbeing a necessary cohort of expertisein the diagnosis and management of thiscondition (CREST, 2005).The common scenario alreadymentioned of patients sitting in hospitalbeds with a misdiagnosis of cellulitishas become a key driver for servicedevelopment in one dermatologydepartment in Norwich. Previously,the majority of cellulitis referrals camethrough either the Emergency AssessmentMedicine Unit (EAUM) or A&E.Tertiary referrals would come into thedermatology department for opinion onrashes or ulcerations for patients admittedto hospital for intravenous therapy.Both the dermatologist and emergencymedicine team realised that patients withlower limb cellulitis were missing out onquick diagnosis of primary skin disease and2009, Vol 5, No 211/6/09 14:47:06
HYDROFIBER CHAL 297x105a:Layout 1 26/05/2009 18:58 Page 1late differential diagnosis was delaying thepatient’s pathway of care.As a direct consequence of this a newsame-day referral outpatient cellulitis clinicwas set up in the dermatology outpatientsdepartment (Wingfield, 2008). GPs using acriteria, can refer lower limb cellulitis casesto this clinic where a thorough assessmentis carried out to include diagnosis/treatment/investigation of any differentialdiagnosis or coexisting skin disease.The patients are seen by a specialistdermatology nurse and a junior doctor.Each new patient is booked into a 90minute assessment slot. Suitable patientsare treated with ceftriaxone intravenoustherapy (IV), a once-a-day antibiotic IVtreatment over a three-day period. Afterreceiving their first administration in clinicthey are discharged with a cannula in situand receive their next two doses at homefrom the community IV team. On day fourthey return to the clinic for review wherethey are stepped down to oral antibioticsover a period of a further 11 days if theirsymptoms are improving.Versiva XC dressinghas a semi-occlusive,low moisture vapourtransmission rate (MVTR)backing preventingAQUACEL dressingfrom drying out.Versiva XC dressing, incorporatingHydrofiber Technology, locks in1 fluid,helping protect periwound skin andreducing the risk of maceration2,3.The benefits of this are:8 Ease of pressure on EAUM resources8 Reduced waiting lists helping toachieve the four-hour target waitin A&E8 Early discharge/preventionof admission8 Patient is not exposed to hospitalacquired infections8 Provision of a faster pathway8 Care in the community.The patientremains closer to home8 Treatment of skin conditions preventsrecurrent episodesof cellulitis.Studies have supported this change ofclinical pathway and management of lowerlimb cellulitis. Seton et al (2005) recognisedhigh standards in nurse-led home IVservices using IV ceftriaxone.Theyconcluded that care is not compromisedand the need for medical review isreduced. Caplan et al (1999) and Corwinet al (2005) state home IV treatment is aseffective as hospital inpatient treatment aswell as being more acceptable to patients.To date, this clinic has seen 500 cases oflower leg cellulitis. Out of this cohort only12 (10.6%) patients have been admittedAQUACEL dressing, incorporatingHydrofiber Technology, creates amoist wound environment to supporthealing and locks-in fluid1, helpingprotect the peri-wound skin andreducing the risk of maceration2,3.References1. Walker M, Hobot JA, Newman GR, Bowler PG. Scanning electron microscopic examination of bacterial immobilisationin a carboxymethyl cellulose (Aquacel) and alginate dressings. Biomaterials. 2003;24(5):883-890.2. Coutts P, Sibbald RG. The effect of a silver-containing Hydrofiber dressing on superficial wound bed and bacterial balanceof Chronic Wounds. Int. Wound J. 2005;2:348-356.UK,3. Robinson BJ. The use of a hydrofibre dressing in wound management. J. Wound Care. 2000;9(1):32-34.Wounds2008, Vol 4, No 4 /TM indicates a trade mark of ConvaTec Inc. ConvaTec Ltd an authorised user. ConvaTec Inc 2009WingfieldC.indd 1135AP-007620-GB11/6/09 14:47:07
Clinical REVIEWto hospital; 76.5% had confirmed cellulitis,23.4% had differential diagnosis, 33.6%had co-existing primary skin disease— either tinea pedis or venous eczema.This has produced a massive saving on beddays offset against the cost of outpatienttreatment. In recognition of this serviceinnovation, the clinic received the HealthEnterprise East Innovation Award in 2008.ConclusionsThe recognition and treatment ofdermatological skin disease in patientspresenting with cellulitis of the lower limbis arguably a crucial part of this condition’smanagement. By treating these primarysources of potential infection, recurrentcases of cellulitis and the risk of chronicoedema can be reduced.Health professionals dealing with thiscondition should include dermatologyknowledge as an important asset for theirown professional practice. Dermatologistsare a useful resource and should becomea necessary part of the patient’s pathwaywhere appropriate.This is supported byimportant recommendations made in theCREST (2005) guidelines stating that keystaff should be identified in an integratedcellulitis pathway with the inclusion ofdermatologists.The establishment ofdermatology-led lower limb clinics insecondary care can greatly improve thepatient’s experience if supported by a wellresourced home IV community team. Allstakeholders need to take ownership ofthis innovation to successfully incorporatean integrated pathway for lower limbcellulitis management. It is recognised thatthe service is only sustainable in largerdermatology departments where there isa full complement of specialist medical andnursing skills and good support from juniordoctors.These clinics will be an ideal basefor evidence-based practice and furtherresearch in the field of cellulitis treatmentand management. WUKReferencesAndrews MD, Burns M (2008) Common tineainfections in children. Am Fam Phys 77(10):1415–20Barron GS, Jacob SE, Kirsner RS (2007)Dermatologic complications of chronic venousdisease: medical m
part of the assessment and diagnosis of suspected lower limb cellulitis. Recognising and treating skin disease associated with lower limb cellulitis Venous eczema It is extremely important to be able to differentiate cellulitis from other dermatological and vascular diagnoses (Quartey-Papafio, 1999; Cox, 2002). Others have concluded that 29% of